Professional Documents
Culture Documents
Nihms 2
Uploaded by
NUR ATHIFAHOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Nihms 2
Uploaded by
NUR ATHIFAHCopyright:
Available Formats
Health Research Alliance
Member Organization Author Manuscript
Stroke. Author manuscript; available in PMC 2020 May 01.
Published in final edited form as:
Stroke. 2019 May ; 50(5): 1193–1200. doi:10.1161/STROKEAHA.118.023885.
Health Research Alliance Author Manuscript
A brief educational intervention improves emergency medical
services stroke recognition
J. Adam Oostema, MD,
Department of Emergency Medicine, Michigan State University College of Human Medicine,
Secchia Center, 15 Michigan, NE, Grand Rapids, MI 49503, P: 616-234-2732, F: 616-458-4680
Todd Chassee, MD,
Kent County Emergency Medical Services, Grand Rapids, MI
William Baer, MD, PharmD,
Mercy Health St Mary’s Hospital, Grand Rapids, MI
Allison Edberg, DO, and
Metro Health Hospital, Wyoming, MI
Mathew J. Reeves, BVSc, PhD
Michigan State University College of Human Medicine, East Lansing, MI
Abstract
Background and Purpose: Recognition of stroke symptoms and hospital prenotification by
Health Research Alliance Author Manuscript
EMS facilitate rapid stroke treatment, however one-third of stroke patients are unrecognized by
EMS. To promote stroke recognition and quality measure compliant prehospital stroke care, we
deployed a 30-minute online EMS educational module coupled with a performance feedback
system in a single Michigan county.
Methods: Over a 24-month study period, a registry of consecutive EMS transported suspected or
unrecognized stroke cases was utilized to perform an interrupted time series analysis of the impact
of the EMS education and feedback intervention. For each agency, we compared EMS stroke
recognition and quality measure compliance rates, as well as emergency department (ED)
performance and hospital outcomes during 12 pre-intervention months with performance in the
remaining study months.
Results: A total of 1805 EMS-transported cases met inclusion criteria; 1235 (68.4%) of these
had ischemic or hemorrhagic strokes or transient ischemic attacks (TIA). There were no trends
toward improvement in any outcome prior to the intervention. Following the intervention, the EMS
stroke recognition rate increased from 63.8% to 69.5% (p=0.037). Prenotification increased from
60.9 to 77.3% (p<0.001). Among patients with ischemic stroke/TIA, there was a trend toward
higher rates of t-PA delivery (13.9 to 17.7%, p=0.096) and a significant increase in t-PA delivery
Correspondence to: J. Adam Oostema.
Disclosures
The authors have no financial conflicts of interest to report.
Oostema et al. Page 2
within 45 minutes (5.7 to 8.9%, p=0.042) following intervention. However, improvements in EMS
recognition were limited to the first 3 months following intervention.
Conclusions: A brief educational intervention was associated with improved EMS stroke
Health Research Alliance Author Manuscript
recognition, hospital prenotification, and faster t-PA delivery. Gains were primarily observed
immediately following education and were not sustained through provision of performance
feedback to paramedics.
Keywords
Emergency Medical Services (EMS); Quality Improvement; Stroke
Introduction
Over recent years there have been significant advances in the availability of disability-
reducing treatments for ischemic stroke such as intravenous thrombolytics (t-PA) and
endovascular therapy (EVT). However, the efficacy of these treatments is highly time
dependent,1, 2 and they are delivered to a minority of stroke patients.3 Therefore, treatment
guidelines stress the importance of developing coordinated systems of care to reduce time
from stroke symptom onset to treatment. Emergency medical services (EMS) has been
identified as a key component of such systems.4
EMS transportation, compared to arrival by private vehicle, has been associated with earlier
CT scan acquisition, more frequent treatment with t-PA, and reduced time from symptom
onset to t-PA treatment among patients with ischemic stroke.5 These benefits are not
uniformly experienced by all EMS-transported patients; rather, they appear to be linked to
EMS stroke recognition and activation of in-hospital stroke response via prenotification.6–8
Health Research Alliance Author Manuscript
However, EMS recognition is often suboptimal.9–11 Stroke guideline recommendations
promote stroke screen utilization to enhance EMS recognition and encourage expedient
stroke evaluations by minimizing EMS on-scene times and promoting rapid transport and
hospital prenotification.4
Previous analyses have demonstrated strong links between documentation of stroke scales
and more accurate EMS recognition of stroke12, 13 and between EMS recognition of stroke
and the quality of EMS stroke care.8, 11 However, the observational nature of these studies
precludes establishment of a causal relationship. Furthermore, while limited evidence
suggests that EMS stroke knowledge may be enhanced through education14 and that
feedback regarding performance may lead to increased compliance with recommended
prehospital practices,15 no interventional studies have attempted to measure the impact of
changes in EMS practice on the entire continuum of acute stroke care.
Utilizing guideline recommendations,4 baseline EMS performance data from a pilot registry,
8 and feedback from focus groups of local paramedics, we designed and implemented an
educational program to improve EMS stroke recognition. We targeted EMS compliance with
prehospital stroke quality metrics and established a system to provide performance feedback
to paramedics. We then utilized a county-wide registry of EMS transported strokes to
measure the impact of the intervention by comparing the accuracy of EMS stroke
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 3
recognition, the quality of prehospital stroke care, and emergency department (ED) stroke
evaluation and treatment before and after the intervention.
Methods
Health Research Alliance Author Manuscript
Study design
An interrupted time series design was used to examine the impact of EMS education and
initiation of a performance feedback process on EMS stroke recognition, compliance with
quality measures, and hospital-based patient outcomes. The data that support the findings of
this study are available from the corresponding author upon reasonable request.
Setting
The Grand Rapids Area Prehospital Stroke (GRAPHS) study was conducted in a single
county in southwestern Michigan over a 24-month period from July 2015 to June 2017. The
county has a population of approximately 600,000 and is served by three EMS agencies.
Collectively, agencies are staffed by over 400 individual paramedics and provide transport to
approximately 55,000 patients annually. All agencies utilize the Medical Priority Dispatch
System™ dispatch protocols. There are four acute care hospitals in the county with a total of
over 1500 licensed beds, all of which were certified Primary Stroke Centers during the study
period. The Institutional Review Boards of Michigan State University, Spectrum Health,
Mercy Health St. Mary’s, and Metro Health approved the study protocol and provided
waivers of informed consent.
Patients
Patients were eligible for inclusion if they were transported from by one of the three EMS
Health Research Alliance Author Manuscript
agencies from a scene within the study county to one of the 4 hospitals. The final study
population included (1) patients with an EMS primary or secondary impression of stroke or
TIA and (2) EMS-transported patients with a discharge diagnosis of stroke or TIA following
their ED or hospital course who were not recognized by EMS. Patients were excluded if they
were under 18 years of age, transferred from an acute care hospital or freestanding ED,
developed stroke symptoms following hospital arrival, or if prehospital and hospital records
could not be linked.
