You might also like
- PMLS2 Understanding Phlebotomy ReviewerDocument5 pagesPMLS2 Understanding Phlebotomy ReviewerShane G.No ratings yet
- Correlation Serum Ferritin HbA1c Type2 Diabetes Patients Tertiary HealthcareDocument7 pagesCorrelation Serum Ferritin HbA1c Type2 Diabetes Patients Tertiary HealthcareSSR-IIJLS JournalNo ratings yet
- Guest Editorial Biomedical and Health Informatics For DiabetesDocument1 pageGuest Editorial Biomedical and Health Informatics For DiabetesJessy BanegasNo ratings yet
- Difference in The Levels of Ferritin, Hemoglobin, and Erythrocyte Count of Stage 5 Chronic Kidney Disease Patients After One, Three and Six Months of HemodialysisDocument6 pagesDifference in The Levels of Ferritin, Hemoglobin, and Erythrocyte Count of Stage 5 Chronic Kidney Disease Patients After One, Three and Six Months of HemodialysisNaldo NathanNo ratings yet
- 2018 Guidelines For The Management of Dyslipidemia: Correspondence To In-Kyung Jeong, M.DDocument49 pages2018 Guidelines For The Management of Dyslipidemia: Correspondence To In-Kyung Jeong, M.DBramantyo Dwi HandjonoNo ratings yet
- ConsensoLabdiabetes2011 (Sacksetal)Document47 pagesConsensoLabdiabetes2011 (Sacksetal)tere ariasNo ratings yet
- Bocchio Et Al 2022, A RCT Pilot Study To Compare Efficacy of Different Iron FormulationsDocument6 pagesBocchio Et Al 2022, A RCT Pilot Study To Compare Efficacy of Different Iron Formulationsedo adimastaNo ratings yet
- WJH 14 670Document13 pagesWJH 14 670juliomenimssNo ratings yet
- New 6Document1 pageNew 6AMELIA ULMNo ratings yet
- Dgac 185Document2 pagesDgac 185Fifi RetiatyNo ratings yet
- (CHINA, 2011) Adaptation of The Audit of Diabetes-Dependent Quality of Life Questionnaire To People With Diabetes in ChinaDocument8 pages(CHINA, 2011) Adaptation of The Audit of Diabetes-Dependent Quality of Life Questionnaire To People With Diabetes in ChinaINVESTIGACIONES HEINZNo ratings yet
- Coagulation Dynamics Type 2 Diabetes Mellitus Insights PT APTT AssessmentDocument5 pagesCoagulation Dynamics Type 2 Diabetes Mellitus Insights PT APTT AssessmentSSR-IIJLS JournalNo ratings yet
- Gut Microbiota and Diabetic Kidney Diseases Pathogenesis and Therapeutic PerspectivesDocument12 pagesGut Microbiota and Diabetic Kidney Diseases Pathogenesis and Therapeutic PerspectivesClaudia AlessandraNo ratings yet
- Clinchem 00 e 1Document47 pagesClinchem 00 e 1بلال العميسيNo ratings yet
- Journal of Pharmacological and Toxicological Methods: 10.1016/j.vascn.2015.11.004Document59 pagesJournal of Pharmacological and Toxicological Methods: 10.1016/j.vascn.2015.11.004Mela KristantiwiNo ratings yet
- Journal Ke 5Document5 pagesJournal Ke 5StrangersNo ratings yet
- Estimation of Serum Zinc Level in Newly Diagnosed Type 2 Diabetes Mellitus PatientsDocument6 pagesEstimation of Serum Zinc Level in Newly Diagnosed Type 2 Diabetes Mellitus PatientsIJAR JOURNALNo ratings yet
- Anemia and Iron Deficiency in Gastrointestinal and Liver ConditionsDocument19 pagesAnemia and Iron Deficiency in Gastrointestinal and Liver ConditionsOcha24 TupamahuNo ratings yet
- Asociacion Entre Diabetes y Colocacion de Implantes Dentales Revision Sistematica y MetaanalisisDocument11 pagesAsociacion Entre Diabetes y Colocacion de Implantes Dentales Revision Sistematica y MetaanalisisLaura Corrales RicaldezNo ratings yet
- Journal of Applied Health Management and TechnologyDocument12 pagesJournal of Applied Health Management and TechnologyMhd Azland FikryNo ratings yet
