You might also like
- Saccharomyces Boulardii in Helicobacter Pylori Eradication in Children, A Randomized Trial From IranDocument5 pagesSaccharomyces Boulardii in Helicobacter Pylori Eradication in Children, A Randomized Trial From IranJUAN SEBASTIAN AVELLANEDA MARTINEZNo ratings yet
- Nutrients 11 00376 With CoverDocument17 pagesNutrients 11 00376 With CoverMartínez Lozano Ana GabrielaNo ratings yet
- Lactobacillus GG in The Prevention of Nosocomial Gastrointestinal and Respiratory Tract InfectionsDocument9 pagesLactobacillus GG in The Prevention of Nosocomial Gastrointestinal and Respiratory Tract InfectionsImran A. IsaacNo ratings yet
- Soal 2Document9 pagesSoal 2TessaRestianiNo ratings yet
- Public Health: Letter To The EditorDocument2 pagesPublic Health: Letter To The EditorFebie DevinaNo ratings yet
- Candida-Induced Oral Epithelial Cell Responses: E.A. Lilly, J.E. Leigh, S.H. Joseph, & P.L. Fidel JRDocument9 pagesCandida-Induced Oral Epithelial Cell Responses: E.A. Lilly, J.E. Leigh, S.H. Joseph, & P.L. Fidel JRJusty GuavaNo ratings yet
- Oral Care Interventions and Oropharyngeal Colonization in Children Receiving Mechanical VentilationDocument12 pagesOral Care Interventions and Oropharyngeal Colonization in Children Receiving Mechanical VentilationAdila amalitaNo ratings yet
- JURNALDocument9 pagesJURNALIKA 79No ratings yet
- Two Methods of Cord Care in High-Risk Newborns: Their Effects On Hydration, Temperature, PH, and Floras of The Cord AreaDocument12 pagesTwo Methods of Cord Care in High-Risk Newborns: Their Effects On Hydration, Temperature, PH, and Floras of The Cord AreaFatma ElzaytNo ratings yet
- Article WMC004489Document8 pagesArticle WMC004489dyahayueNo ratings yet
- Probiotics and Oral DiseaseDocument3 pagesProbiotics and Oral DiseasechytatoNo ratings yet
- Nadt14i1p8 PDFDocument8 pagesNadt14i1p8 PDFnurharyanti darmaningtyasNo ratings yet
- Beneficial Effects of A Mouthwash Containing An Antiviral Phthalocyanine Derivative On The Length of Hospital Stay For COVID 19: Randomised TrialDocument10 pagesBeneficial Effects of A Mouthwash Containing An Antiviral Phthalocyanine Derivative On The Length of Hospital Stay For COVID 19: Randomised TrialtvinteNo ratings yet
- Agus K LarobuDocument9 pagesAgus K LarobuAgus LarobuNo ratings yet
- Mouth Care To Reduce Ventilator Associated.22Document7 pagesMouth Care To Reduce Ventilator Associated.22heartbcglNo ratings yet
- Lingual Bony ProminencesDocument9 pagesLingual Bony ProminencesAgustin BiagiNo ratings yet
- MicroDocument9 pagesMicroMafe SuarezNo ratings yet
- J CLP 2010 05 003Document15 pagesJ CLP 2010 05 003Rofifa EvaNo ratings yet
- Impact of Oral Hygiene Involving Toothbrushing Versus Chlorhexidine in The Prevention of Ventilator-Associated Pneumonia A Randomized StudyDocument9 pagesImpact of Oral Hygiene Involving Toothbrushing Versus Chlorhexidine in The Prevention of Ventilator-Associated Pneumonia A Randomized StudyAlessandra Rocha PedrozaNo ratings yet
- Immediate Effects and Safety of High-Frequency Chest Wall Compression Compared To Airway Clearance Techniques in Non-Hospitalized Infants With Acute Viral BronchiolitisDocument9 pagesImmediate Effects and Safety of High-Frequency Chest Wall Compression Compared To Airway Clearance Techniques in Non-Hospitalized Infants With Acute Viral BronchiolitisBelén María Vega AladueñaNo ratings yet
- Rhinopharyngeal Retrograde Clearance Induces Less Respiratory Effort and Fewer Adverse Effects in Comparison With Nasopharyngeal Aspiration in Infants With Acute Viral BronchiolitisDocument7 pagesRhinopharyngeal Retrograde Clearance Induces Less Respiratory Effort and Fewer Adverse Effects in Comparison With Nasopharyngeal Aspiration in Infants With Acute Viral Bronchiolitismariane bezerraNo ratings yet
- Neocon 2017Document71 pagesNeocon 2017Jasleen KaurNo ratings yet
- Lactobacillus Salivarius NK02 A Potent Probiotic For ClinicalDocument11 pagesLactobacillus Salivarius NK02 A Potent Probiotic For ClinicalHossein ShahbaniNo ratings yet