Data Collection
Patients were identified from two sources. First, EMS suspected stroke cases were identified
by query of each EMS agency’s electronic records for cases with a primary or secondary
impression of stroke or TIA. Patient name, birthdate, and service date were then used to
identify patients within the destination hospital’s electronic medical records. Second, to
capture stroke cases that were unrecognized by EMS, all patients with a hospital discharge
diagnosis of stroke or TIA who arrived by EMS were identified from each hospital’s
discharge database and prehospital records obtained from agencies if not already present. All
data elements were abstracted manually from EMS and hospital records using a standard
electronic abstraction tool. Discharge diagnoses were used to categorize patients as ischemic
stroke (IS), transient ischemic attack (TIA), intracerebral hemorrhage (ICH), subarachnoid
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 4
hemorrhage (SAH), non-traumatic subdural hemorrhage (SDH), or non-stroke (stroke
mimic).
EMS Recognition Categorization
Health Research Alliance Author Manuscript
Cases were classified according to the EMS impression (the provider’s opinion as to the
underlying reason for transport) as recorded in prehospital electronic records. Since EMS
may record both a primary and secondary impression, cases with stroke/TIA in either of
these fields were considered EMS suspected strokes. Cases were considered EMS
recognized (true positives) if they were EMS suspected strokes and the final hospital
diagnosis was stroke (IS, ICH, SAH, SDH) or TIA. Cases were considered EMS overcalls
(false positives) if they were EMS suspected strokes but the final hospital discharge
diagnosis was not stroke. Cases were EMS unrecognized (false negatives) if the EMS
impressions did not include stroke but a final discharge diagnosis of stroke or TIA was
recorded. These designations were used to calculate EMS sensitivity (true positives/all
stroke or TIA cases) and the EMS overcall rate (false positives/all EMS suspected stroke
cases).
Intervention
The intervention was developed to address local performance gaps identified by analysis of a
pilot registry of EMS transported strokes conducted in the same county.8, 12 We conducted
focus groups with paramedics to identify barriers to optimal stroke care, which identified the
diversity of stroke clinical presentations, knowledge deficits regarding the timing and
availability of acute stroke treatments, and the absence of consistent feedback from the
hospitals as primary barriers. Based on this information, we developed a 30-minute, web-
based training module directed at improving stroke-related knowledge and eliminating
Health Research Alliance Author Manuscript
performance gaps. The module consisted of a narrated PowerPoint (Microsoft®, Redmond,
WA) presentation that provided statistics regarding local EMS performance, reviewed
various clinical presentations of stroke, and highlighted EMS stroke quality measures. A
particular focus of the education was on performance and documentation of a Cincinnati
Prehospital Stroke Screen (CPSS)16 for all patients with acute neurological symptoms,
especially among those patients with ambiguous chief complaints such as altered mental
status and dizziness. Furthermore, the presentation emphasized documentation of the last
known well (LKW) time, glucose check, minimizing on-scene time, and hospital
prenotification. To receive credit for training, EMS providers were required to pass a post-
training test with a score of at least 80%.
Completion of the educational module was required of all EMS providers by each agency
over a period of one month. Following completion of training, feedback letters detailing
performance on individual cases were provided to the involved providers every other month.
Feedback included the EMS impression and final discharge diagnosis, performance of EMS
stroke quality measures, door-to-CT (DTCT) times, t-PA delivery, and the final discharge
disposition.
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 5
Statistical Analysis
Descriptive statistics were used to characterize the study population, EMS stroke recognition
rates, prehospital quality measure compliance, DTCT times, t-PA delivery, and hospital
Health Research Alliance Author Manuscript
disposition. Since the intervention was introduced at different times by the agencies, before
and after periods were coded by agency into both dichotomous (before vs after) and
quarterly time epochs. For each agency, the month during which the training occurred was
excluded from analysis.
The primary analysis compared EMS stroke recognition sensitivity and overcall rates before
and after the intervention. Based upon EMS recognition rates in our pilot study,12 a sample
size of 300 stroke cases in each of the two periods was needed to have 80% power to detect
a 10% absolute increase in EMS stroke recognition. Secondary analyses included
comparisons of EMS performance measures such as CPSS, LKW, documentation, on-scene
time ≤15 minutes, and prenotification among all confirmed stroke/TIA patients.4 Since
prehospital stroke scales do not identify stroke with perfect sensitivity, EMS may justifiably
transport stroke cases with a non-stroke impression when cases have a (falsely) negative
screen. To give EMS credit for conducting appropriate screening, we generated a novel
composite endpoint of EMS recognition or stroke screen documentation among hospital-
confirmed stroke/TIA cases. Hospital-based secondary outcomes included DTCT times ≤25
among all confirmed stroke/TIA patients, as well as t-PA delivery and door-to-needle times
≤45 minutes among IS/TIA patients. TIA patients were included in the denominator for the
latter comparisons because of variability in assigning a diagnosis of stroke or TIA to patients
who received t-PA and subsequently had negative brain imaging. Statistical comparisons
were made using chi square tests, Fisher’s exact tests, or Mann Whitney U tests.
Baseline trends in EMS performance and patient outcomes by month during the before
Health Research Alliance Author Manuscript
period were examined using linear regression and chi square tests for trend. Multivariable
logistic regression modelling was used to assess the association between the intervention and
the following outcomes: EMS recognition, hospital prenotification, DTCT ≤25 among
confirmed stroke/TIA patients, t-PA delivery and door-to-needle time (DTNT) within 45
minutes among IS/TIA patients. To account for potential confounding effects of age, sex,
early presentation (LKW to door ≤270 minutes), Glasgow Coma Scale, stroke subtype, and
stroke severity, we undertook a bivariate screening process to examine the independent
association between each variable and each of the 5 outcomes. Covariates that had a
bivariate association (p<0.2) with each outcome were placed into a multivariable model. We
then performed backwards elimination, removing variables with a non-significant (p>0.05)
association.17 Age was forced into all models as an a priori confounder and random
intercepts were used to account for clustering by either EMS agency (prehospital outcomes)
or hospital (hospital-based outcomes).18
Results
During a total of 36 agency-months prior to introduction of the intervention and 30 agency-
months after, 1805 EMS-transported patients met inclusion criteria (Figure 1, Table 1). Of
these, 1235 (67.7%) received a final discharge diagnosis of acute stroke or TIA, and 570
(31.6%) received non-stroke diagnoses. EMS agency volume varied (range 345 to 736) as
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 6
did destination hospital annual stroke volume (range 218 to 927). Ischemic strokes were the
most common subtype of stroke, accounting for over two thirds of strokes while TIA
represented about 17%. Chi square tests for trend did not identify any trends during the
before period in EMS recognition, overcall rates, prehospital quality measures, DTCT times,
Health Research Alliance Author Manuscript
t-PA delivery, or in-hospital mortality (Table 2).