- Jurding 2Document8 pagesJurding 2Tiffany Rachma PutriNo ratings yet
- Diabetes Treatment Adherence and Associated Factors in Sub-Saharan Africa: A Systematic Review and Meta-AnalysisDocument13 pagesDiabetes Treatment Adherence and Associated Factors in Sub-Saharan Africa: A Systematic Review and Meta-Analysisijmb333No ratings yet
- Type 2 Diabetes: Annals of Internal MedicineDocument17 pagesType 2 Diabetes: Annals of Internal MedicinenicoolNo ratings yet
- Journal Homepage: - : IntroductionDocument6 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Dgab 636Document10 pagesDgab 636Fifi RetiatyNo ratings yet
- Analysis of Nutrition and Nutritional Status of HaDocument11 pagesAnalysis of Nutrition and Nutritional Status of HaVione rizkiNo ratings yet
- Wild2007 PDFDocument6 pagesWild2007 PDFJavi PatónNo ratings yet
- Nutrients 14 00815 v2Document12 pagesNutrients 14 00815 v2donald duckNo ratings yet
- Folate 2Document25 pagesFolate 2ayham luNo ratings yet
- Comparative Studies of Diabetes in Adult Nigerians Lipid Profile and Antioxidants Vitamins A and CDocument5 pagesComparative Studies of Diabetes in Adult Nigerians Lipid Profile and Antioxidants Vitamins A and CEditor IJTSRDNo ratings yet
- Apical Periodontitis and Diabetes Mellitus Type 2Document11 pagesApical Periodontitis and Diabetes Mellitus Type 2Mihaela TuculinaNo ratings yet
- Serum Calcium Levels in Correlation With GlycatedDocument6 pagesSerum Calcium Levels in Correlation With GlycatedShivpartap SinghNo ratings yet
- Association Between Obesity and Anemia in A Nationally Representative Sample of South Korean Adolescents: A Cross-Sectional StudyDocument8 pagesAssociation Between Obesity and Anemia in A Nationally Representative Sample of South Korean Adolescents: A Cross-Sectional Studyayham luNo ratings yet
- Intermittent Fasting Is There A Role in The Treatment of DiabetesDocument12 pagesIntermittent Fasting Is There A Role in The Treatment of DiabetesluthfianamiftasyafitriNo ratings yet
- Vitamin Dpaper JACNACS2019Document13 pagesVitamin Dpaper JACNACS2019Neider Salazar CaroNo ratings yet
- Effect of Iron Deficiency Anemia On Hemoglobin A1c LevelsDocument6 pagesEffect of Iron Deficiency Anemia On Hemoglobin A1c LevelscandraNo ratings yet
- Pharmaceutical SciencesDocument5 pagesPharmaceutical SciencesiajpsNo ratings yet
- Song 2012Document6 pagesSong 2012Yasser AlghrafyNo ratings yet
- Hypertension and Chronic Kidney Disease in Asian PopulationsDocument6 pagesHypertension and Chronic Kidney Disease in Asian PopulationsBIETRIS WARISYUNo ratings yet
- ERC PotasioDocument10 pagesERC PotasioAbrilNo ratings yet
- TODIAJ 8 13 Lu Diabetes 2018 PDFDocument10 pagesTODIAJ 8 13 Lu Diabetes 2018 PDFغاز الشمالNo ratings yet
- Intravenous Iron For Iron Deficiency Anaemia Full ReportDocument124 pagesIntravenous Iron For Iron Deficiency Anaemia Full ReportSitha DeviNo ratings yet
- 1 s2.0 S2352648324000126 MainDocument46 pages1 s2.0 S2352648324000126 MainCristian ȘtefanNo ratings yet
- Impact of Air and Manual Scaling On Dental Anxiety and Blood Glucose Level Among Diabetic PatientsDocument7 pagesImpact of Air and Manual Scaling On Dental Anxiety and Blood Glucose Level Among Diabetic PatientsDeanita PutriNo ratings yet
- Correlation Between Onset of Diabetes Mellitus and Nitric Oxide Levels in Patient With Type 2 Diabetes MellitusDocument4 pagesCorrelation Between Onset of Diabetes Mellitus and Nitric Oxide Levels in Patient With Type 2 Diabetes MellitusNina DorotheaNo ratings yet