- Effects of Lactobacillus Bulgaricus in Soyghurt On Inhibition of Adhesion Klebsiella Pneumoniae Strains in HEp-2 Cell LinesDocument6 pagesEffects of Lactobacillus Bulgaricus in Soyghurt On Inhibition of Adhesion Klebsiella Pneumoniae Strains in HEp-2 Cell Linesprimayaa4758No ratings yet
- American Journal of Infection ControlDocument6 pagesAmerican Journal of Infection ControlAuliasari SiskaNo ratings yet
- In Vitro Beneficial Effects of Streptococcus Dentisani As PotentialDocument10 pagesIn Vitro Beneficial Effects of Streptococcus Dentisani As PotentialValentina Villanueva nietoNo ratings yet
- Attachment 1Document10 pagesAttachment 1Ara MariNo ratings yet
- Antibiotics 11 00757 v2Document16 pagesAntibiotics 11 00757 v2chaandNo ratings yet
- Jurnal Anak Bibir Sumbing - PDF 5Document5 pagesJurnal Anak Bibir Sumbing - PDF 5Bella Adinda N.SNo ratings yet
- Wabe NT 2011Document7 pagesWabe NT 2011Agus PrimaNo ratings yet
- Asian Paci Fic Journal of Tropical BiomedicineDocument7 pagesAsian Paci Fic Journal of Tropical BiomedicineAlexandru Codrin-IonutNo ratings yet
- Bacillus Clausii As Adjunctive Treatment For Acute Community-Acquired Diarrhea 2019 PDFDocument9 pagesBacillus Clausii As Adjunctive Treatment For Acute Community-Acquired Diarrhea 2019 PDFAMIT JAINNo ratings yet
- Kovachev 2014Document7 pagesKovachev 2014habibNo ratings yet
- Characterization of Bacterial Isolates Cultured From The Nasopharynx of Children With Sickle Cell Disease (SCD)Document10 pagesCharacterization of Bacterial Isolates Cultured From The Nasopharynx of Children With Sickle Cell Disease (SCD)International Medical PublisherNo ratings yet
- DX y Tto de Infecciones Por H. Pylori en Niños y Poblaciones MayoresDocument9 pagesDX y Tto de Infecciones Por H. Pylori en Niños y Poblaciones MayoresGerman Andres SomoyarNo ratings yet
- Avhad (2020), Comparison of Effectiveness of Chlorine Dioxide Mouthwash and Chlorhexidine Gluconate Mouthwash in Reduction of Oral Viral Load in Patients With COVID-19Document6 pagesAvhad (2020), Comparison of Effectiveness of Chlorine Dioxide Mouthwash and Chlorhexidine Gluconate Mouthwash in Reduction of Oral Viral Load in Patients With COVID-19Phuong ThaoNo ratings yet
- Helicobacter Pylori Infection in ChildrenDocument11 pagesHelicobacter Pylori Infection in ChildrenCarolina VillagarayNo ratings yet
- Microbiology and Management of Odontogenic InfectionsDocument5 pagesMicrobiology and Management of Odontogenic InfectionsJeninNo ratings yet
- 693 FullDocument12 pages693 FullGilmer alvarez floresNo ratings yet
- PDF 8Document8 pagesPDF 8Justy GuavaNo ratings yet
- GuptaDocument7 pagesGuptaAdit TaufikNo ratings yet
- Mouth Care To Reduce Ventilator Associated.22Document7 pagesMouth Care To Reduce Ventilator Associated.22ANOOPVANo ratings yet
- Research Journal of Pharmaceutical, Biological and Chemical SciencesDocument6 pagesResearch Journal of Pharmaceutical, Biological and Chemical SciencesSurajit SahaNo ratings yet
- S. aureus role in sinusitisDocument6 pagesS. aureus role in sinusitisAnada KaporinaNo ratings yet
- Journal 3Document11 pagesJournal 3margareth silaenNo ratings yet
- Diagnosis and Treatment of Helicobacter Pylori Infections in Children and Elderly PopulationsDocument9 pagesDiagnosis and Treatment of Helicobacter Pylori Infections in Children and Elderly PopulationsAhmedNo ratings yet
- Chronic Periodontitis ReuteriDocument11 pagesChronic Periodontitis ReuteriMUNAZNo ratings yet
- Suppression of Streptococcus Mutans and Candida Albicans by Probioticsan in Vitro StudyDocument8 pagesSuppression of Streptococcus Mutans and Candida Albicans by Probioticsan in Vitro StudyTahir AliNo ratings yet
- SinusitisDocument14 pagesSinusitisdr Rizaldi AbesyNo ratings yet
- Streptococcus Mutans in Denture Stomatitis Patients Under Antifungal TherapyDocument7 pagesStreptococcus Mutans in Denture Stomatitis Patients Under Antifungal TherapyFebrian ArdwiantoNo ratings yet
- 1 1 71Document8 pages1 1 71Medical JournalNo ratings yet
- Comprehensive Oral Care Program For Intubated Intensive Care Unit PatientsDocument15 pagesComprehensive Oral Care Program For Intubated Intensive Care Unit PatientsnurharyantidarmaningtyasNo ratings yet