Unadjusted pre vs post-intervention comparisons of primary and secondary outcomes are
summarized in Table 3. There was statistically significant improvement in the primary
outcome of EMS stroke recognition (63.8% before vs. 69.5% after, p=0.037); however, there
was no change in EMS stroke overcall rates (42.1% before vs. 39.9% after, p=0.868). There
was also no statistically significant change in CPSS documentation rates (66.9% before, vs.
67.1% after); however, the composite outcome of EMS recognition or CPSS documentation
increased significantly from 72.1% prior to the intervention to 78.9% after (p=0.006). The
proportion of stroke cases with on-scene times ≤15 minutes increased (37.5% vs 44.3%), yet
there was not an overall improvement in scene times (median 18 minutes before vs. 17 after,
p=0.135) or overall transport times (median 33 before vs. 33.5 after, p=0.314).
Prenotification documentation increased by more than 15% following the intervention;
LKW documentation did not change.
There was also no significant change in the proportion of stroke/TIA patients who received
CT scans within 25 minutes of arrival following intervention, though there was a trend
toward higher rates of t-PA delivery among ischemic stroke/TIA patients and a significant
increase in the proportion of ischemic stroke and TIA patients who received t-PA within 45
minutes of arrival (Table 3). When examining the effect of the intervention over time,
changes in EMS recognition, early CT acquisition, t-PA delivery, and faster DTN times ≤
followed one another closely: increasing during the first quarter following the intervention,
Health Research Alliance Author Manuscript
gradually returning to baseline, and then increasing again in the 4th quarter following
intervention (Figure 2).
Results of the multivariable logistic regression analyses are reported in Table 4. The odds of
EMS recognition were significantly greater in the 1st and 4th post-intervention quarters
compared to baseline (adjusted OR 1.7 and 1.8 respectively). The adjusted odds of
prenotification increased progressively over the post-intervention period. Early CT
acquisition did not increase from baseline during the first quarter following implementation
of the intervention but did increase during the fourth post-intervention quarter. There were
modestly higher odds of t-PA delivery and delivery within 45 minutes during the first two
quarters following the intervention. Results did not change when cases from the final study
quarter were excluded from the regression models. When transporting agency and
destination hospital were treated as fixed effects rather than random effects, point estimates
for the time epoch odds ratios were essentially unchanged, however the p-values for t-PA
delivery and t-PA delivery ≤45 minutes were no longer statistically significant.
Discussion
Following patient or bystander recognition of stroke symptoms, an effective medical
response requires efficient and coordinated systems of care. EMS providers have the
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 7
opportunity to identify potential strokes and facilitate efficient treatment through rapid
transport and activation of an ED stroke response. Indeed, EMS stroke recognition and
hospital prenotification have been linked to faster ED CT scan acquisition and more frequent
and faster t-PA delivery in observational studies.6, 11, 19, 20 However, challenges such as the
Health Research Alliance Author Manuscript
diversity of stroke clinical presentations, absence of standardized EMS stroke education, and
inconsistent communication between hospitals and EMS hinder realization of the full
benefits of acute stroke treatment. We describe the impact of an EMS education and
feedback program designed to address some of these challenges to optimal EMS stroke care.
As far as we are aware, this is the first study to assess the real-world impact of an EMS
training program to enhance prehospital stroke recognition. Overall EMS stroke recognition
(sensitivity) improved significantly following deployment of the educational module.
Moreover, nearly 80% of stroke cases were either recognized as stroke or screened for stroke
by EMS in the post intervention period. This improvement was not accompanied by an
increased overcall rate, which remained stable at around 40%, consistent with other studies.
10, 13, 21 Sensitivity gains were not maintained uniformly over the study period despite
provision of regular performance feedback to providers. During the first quarter following
education, EMS recognition of stroke increased, followed by a gradual return to baseline
rates over the 2nd and 3rd post-intervention quarters. Although there was a resurgence in
sensitivity during 4th post-intervention quarter, this appears to be driven primarily by the fact
that a preponderance of cases during that quarter were transported by the highest performing
agency (supplemental table).
In addition to recognition of stroke symptoms, the educational intervention encouraged
compliance with three prehospital quality metrics for stroke: LKW documentation,
minimization of on-scene times (goal ≤15 minutes), and hospital prenotification. Despite a
Health Research Alliance Author Manuscript
modest improvement in scene time goal compliance, overall transport times remained
unchanged. Interestingly, marked improvement in prenotification documentation was
observed, but this was not accompanied by earlier CT acquisition. This finding contrasts
with observational data that suggest a strong association between prenotification and DTCT
times.6, 22 There may be several explanations for this. It may be that the magnitude of
prenotification improvement was insufficient to result in detectable DTCT time gains.
Furthermore, prenotification documentation is not a required field in EMS records. Thus, the
prenotification improvement may merely represent changes in documentation rather than
practice. Finally, the content of prenotification was not specified by EMS documentation,
which prevents comparisons between notifications that specifically mentioned stroke and
those that did not. The finding that quarterly trends in early CT acquisition closely mirrored
those of EMS recognition (Figure 2) implies that EMS recognition may be the true driver of
faster ED stroke response, presumably by means of stroke-specific prenotification. Further
study of this phenomenon is needed.
On the other hand, we found a trend toward higher rates of t-PA delivery among the
ischemic stroke/TIA population and a statistically significant increase in t-PA delivery
within 45 minutes in the post-intervention period—despite the absence of such trends over
the pre-intervention period. Since DTCT times, which are more proximate to EMS arrival,
did not improve, it may be that DTN time gains were due to hospital-based quality
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 8
improvement efforts. However, data from the Michigan Stroke Registry suggests that
variation in DTCT times is not a primary source of variation in DTN times, a finding which
is probably explained by the consistently low DTCT times that most hospitals have
achieved.23 The similarity between quarterly trends in EMS recognition and t-PA delivery
Health Research Alliance Author Manuscript
overall as well as delivery within 45 minutes (Figure 2) suggests that prehospital
identification of stroke by may have a positive impact on t-PA delivery, even if it does not
operate primarily through faster CT acquisition.