- Effect of Apple Cider Vinegar On Glycemic Control, Hyperlipidemia and Control On Body Weight in Type 2 Diabetes PatientsDocument16 pagesEffect of Apple Cider Vinegar On Glycemic Control, Hyperlipidemia and Control On Body Weight in Type 2 Diabetes PatientsJoseph PositivoNo ratings yet
- Peri Implant Conditions and Levels of Advanced Glycation End Products Among Patients With Different Glycemic ControlDocument7 pagesPeri Implant Conditions and Levels of Advanced Glycation End Products Among Patients With Different Glycemic ControlBagis Emre GulNo ratings yet
- Dental CariesDocument6 pagesDental Cariesyusuf230287No ratings yet
- Anemia in Patients With Type 2 Diabetes MellitusDocument9 pagesAnemia in Patients With Type 2 Diabetes MellitusmitchelNo ratings yet
- Exploration - 2023 - Zhang - The Pharmacology and Therapeutic Role of Cannabidiol in DiabetesDocument10 pagesExploration - 2023 - Zhang - The Pharmacology and Therapeutic Role of Cannabidiol in Diabetesladyzeta16No ratings yet
- Iron Deficiency Anemia in Inflammatory Bowel Disease: Sindhu Kaitha, Muhammad Bashir, Tauseef AliDocument12 pagesIron Deficiency Anemia in Inflammatory Bowel Disease: Sindhu Kaitha, Muhammad Bashir, Tauseef AliWahyu DustnamNo ratings yet
- Ijacm AnemiaDocument7 pagesIjacm Anemiasusanti08No ratings yet
- Prevalensi Gout Tibet ChinaDocument5 pagesPrevalensi Gout Tibet ChinaShared LifeNo ratings yet
- 8 Mansour - Factors - Associated - With - Glycemic - Control - in - Type - 2 - Diabetic - Patients - in - Saudi - ArabiaDocument5 pages8 Mansour - Factors - Associated - With - Glycemic - Control - in - Type - 2 - Diabetic - Patients - in - Saudi - Arabiabangd1f4nNo ratings yet
- ITC Type 2 Diabetes 2019Document16 pagesITC Type 2 Diabetes 2019ALEJANDRO DUEÑAS GUTIERREZNo ratings yet
- Nutrients 12 00878Document13 pagesNutrients 12 00878Ardian AshadiNo ratings yet
- Hemoglobin Targets For The Anemia in Patients With Dialysis Dependent Chronic Kidney Disease A Meta Analysis of Randomized Controlled TrialsDocument10 pagesHemoglobin Targets For The Anemia in Patients With Dialysis Dependent Chronic Kidney Disease A Meta Analysis of Randomized Controlled TrialsDesi MeliaNo ratings yet
- Bmjopen 2015 009088 PDFDocument10 pagesBmjopen 2015 009088 PDFKanesti KamajayaNo ratings yet
- Assessment of The Alteration of Blood Indices in Patients With Type 2 Diabetic Mellitus: A Cross Sectional StudyDocument6 pagesAssessment of The Alteration of Blood Indices in Patients With Type 2 Diabetic Mellitus: A Cross Sectional StudyYanet FrancoNo ratings yet
- Fiber DiabetesDocument8 pagesFiber DiabetesMatthew NathanielNo ratings yet
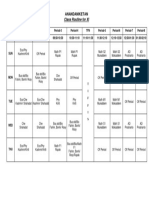
- Class Routine For XI: AnandaniketanDocument1 pageClass Routine For XI: AnandaniketanTawsif MusharofNo ratings yet
- Glycated Haemoglobin (Hba1C) Variations in Nondiabetics With Nutritional AnemiaDocument5 pagesGlycated Haemoglobin (Hba1C) Variations in Nondiabetics With Nutritional AnemiaTawsif MusharofNo ratings yet
- Sreedev Narayanan, Prakruti Dash, Preetam Mahajan: Original ArticleDocument4 pagesSreedev Narayanan, Prakruti Dash, Preetam Mahajan: Original ArticleTawsif MusharofNo ratings yet
- Haemoglobin Electrophoresis in Diagnosing A Case oDocument3 pagesHaemoglobin Electrophoresis in Diagnosing A Case oTawsif MusharofNo ratings yet
- S2 Discrete Distributions - PoissonDocument54 pagesS2 Discrete Distributions - PoissonTawsif MusharofNo ratings yet
