You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Chapter 30 Assessment and Management of Patients With Vascular Disorders and Problems of Peripheral CirculationDocument23 pagesChapter 30 Assessment and Management of Patients With Vascular Disorders and Problems of Peripheral CirculationAbel C. Idusma Jr.No ratings yet
- Unit 1 Biology IAL Past Papers by TopicDocument23 pagesUnit 1 Biology IAL Past Papers by TopicWillie Wong100% (2)
- National Clinical Guidelines For Stroke Fourth EditionDocument232 pagesNational Clinical Guidelines For Stroke Fourth EditionRosa Mabel Sanchez RoncalNo ratings yet
- Medical Devices Regulations and ClassificationsDocument46 pagesMedical Devices Regulations and ClassificationsAhmet Hayri KınacılarNo ratings yet
- Life Sciences Grade 10 Revision Material Term 2 - 2023Document28 pagesLife Sciences Grade 10 Revision Material Term 2 - 2023Linati Dawedi100% (1)
- Red Cross Emergency Care Workbook Answer Key 2012Document36 pagesRed Cross Emergency Care Workbook Answer Key 2012jennybooby100% (1)
- Grand Case Study V7 Final 030310Document49 pagesGrand Case Study V7 Final 030310Jemimah Ruth Madayag ValenzuelaNo ratings yet
- Summary Notes - Topic 1 Edexcel (A) Biology A LevelDocument10 pagesSummary Notes - Topic 1 Edexcel (A) Biology A LevelAmal Abu KhalilNo ratings yet
- Sample Case StudyDocument38 pagesSample Case Studyanon-387573100% (3)
- Journal of Medical Ethics and History of Medicine: Original ArticleDocument11 pagesJournal of Medical Ethics and History of Medicine: Original Articleali sarjunipadangNo ratings yet
- PathophysiologyDocument3 pagesPathophysiologyali sarjunipadangNo ratings yet
- Surgical Procedures: Coronary Artery RevascularizationDocument2 pagesSurgical Procedures: Coronary Artery Revascularizationali sarjunipadangNo ratings yet
- Nursing Process The Patient With Acute Coronary SyndromeDocument3 pagesNursing Process The Patient With Acute Coronary Syndromeali sarjunipadangNo ratings yet
- Promoting Adequate Gas ExchangeDocument5 pagesPromoting Adequate Gas Exchangeali sarjunipadangNo ratings yet
- ReferencesDocument1 pageReferencesali sarjunipadangNo ratings yet
- ReferencesDocument1 pageReferencesali sarjunipadangNo ratings yet
- Olly The Oxygen MoleculeDocument1 pageOlly The Oxygen MoleculeElizabeth CollisNo ratings yet
- Dharam Prakash SaranDocument89 pagesDharam Prakash SarankeerthanaaNo ratings yet
- Transportation in Animals and Plants Worksheet 11 PDFDocument2 pagesTransportation in Animals and Plants Worksheet 11 PDFParul ShahNo ratings yet
- PSSC Biology QPDocument35 pagesPSSC Biology QPAndrew ArahaNo ratings yet
- Study of HypertensionDocument44 pagesStudy of HypertensionMathew PiNo ratings yet
- A Review On The Biomechanics of Coronary ArteriesDocument62 pagesA Review On The Biomechanics of Coronary ArteriesAbhishek KarmakarNo ratings yet
- Cardiovascular Hemodynamic: Mukhammad Dema PrakasaDocument30 pagesCardiovascular Hemodynamic: Mukhammad Dema PrakasayuliaNo ratings yet
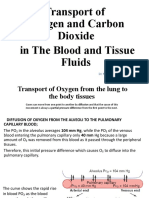
- Transport of Oxygen and Crabon Dioxid in The Blood and Tissue FluidDocument19 pagesTransport of Oxygen and Crabon Dioxid in The Blood and Tissue FluidSAKARIYE MAXAMEDNo ratings yet
- The Circulatory System: (Parts and Functions) Prepared By: Wilfred D. ManingasDocument30 pagesThe Circulatory System: (Parts and Functions) Prepared By: Wilfred D. ManingasAngelica OlivarNo ratings yet
- Peripheral Artery DiseaseDocument8 pagesPeripheral Artery DiseaseDrNadia ZubairNo ratings yet
- Ls2 Elem Las21 To-Las67-MergedDocument47 pagesLs2 Elem Las21 To-Las67-MergedJaypee AturoNo ratings yet
- Term 1 Questions - Life ProcessesDocument30 pagesTerm 1 Questions - Life ProcessesAmbitious StudentNo ratings yet
- UntitledDocument5 pagesUntitledRobin LeeNo ratings yet
- Circulatory System HWDocument2 pagesCirculatory System HWRulani PrinceNo ratings yet
- Human Body Systems Test Study GuideDocument7 pagesHuman Body Systems Test Study GuideJoan JonesNo ratings yet
- Cambridge IGCSE: Biology 0610/13Document16 pagesCambridge IGCSE: Biology 0610/13Saleha ShafiqueNo ratings yet
- Coronary Artery Bypass Grafting: Coronary Bypass Surgery Is An Open-Heart Surgery, You MightDocument17 pagesCoronary Artery Bypass Grafting: Coronary Bypass Surgery Is An Open-Heart Surgery, You MightNuzhat FatimaNo ratings yet
- Gce Marking Scheme: Biology/Human Biology AS/AdvancedDocument29 pagesGce Marking Scheme: Biology/Human Biology AS/Advancedadam wilsonNo ratings yet
- CirculatorySystemSE - Anthony HernandezDocument5 pagesCirculatorySystemSE - Anthony HernandezAnthony Hernandez100% (1)
- Dimension of Development: Health AwarenessDocument46 pagesDimension of Development: Health AwarenessBeverly TogononNo ratings yet
- Target Risk 3: Risk Homeostasis in Everyday LifeDocument235 pagesTarget Risk 3: Risk Homeostasis in Everyday LifeSofia Malgioglio100% (1)