Sustainability of clinical practice change is a common challenge in implementation science
and one that is inadequately researched,24 particularly in the prehospital setting.25 Despite
evidence of improvement in EMS care following implementation of a feedback system in
Rhode Island,15 the individualized audit and feedback system employed in our study did not
sustain improvement. There may be several reasons for this. First, feedback was provided on
all transported cases (strokes and overcalls). Since overcalls were common (32%), feedback
on these cases may have unintentionally discouraged paramedics from labeling patients as a
stroke. Second, feedback may have been ignored or not carefully reviewed due to lack of
performance-based incentives. Third, performance feedback was provided on a case by case
basis rather than providing cumulative or aggregate performance for benchmarking. Finally,
the time required for case ascertainment and abstraction introduced delays between transport
and feedback delivery.
Limitations
Several limitations to this study should be noted. While a before and after design was the
most practical in our context, this design is susceptible to bias since underlying temporal
trends or competing interventions initiated by hospitals may produce misleading results.
26, 27 We attempted to mitigate this by analyzing trends in outcomes for a period of 12
Health Research Alliance Author Manuscript
months prior to implementation by adjusting epoch-specific effects for confounders and
clustering by agency or hospital. Another limitation is that our intervention did not
specifically target emergency dispatcher stroke recognition. Since dispatchers frequently
identify stroke28 and dispatcher stroke recognition may positively influence EMS
recognition,29 their inclusion in the intervention might have enhanced or helped sustain
gains in prehospital recognition. Also, because EMS stroke recognition and quality measure
compliance were abstracted from EMS documentation, changes in documentation might not
reflect true changes in behavior. Furthermore, while our study was powered to detect a
difference in EMS stroke recognition, it was underpowered to detect differences in
uncommon events such as t-PA delivery. Finally, as a pilot project conducted in one
relatively small geographical region, generalizability of our findings cannot be assumed. All
medical transports in our predominantly urban/suburban county are staffed by at least one
paramedic. This makes extrapolation of our results to areas with different EMS staffing
models or more rural locations somewhat uncertain.
Conclusions
We present an analysis of the impact of an education and feedback process on EMS stroke
recognition, quality measure compliance, and ED stroke care. Our findings suggest that
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 9
EMS stroke recognition and quality measure compliance may be significantly influenced by
a brief educational intervention without a concurrent increase in EMS stroke overcalls.
These improvements appear to positively impact the prompt delivery of thrombolytic
therapy to appropriate candidates. However, case-by-case provision of feedback to
Health Research Alliance Author Manuscript
paramedics regarding EMS care and hospital outcomes did not sustain these improvements
over time. Future studies should explore methods to preserve improvements in prehospital
care. These might include faster turnaround for feedback, personalized benchmarking, and
performance incentives at the individual paramedic or agency level.
Supplementary Material
Refer to Web version on PubMed Central for supplementary material.
Acknowledgements
The authors wish to acknowledge Linsey Ouellette, MPH, Keeonna Gordon, BS, and Emily Plachta, MSN, RN,
SCRN, for their significant efforts in abstracting data for this study.
Funding
This project was supported by an American Heart Association Mentored Clinical and Population Research Award
(15MCPRP24470121).
References
1. Emberson J, Lees KR, Lyden P, Blackwell L, Albers G, Bluhmki E, et al. Effect of treatment delay,
age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute
ischaemic stroke: A meta-analysis of individual patient data from randomised trials. The Lancet.
2014;384:1929–1935
2. Saver JL, Goyal M, van der Lugt A, Menon BK, Majoie CB, Dippel DW, et al. Time to treatment
Health Research Alliance Author Manuscript
with endovascular thrombectomy and outcomes from ischemic stroke: A meta-analysis. JAMA.
2016;316:1279–1288 [PubMed: 27673305]
3. Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, et al. Heart disease and stroke
statistics-2017 update: A report from the american heart association. Circulation. 2017;135:e146–
e603 [PubMed: 28122885]
4. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. 2018
guidelines for the early management of patients with acute ischemic stroke: A guideline for
healthcare professionals from the american heart association/american stroke association. Stroke.
2018;49:e46–e110 [PubMed: 29367334]
5. Ekundayo OJ, Saver JL, Fonarow GC, Schwamm LH, Xian Y, Zhao X, et al. Patterns of emergency
medical services use and its association with timely stroke treatment: Findings from get with the
guidelines-stroke. Circulation: Cardiovascular Quality and Outcomes. 2013;6:262–269 [PubMed:
23633218]
6. Lin CB, Peterson ED, Smith EE, Saver JL, Liang L, Xian Y, et al. Patterns, predictors, variations,
and temporal trends in emergency medical service hospital prenotification for acute ischemic stroke.
Journal of the American Heart Association. 2012;1:e002345 [PubMed: 23130167]
7. Kim DH, Nah HW, Park HS, Choi JH, Kang MJ, Huh JT, et al. Impact of prehospital intervention on
delay time to thrombolytic therapy in a stroke center with a systemized stroke code program. J
Stroke Cerebrovasc Dis. 2016;25:1665–1670 [PubMed: 27067887]
8. Oostema JA, Nasiri M, Chassee T, Reeves MJ. The quality of prehospital ischemic stroke care:
Compliance with guidelines and impact on in-hospital stroke response. J Stroke Cerebrovasc Dis.
2014;23:2773–2779 [PubMed: 25312034]
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 10
9. Ramanujam P, Guluma KZ, Castillo EM, Chacon M, Jensen MB, Patel E, et al. Accuracy of stroke
recognition by emergency medical dispatchers andparamedics—san diego experience. Prehospital
Emergency Care. 2008;12:307–313 [PubMed: 18584497]
10. Jia J, Band R, Abboud ME, Pajerowski W, Guo M, David G, et al. Accuracy of emergency medical
Health Research Alliance Author Manuscript
services dispatcher and crew diagnosis of stroke in clinical practice. Front Neurol. 2017;8:466
[PubMed: 28959230]
11. Abboud ME, Band R, Jia J, Pajerowski W, David G, Guo M, et al. Recognition of stroke by ems is
associated with improvement in emergency department quality measures. Prehosp Emerg Care.