- ModifiedPrinciplesofHaematologyLabManual Fall2016 PDFDocument59 pagesModifiedPrinciplesofHaematologyLabManual Fall2016 PDFGwenNo ratings yet
- Minipro Anemia Kelompok 1Document62 pagesMinipro Anemia Kelompok 1Vicia GloriaNo ratings yet
- Lab Report 1 (Hematology)Document8 pagesLab Report 1 (Hematology)Romanda GreeneNo ratings yet
- Beta Thal E DiseaseDocument2 pagesBeta Thal E DiseaseM Asif NaveedNo ratings yet
- Normal Lab ValuesDocument1 pageNormal Lab Valueshurt_y100% (1)
- Liver Function Test (Lft-A)Document4 pagesLiver Function Test (Lft-A)ce mgnregsNo ratings yet
- Acid Elution TestDocument14 pagesAcid Elution Testتجربة أولىNo ratings yet
- NSS KMC: COVID-19 Resource ListDocument21 pagesNSS KMC: COVID-19 Resource ListHarshad MehtaNo ratings yet
- اسئله شائعة ف مقابله المختبر 3 pdfDocument6 pagesاسئله شائعة ف مقابله المختبر 3 pdfAnas ShwbkNo ratings yet
- Contoh Laporan Bulanan LaboratoriumDocument3 pagesContoh Laporan Bulanan LaboratoriumAgataAyuningtyasNo ratings yet
- Haemato PBFDocument7 pagesHaemato PBFNishaNo ratings yet
- Test 1 - PSE Model Answers-1Document3 pagesTest 1 - PSE Model Answers-1Matsiri ImmanuelNo ratings yet
- 11zon Merged PDFDocument10 pages11zon Merged PDFvigneshwaran sugumarNo ratings yet
- Blood Group of AnimalsDocument26 pagesBlood Group of Animals김소정No ratings yet
- 345 - Hematology Physiology) PolycythemiasDocument3 pages345 - Hematology Physiology) PolycythemiasAro DanaNo ratings yet
- Guidelines On The Management of Massive Blood Loss: GuidelineDocument8 pagesGuidelines On The Management of Massive Blood Loss: GuidelineRatna AgustinaNo ratings yet
- Rawalpindi Institute of Cardiology: HaematologyDocument1 pageRawalpindi Institute of Cardiology: HaematologyAabid MehmoodNo ratings yet
- Beta-Thalassemia: Authors: Antonio Cao, MD Renzo Galanello, MDDocument33 pagesBeta-Thalassemia: Authors: Antonio Cao, MD Renzo Galanello, MDUMMID WashimNo ratings yet
- Trima Accel Blood Collection SystemDocument3 pagesTrima Accel Blood Collection SystemIRFAN KHANNo ratings yet
- تقنيات تحاليل الدم 1Document6 pagesتقنيات تحاليل الدم 1hanan modaNo ratings yet
- Prepartion of Blood Smear Hematology PresentationDocument44 pagesPrepartion of Blood Smear Hematology PresentationArslan ArshadNo ratings yet
- Other Major Blood Group SystemsDocument7 pagesOther Major Blood Group SystemsRron de GuzmanNo ratings yet
- Prevalence of Anaemia in Pregnant Women Attending AntenatalDocument19 pagesPrevalence of Anaemia in Pregnant Women Attending Antenatalchebetnaomi945No ratings yet
- Deep Vein ThrombosisDocument103 pagesDeep Vein ThrombosisWildcane SalmeronNo ratings yet
- (Trans) Chapter 16: Anemias - Red Blood Cell Morphology and Approach To DiagnosisDocument4 pages(Trans) Chapter 16: Anemias - Red Blood Cell Morphology and Approach To Diagnosisgotvelvet world dominationNo ratings yet
- Sickle Cell Anemia: By: Salwan Ayad YahyaDocument5 pagesSickle Cell Anemia: By: Salwan Ayad Yahyaأياد المشهدانيNo ratings yet
- Hematology - Oncology - PREP 2021Document46 pagesHematology - Oncology - PREP 2021drthanalla100% (1)
- Max Lab ReportDocument8 pagesMax Lab ReportKallu PrasadNo ratings yet
- Transfusion and Apheresis Science: Ravneet Kaur Bedi, Kshitija Mittal, Tanvi Sood, Rakesh Kumar, Ajay S. PraveenDocument3 pagesTransfusion and Apheresis Science: Ravneet Kaur Bedi, Kshitija Mittal, Tanvi Sood, Rakesh Kumar, Ajay S. PraveenLuis Enrique Tinoco JuradoNo ratings yet