2016;20:729–736 [PubMed: 27246289]
12. Oostema JA, Konen J, Chassee T, Nasiri M, Reeves MJ. Clinical predictors of accurate prehospital
stroke recognition. Stroke. 2015;46:1513–1517 [PubMed: 25922507]
13. Mould-Millman NK, Meese H, Alattas I, Ido M, Yi I, Oyewumi T, et al. Accuracy of prehospital
identification of stroke in a large stroke belt municipality. Prehosp Emerg Care. 2018:1–9
14. Oser CS, McNamara MJ, Fogle CC, Gohdes D, Helgerson SD, Harwell TS. Educational outreach
to improve emergency medical services systems of care for stroke in montana. Prehospital
Emergency Care. 2010;14:259–264 [PubMed: 20095821]
15. Choi B, Tsai D, McGillivray CG, Amedee C, Sarafin J-A, Silver B. Hospital-directed feedback to
emergency medical services improves prehospital performance. Stroke. 2014;45:2137–2140
[PubMed: 24876080]
16. Kothari R, Pancioli A, Liu T, Brott T, Broderick J. Cincinnati prehospital stroke scale:
Reproducibility and validity. Ann Emerg Med. 1999;33:373–378 [PubMed: 10092713]
17. Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic
regression. Source code for biology and medicine. 2008;3:17 [PubMed: 19087314]
18. Austin PC. Estimating multilevel logistic regression models when the number of clusters is low: A
comparison of different statistical software procedures. The International Journal of Biostatistics.
2010;6:16
19. Prabhakaran S, O’Neill K, Stein-Spencer L, Walter J, Alberts MJ. Prehospital triage to primary
stroke centers and rate of stroke thrombolysis. JAMA Neurology. 2013;70:1126–1132 [PubMed:
23817961]
20. Patel MD, Rose KM, O’Brien EC, Rosamond WD. Prehospital notification by emergency medical
Health Research Alliance Author Manuscript
services reduces delays in stroke evaluation. Stroke. 2011;42:2263–2268 [PubMed: 21659638]
21. Medoro I, Cone DC. An analysis of ems and ed detection of stroke. Prehospital Emergency Care.
2017;21:476–480 [PubMed: 28339314]
22. Rostanski SK, Shahn Z, Elkind MSV, Liberman AL, Marshall RS, Stillman JI, et al. Door-to-
needle delays in minor stroke: A causal inference approach. Stroke. 2017;48:1980–1982 [PubMed:
28536170]
23. Sauser K, Levine DA, Nickles AV, Reeves MJ. Hospital variation in thrombolysis times among
patients with acute ischemic stroke: The contributions of door-to-imaging time and imaging-to-
needle time. JAMA Neurol. 2014;71:1155–1161 [PubMed: 25023407]
24. Wiltsey Stirman S, Kimberly J, Cook N, Calloway A, Castro F, Charns M. The sustainability of
new programs and innovations: A review of the empirical literature and recommendations for
future research. Implementation science: IS. 2012;7:17 [PubMed: 22417162]
25. Fishe JN, Crowe RP, Cash RE, Nudell NG, Martin-Gill C, Richards CT. Implementing prehospital
evidence-based guidelines: A systematic literature review. Prehosp Emerg Care. 2018:1–9
26. Ramsay CR, Matowe L, Grilli R, Grimshaw JM, Thomas RE. Interrupted time series designs in
health technology assessment: Lessons from two systematic reviews of behavior change strategies.
Int J Technol Assess Health Care. 2003;19:613–623 [PubMed: 15095767]
27. Eccles M, Grimshaw J, Campbell M, Ramsay C. Research designs for studies evaluating the
effectiveness of change and improvement strategies. Quality & safety in health care. 2003;12:47–
52 [PubMed: 12571345]
28. Clawson JJ, Scott G, Gardett I, Youngquist S, Taillac P, Fivaz C, et al. Predictive ability of an
emergency medical dispatch stroke diagnostic tool in identifying hospital-confirmed strokes. J
Stroke Cerebrovasc Dis. 2016;25:2031–2042 [PubMed: 27256173]
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 11
29. Oostema JA, Chassee T, Reeves M. Emergency dispatcher stroke recognition: Associations with
downstream care. Prehosp Emerg Care. 2018:1–6
Health Research Alliance Author Manuscript
Health Research Alliance Author Manuscript
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 12
Health Research Alliance Author Manuscript
Figure 1:
Flow diagram describing case ascertainment and classification. ED=Emergency Department;
TIA=transient ischemic attack
Health Research Alliance Author Manuscript
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 13
Health Research Alliance Author Manuscript
Health Research Alliance Author Manuscript
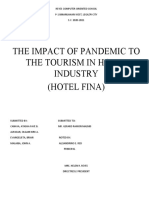
Figure 2:
EMS recognition and hospital outcomes by study quarter. (A) The proportion of 1235
stroke/TIA cases recognized by EMS and who received CT scans within 25 minutes of
hospital arrival. (B) The proportion of 1056 ischemic stroke/TIA cases who received t-PA
and t-PA within 45 minutes. EMS=emergency medical services; DTCT=door-to-CT;
DTNT=door-to-needle-time
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 14
Table 1:
Characteristics of Included Patients
Health Research Alliance Author Manuscript
Total Before After
p-value
N=1805 (%) n=1012 (%) n=793 (%)
Agency-Months 66 36 30
Demographics
Median Age (IQR) 75 (61 to 85) 74 (61 to 85) 74 (61 to 86) 0.788
Female 1032 (57.2) 576 (59.0) 456 (57.5) 0.803
Race/Ethnicity 0.002
Caucasian 1135 (62.9) 597 (59.0) 538 (67.8)
African American 150 (8.3) 87 (8.6) 63 (7.9)
Hispanic/Latino 37 (2.0) 24 (2.4) 13 (1.6)
Asian/Pacific Islander 19 (1.1) 9 (0.9) 10 (1.3)
Other/Missing 464 (25.7) 295 (29.2) 169 (21.3)
Hospital 0.001
1 927 (51.4) 499 (49.3) 428 (54.0)
2 241 (13.4) 163 (16.1) 78 (9.8)
3 419 (23.2) 233 (23.0) 186 (23.5)
4 218 (12.1) 117 (11.6) 101 (12.7)
Agency <0.001
1 724 (40.1) 451 (44.6) 273 (34.4)
2 736 (40.8) 403 (39.8) 333 (42.0)
3 345 (19.1) 158 (15.6) 187 (23.6)
Characteristics
Health Research Alliance Author Manuscript
Non-Stroke Final Diagnosis 570 (31.6) 321 (31.7) 249 (31.4) 0.885
Confirmed Strokes 1235 (68.4) 691 (68.3) 544 (68.6) 0.885
Ischemic Stroke 851 (47.1) 458 (45.3) 393 (49.6) 0.002
Transient Ischemic Attack 205 (11.4) 139 (13.7) 66 (8.3)
Intracerebral hemorrhage 142 (7.9) 71 (7.0) 71 (9.0)
Subarachnoid Hemorrhage 25 (1.4) 17 (1.7) 8 (1.0)
Non-traumatic subdural 12 (0.7) 6 (0.9) 6 (1.1)
Median NIHSS (IQR) 5 (2 to 12) 5 (2 to 12) 5 (2 to 12) 0.775
Discharged Home 887 (49.1) 498 (49.2) 389 (49.1) 0.948
In-hospital Mortality/Hospice 153 (8.5) 81 (8.0) 65 (9.1) 0.416
IQR=interquartile range
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 15
Table 2:
Trends in EMS and hospital performance outcomes during the 12-month before period.
Health Research Alliance Author Manuscript
Outcomes Regression Coefficient* p-value**
EMS Recognized 0.0012 0.818
Recognized or CPSS Documented 0.0027 0.758
EMS Overcall −0.0061 0.584
CPSS Documented 0.0075 0.142
LKW Documentation 0.0061 0.539
Scene Time ≤ 15 minutes −0.0114 0.227
Hospital Prenotification Documented −0.0060 0.259
DTCT Time ≤ 25 minutes 0.0024 0.657
t-PA Delivery (if IS/TIA) 0.0026 0.517
DTNT ≤ 45 minutes (if IS/TIA) 0.0000 0.991
Mortality −0.0011 0.759
EMS=emergency medical services; CPSS=Cincinnati prehospital stroke scale; LKW=last known well; DTCT=door-to-CT; IS/TIA=ischemic
stroke/transient ischemic attack
*
Linear regression coefficient for the proportion of cases with each outcome over 1-month time intervals;
**
chi square test for trend
Health Research Alliance Author Manuscript
Stroke. Author manuscript; available in PMC 2020 May 01.
Oostema et al. Page 16
Table 3:
Unadjusted comparison of EMS performance and hospital outcomes Among 1235 EMS Transported Stroke
Health Research Alliance Author Manuscript
and TIA Patients before and after the intervention.
EMS Performance Before n=691 (%) After n=544 (%) p-value
Dispatch for Stroke 372 (53.8) 316 (58.2) 0.126
EMS Recognized (Sensitivity) 441 (63.8) 378 (69.5) 0.037
EMS Overcall (False Positive Rate) 321 (42.1)* 249 (39.7)* 0.363
CPSS Documented 463 (66.9) 365 (67.1) 0.930
EMS Recognized or CPSS Documented 499 (72.2) 115 (78.9) 0.006
LKW Documented 468 (67.6) 359 (65.9) 0.555
Scene Time ≤ 15 Minutes 260 (37.5) 241 (44.3) 0.018
Hospital Prenotification Documented 422 (60.9) 421 (77.3) <0.001
Hospital Performance
DTCT Time ≤ 25 Minutes 297 (43.0) 250 (46.0) 0.296
t-PA Delivery (among 1056 IS/TIA) 83 (13.9) 81 (17.7) 0.096
DTNT ≤ 45 Minutes (among 1056 IS/TIA) 34 (5.7) 41 (8.9) 0.042
Mortality 80 (11.6) 64 (12.0) 0.841
EMS=emergency medical services; CPSS=Cincinnati prehospital stroke scale; LKW=last known well; DTCT=door-to-CT; IS/TIA= ischemic
stroke/transient ischemic attack; DTNT=door-to-needle time
*
Based on EMS suspected strokes (n=762 before and n=627 after)
Health Research Alliance Author Manuscript
Stroke. Author manuscript; available in PMC 2020 May 01.
Health Research Alliance Author Manuscript Health Research Alliance Author Manuscript
Table 4:
Unadjusted and adjusted logistic regression analyses demonstrating the odds of each outcome given transport during the specified post-intervention time
epoch, compared to the before period.
EMS Recognition (Sensitivity) Hospital Prenotification DTCT ≤25 Minutes t-PA Delivery t-PA ≤45 Minutes
Oostema et al.
Outcome*
Adjusted Adjusted Adjusted Adjusted
Unadjusted OR Adjusted Unadjusted Unadjusted Unadjusted Unadjusted
Time Epoch OR (95% OR (95% OR (95% OR (95%
(95% CI) † OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI)
OR (95% CI) † ‡ § §
CI) CI) CI) CI)
Before 1.0 (Ref) 1.0 (Ref) 1.0 (Ref) 1.0 (Ref) 1.0 (Ref) 1.0 (Ref) 1.0 (Ref) 1.0 (Ref) 1.0 (Ref) 1.0 (Ref)
1.6 1.7 1.5 1.7 1.3 1.0 1.5 1.4 1.9 1.6
1st Quarter
(1.1–2.3) (1.3–2.2) (1.1–2.2) (1.2–2.5) (0.91.7) (0.7–1.5) (1.8–2.4) (0.9–2.1) (1.0–3.5) (1.3–2.1)
1.1 1.4 2.0 2.3 1.0 0.9 1.3 1.4 1.4 1.4
2nd Quarter
(0.8–1.6) (0.9–2.0) (1.4–3.0) (0.9–5.9) (0.7–1.4) (0.5–1.9) (0.7–2.2) (1.2–1.6) (0.6–3.0) (0.9–2.4)
1.0 1.0 2.4 2.5 0.8 0.7 1.1 1.0 1.6 1.4
3rd Quarter
(0.7–1.5) (0.7–1.6) (1.6–3.7) (1.5–4.1) (0.6–1.2) (0.5–1.1) (0.6–1.9) (0.7–1.4) (0.8–3.2) (0.8–2.3)
1.9 1.8 38.5 6.7 2.2 1.7 1.4 0.9 1.5 1.0
4th Quarter
(1.0–3.5) (1.4–2.2) (5.3–279.5) (4.7–9.6) (1.3–3.8) (1.3–2.3) (0.6–3.0) (0.5–1.6) (0.5–4.3) (0.3–3.6)
EMS= emergency medical services; DTCT=door-to-CT; OR=odds ratio; CI=confidence interval; Bolt typeface indicates p<0.05
*
EMS recognized, hospital prenotification, and DTCT time ≤25 minutes analyses conducted among all stroke and TIA patients (n=1235); t-PA delivery and t-PA ≤45 minutes analyses conducted among
1056 confirmed ischemic stroke/TIA patients
†
Adjusted for age, early arrival, NIHSS, stroke subtype, and clustering by agency
‡
Adjusted for age, early arrival, NIHSS, stroke subtype, and clustering by hospital
§
Adjusted for age, NIHSS, and clustering by hospital
Stroke. Author manuscript; available in PMC 2020 May 01.
Page 17
You might also like
- Empirical Research Methods For Software EngineeringDocument24 pagesEmpirical Research Methods For Software EngineeringsarfraznawazbrohiNo ratings yet
- Understanding Magnetic Flux Leakage Test PDFDocument386 pagesUnderstanding Magnetic Flux Leakage Test PDFMayra Lizeth Mayorga LaguadoNo ratings yet
- Critical Success Factors For Digitalization ProjecDocument10 pagesCritical Success Factors For Digitalization ProjecChiraz RosaNo ratings yet
- Swot Analysis PROJECTDocument52 pagesSwot Analysis PROJECTDipanjan Das100% (2)
- Home Reading Intervention PlanDocument15 pagesHome Reading Intervention Plannoel bandaNo ratings yet
- Case Study On FoggDocument4 pagesCase Study On Foggadijalan50% (2)
- International MarketingDocument146 pagesInternational MarketingKelly95% (38)
- Group 3 ThesisDocument19 pagesGroup 3 ThesisSVPS100% (1)
- EWS Dan KESELAMATAN PASIEN - 20072019Document63 pagesEWS Dan KESELAMATAN PASIEN - 20072019ayu100% (2)
- Hon-2020-How Well Do Ems Providers Predict IntDocument14 pagesHon-2020-How Well Do Ems Providers Predict IntDereje BayissaNo ratings yet
- EMS Management of Acute Stroke-Prehospital Triage (Resource Document To NAEMSP Position Statement)Document6 pagesEMS Management of Acute Stroke-Prehospital Triage (Resource Document To NAEMSP Position Statement)Allencia NauweNo ratings yet
- System Delay and Mortality Among Patients With STEMI Treated With Primary Percutaneous Coronary InterventionDocument9 pagesSystem Delay and Mortality Among Patients With STEMI Treated With Primary Percutaneous Coronary InterventionRazika MarissaNo ratings yet
- Jcs 9 13Document7 pagesJcs 9 13kampret berbagiNo ratings yet
- Accepted Manuscript: The American Journal of CardiologyDocument26 pagesAccepted Manuscript: The American Journal of CardiologyYuni IndrianiNo ratings yet
- Ta 0000000000002555Document24 pagesTa 0000000000002555Vivian Ayte LopezNo ratings yet
- Use of A Modified Early Warning Score System To Reduce The Rate of In-Hospital Cardiac ArrestDocument6 pagesUse of A Modified Early Warning Score System To Reduce The Rate of In-Hospital Cardiac ArrestPuspa AmandatyNo ratings yet
- Prehospital Care of Traumatic Brain InjuryDocument6 pagesPrehospital Care of Traumatic Brain Injuryaffa_lechyNo ratings yet
- Broderick 2015Document4 pagesBroderick 2015Jimmy SilverhandNo ratings yet
- 1 s2.0 S0736467903001987 Mainemt - MedDocument6 pages1 s2.0 S0736467903001987 Mainemt - MedJamison ParfittNo ratings yet
- Jamasurgery Spaite 2019Document11 pagesJamasurgery Spaite 2019smith.kevin1420344No ratings yet
- Developing A Therapeutic Approach Toward Active Engagement For Veterans With Mild Traumatic Brain Injury (Tapia Et Al., 2019)Document9 pagesDeveloping A Therapeutic Approach Toward Active Engagement For Veterans With Mild Traumatic Brain Injury (Tapia Et Al., 2019)T4H ResearchNo ratings yet
- 708 FullDocument8 pages708 FullHidayadNo ratings yet
- What Do Our Nurses Know About Managing Patient With Permanent Pacemakers? Muhamad Al Muizz Ismail, Nor Marini Ibrahim and Muhammad Kamil Che HasanDocument5 pagesWhat Do Our Nurses Know About Managing Patient With Permanent Pacemakers? Muhamad Al Muizz Ismail, Nor Marini Ibrahim and Muhammad Kamil Che Hasanyuliana muinNo ratings yet
- Ews1 PDFDocument7 pagesEws1 PDFLivianadrNo ratings yet
- Emergency Medical Services Intervals and Survival in Trauma Assessment of The Golden Hour in A North American Prospective CohortDocument27 pagesEmergency Medical Services Intervals and Survival in Trauma Assessment of The Golden Hour in A North American Prospective Cohortnageur2017No ratings yet
- Godfrey Act RCT 2019Document27 pagesGodfrey Act RCT 2019torrischan199No ratings yet
- Ni Hms 725829Document19 pagesNi Hms 725829SabariaNo ratings yet
- Menopausal Hormone Therapy and The Incidence of Carpal Tunnel Syndrome in Postmenopausal Women: Findings From The Women's Health InitiativeDocument15 pagesMenopausal Hormone Therapy and The Incidence of Carpal Tunnel Syndrome in Postmenopausal Women: Findings From The Women's Health InitiativeDwiky YuanasikaNo ratings yet
- Circulationaha 110 971044Document11 pagesCirculationaha 110 971044mukhlis akmalNo ratings yet
- Schmidt 2016Document19 pagesSchmidt 2016castroailen29No ratings yet
- American Heart Journal Plus: Cardiology Research and PracticeDocument6 pagesAmerican Heart Journal Plus: Cardiology Research and Practice18ME045No ratings yet
- 2013 - STEMI - Future Strategies - LancetDocument14 pages2013 - STEMI - Future Strategies - LancetMichail PapafaklisNo ratings yet
- Abrahams 2018Document33 pagesAbrahams 2018FlorinaNo ratings yet
- Artigo Mobilização PrecoceDocument9 pagesArtigo Mobilização PrecoceLuciana AlexandreNo ratings yet
- Accepted Manuscript: American Journal of Emergency MedicineDocument26 pagesAccepted Manuscript: American Journal of Emergency MedicineRober MerazNo ratings yet
- Meningkatkan Keselamatan Pasien Dalam Deteksi Dini Perburukan Kondisi Fisiologis Pasien Menggunakan National Early Warning Score (NEWS)Document12 pagesMeningkatkan Keselamatan Pasien Dalam Deteksi Dini Perburukan Kondisi Fisiologis Pasien Menggunakan National Early Warning Score (NEWS)Alma AlmiraNo ratings yet
- SepsisScreenTreatmentAlgorithm BaylorUMedicalCenter PDFDocument66 pagesSepsisScreenTreatmentAlgorithm BaylorUMedicalCenter PDFFanie BeatriceNo ratings yet
- Grosse-Sundrup2012 Score PredictifDocument2 pagesGrosse-Sundrup2012 Score PredictifZinar PehlivanNo ratings yet
- DR Srinath Meadipudi: MBBS, FRCP EdinDocument50 pagesDR Srinath Meadipudi: MBBS, FRCP EdincatolgaNo ratings yet
- Sequeira 2016Document7 pagesSequeira 2016WELLINGTON VASCONCELOSNo ratings yet
- UC Irvine: Western Journal of Emergency Medicine: Integrating Emergency Care With Population HealthDocument13 pagesUC Irvine: Western Journal of Emergency Medicine: Integrating Emergency Care With Population HealthARINANo ratings yet
- Adekuate Symtome and KnowlageDocument7 pagesAdekuate Symtome and KnowlageYustina Ni Putu YusniawatiNo ratings yet
- Efectividad de La Fisio en EspasticidadDocument58 pagesEfectividad de La Fisio en EspasticidadAbner SánchezNo ratings yet
- Health Research AllianceDocument14 pagesHealth Research AlliancenadaNo ratings yet
- Circulationaha 110 971044Document11 pagesCirculationaha 110 971044Jemina GuenevereNo ratings yet
- Bunemann (2020)Document10 pagesBunemann (2020)Nerea AlvarezNo ratings yet
- E000349 FullDocument12 pagesE000349 FullZulfa AlfaniaNo ratings yet
- SuccessfulImplementationNIHSS2006 PDFDocument7 pagesSuccessfulImplementationNIHSS2006 PDFMaryoma HabibyNo ratings yet
- ECG in Low Risk PatientsDocument8 pagesECG in Low Risk PatientsSondang JasmineNo ratings yet
- Sree Raj 2016Document6 pagesSree Raj 2016amilyapraditaNo ratings yet
- Journal Pre-Proof: Eres, JadrankaDocument25 pagesJournal Pre-Proof: Eres, JadrankaDiana Magnavita MouraNo ratings yet
- CRITIQUE REVIEW (New)Document6 pagesCRITIQUE REVIEW (New)Anita De GuzmanNo ratings yet
- Coach 2023Document11 pagesCoach 2023Guilherme CarelliNo ratings yet
- Acad Emerg Med 2007 p1114Document6 pagesAcad Emerg Med 2007 p1114Handris SupriadiNo ratings yet
- Seymour-2017-Delays From First Medical ContactDocument14 pagesSeymour-2017-Delays From First Medical ContactDereje BayissaNo ratings yet
- Bagui PsicossocialDocument56 pagesBagui PsicossocialjackNo ratings yet
- Jamainternal Thiruganasambandamoorthy 2020 Oi 200011Document8 pagesJamainternal Thiruganasambandamoorthy 2020 Oi 200011meganNo ratings yet
- Emergency Medical Services Intervals and Survival in Trauma: Assessment of The "Golden Hour" in A North American Prospective CohortDocument16 pagesEmergency Medical Services Intervals and Survival in Trauma: Assessment of The "Golden Hour" in A North American Prospective CohortrutnomleniNo ratings yet
- Outcome Predictors of Acute Stroke Patients in Need of Intensive Care TreatmentDocument8 pagesOutcome Predictors of Acute Stroke Patients in Need of Intensive Care TreatmentAstrid CarolineNo ratings yet
- Journal Reading SarafDocument10 pagesJournal Reading SarafRifa RoazahNo ratings yet
- Long 2017Document33 pagesLong 2017Fabio Antonio Villadiego FontanillaNo ratings yet
- CRITIQUE REVIEW (New)Document7 pagesCRITIQUE REVIEW (New)Anita De GuzmanNo ratings yet
- Ewss PDFDocument6 pagesEwss PDFChintia Meliana Kathy SiraitNo ratings yet
- Stroke Scales and Trajectory of Recovery A Major Concern For Patients and Nurses AlikeDocument7 pagesStroke Scales and Trajectory of Recovery A Major Concern For Patients and Nurses AlikeAnonymous XO9RqHhOgiNo ratings yet
- Fang Impact of Emergency Medical Technician Configurations On Outcomes of Patients in Cardiac ArrestDocument12 pagesFang Impact of Emergency Medical Technician Configurations On Outcomes of Patients in Cardiac ArrestJamison ParfittNo ratings yet
- Predictive Analytics Healthcare BayesianDocument28 pagesPredictive Analytics Healthcare BayesianlauNo ratings yet
- Main 25Document6 pagesMain 25pokharelriwaj82No ratings yet
- Manual of Austere and Prehospital UltrasoundFrom EverandManual of Austere and Prehospital UltrasoundBenjamin D. NicholsonNo ratings yet
- Research PPT Sa PotatoDocument29 pagesResearch PPT Sa PotatoTrisha Mae BahandeNo ratings yet
- Prevalence and Risk Factors For Myopia in Second-Grade Primary School Children in Taipei: A Population-Based StudyDocument8 pagesPrevalence and Risk Factors For Myopia in Second-Grade Primary School Children in Taipei: A Population-Based StudyRosaliaNo ratings yet
- Al Azawei Et Al 2017Document23 pagesAl Azawei Et Al 2017Nath ZuletaNo ratings yet
- Mid Term Report of ISTDDocument2 pagesMid Term Report of ISTDAlma ToppoNo ratings yet
- Effect of Organizational Culture On Delay in Construction PDFDocument12 pagesEffect of Organizational Culture On Delay in Construction PDFashikNo ratings yet
- Mth3340 2017jan - Lab Spss ReportDocument2 pagesMth3340 2017jan - Lab Spss ReportglNo ratings yet
- Research Methods 2020-2021Document27 pagesResearch Methods 2020-2021Daban AbdwllaNo ratings yet
- Chapter 22 HW AnswersDocument19 pagesChapter 22 HW Answersapi-247483889No ratings yet
- Laili 2018 PDFDocument11 pagesLaili 2018 PDFIka MentariNo ratings yet
- Basic Audit 2017Document51 pagesBasic Audit 2017DikaRPertiwiNo ratings yet
- Worked Examples of Non-Parametric TestsDocument22 pagesWorked Examples of Non-Parametric TestsCollins MuseraNo ratings yet
- 54 January 456 PDFDocument18 pages54 January 456 PDFSidhi SoodNo ratings yet
- KCU 200-Statistics For Agriculture-Notes.Document115 pagesKCU 200-Statistics For Agriculture-Notes.treazeragutu365No ratings yet
- Chulalongkorn University: Visiting/Free Mover Student Application Form (Non-Degree)Document4 pagesChulalongkorn University: Visiting/Free Mover Student Application Form (Non-Degree)Ledi Wakha WakhaNo ratings yet
- Lectnotemat 5Document346 pagesLectnotemat 5HassanNo ratings yet
- (Asce) Co 1943-7862 0000751Document8 pages(Asce) Co 1943-7862 0000751ilhamNo ratings yet
- Chapter 2: Strategic Management and Project Selection: Learning ObjectivesDocument14 pagesChapter 2: Strategic Management and Project Selection: Learning ObjectivesJeng AndradeNo ratings yet
- Experimental Design Lec 2Document25 pagesExperimental Design Lec 2Sara HussienNo ratings yet
- StatstiDocument1 pageStatstihiamnshuNo ratings yet
- City Premier CollegeDocument10 pagesCity Premier CollegeAnonymous g7uPednINo ratings yet
- Chapter 03 Us 7eDocument46 pagesChapter 03 Us 7eMuhammad SaefiNo ratings yet