- Jurnal 1Document9 pagesJurnal 1Maharani Zahra FitriNo ratings yet
- Saudi Pharmaceutical JournalDocument8 pagesSaudi Pharmaceutical JournalSardono WidinugrohoNo ratings yet
- 7225-Article Text for Production-20461-1-10-20231016Document12 pages7225-Article Text for Production-20461-1-10-20231016grovy90No ratings yet
- TurquiaDocument8 pagesTurquiaanselmopesquisa2769No ratings yet
- JURNAL Cefaclor Vs Amoxicillin in The Treatment of AcuteDocument8 pagesJURNAL Cefaclor Vs Amoxicillin in The Treatment of Acuterichard gunturNo ratings yet
- Jurnal Eliminating Risk IntubeDocument14 pagesJurnal Eliminating Risk IntubewilmaNo ratings yet
- Anesthesia in A Patient With Reactive Airways Case FileDocument2 pagesAnesthesia in A Patient With Reactive Airways Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Teaching Care PlanDocument2 pagesTeaching Care Planapi-544206685No ratings yet
- Skills LabDocument2 pagesSkills LabJessa Mae BarquillaNo ratings yet
- N116-Skills Performance Checklist: Tracheostomy SuctioningDocument3 pagesN116-Skills Performance Checklist: Tracheostomy SuctioningAlessandra Dominique MarianoNo ratings yet
- SOP For Covid-19 Liendak Rev 2Document14 pagesSOP For Covid-19 Liendak Rev 2guruNo ratings yet
- Exercise LabDocument3 pagesExercise LabJonatan LeflerNo ratings yet
- Bringing Balasana To Your Body and MindDocument5 pagesBringing Balasana To Your Body and Mindיְפֵהפִיָה רפאלNo ratings yet
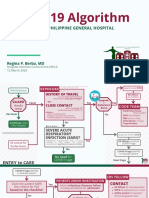
- COVID-19 Algorithm: For The Philippine General HospitalDocument10 pagesCOVID-19 Algorithm: For The Philippine General HospitalJay VeeNo ratings yet
- Recognition of Critically Ill ChildDocument58 pagesRecognition of Critically Ill ChildEmpat patimahNo ratings yet
- Trauma Thorax 2Document73 pagesTrauma Thorax 2----No ratings yet
- When To Suction: Swedish or Artificial Nose (HME)Document2 pagesWhen To Suction: Swedish or Artificial Nose (HME)Liezl Mae MacaraegNo ratings yet
- Safety Data Sheet: Blue DyeDocument13 pagesSafety Data Sheet: Blue DyeAsh BuzNo ratings yet
- Material Safety Data Sheet: Identification of The Material and Supplier 1Document5 pagesMaterial Safety Data Sheet: Identification of The Material and Supplier 1Geo IonNo ratings yet
- Respiratory Physiology & NeurobiologyDocument5 pagesRespiratory Physiology & NeurobiologynimaaandmNo ratings yet
- E-Z WELD PIPE CLEANER SDSDocument2 pagesE-Z WELD PIPE CLEANER SDSVinith KumarNo ratings yet
- CBSE Class 11 Biology Chapter 17 Notes on Breathing and Exchange of GasesDocument8 pagesCBSE Class 11 Biology Chapter 17 Notes on Breathing and Exchange of Gasesfast-track for n2021No ratings yet
- Abdominalassessment PDFDocument29 pagesAbdominalassessment PDFChurrizo IslamiNo ratings yet
- Scoring Systems in Anesthesia and PACUDocument16 pagesScoring Systems in Anesthesia and PACUmissyaaaaNo ratings yet
- ID Hubungan Lingkar Pinggang Dengan FrekuenDocument8 pagesID Hubungan Lingkar Pinggang Dengan FrekuenNurul AlifahNo ratings yet
- Consent FormDocument1 pageConsent FormJulius CagampangNo ratings yet
- Sugammadex Associated Anaphylaxis Summary And.777Document5 pagesSugammadex Associated Anaphylaxis Summary And.777Gabriela TeránNo ratings yet
- 7.4 Gas Exchange in Plants and Animals 2Document3 pages7.4 Gas Exchange in Plants and Animals 2yiuzz hcyNo ratings yet
- COVID 19 Prevention Strategies for Healthcare WorkersDocument31 pagesCOVID 19 Prevention Strategies for Healthcare WorkersPuteriNo ratings yet
- OXYGEN CYLINDER USE AND CAREDocument23 pagesOXYGEN CYLINDER USE AND CAREpriyanka0% (1)
- (Template) BEED CHAPTER 3 MODULE 3 - Sci 1Document6 pages(Template) BEED CHAPTER 3 MODULE 3 - Sci 1Regilyn GalasNo ratings yet
- Basics of Mechanical VentilationDocument5 pagesBasics of Mechanical Ventilationruhaina malikNo ratings yet
- Science: Quarter 1 - Module 1: Respiratory and Circulatory Systems, Working With Other Organ SystemsDocument27 pagesScience: Quarter 1 - Module 1: Respiratory and Circulatory Systems, Working With Other Organ SystemsSofia Rose Saniel Gonzales100% (1)
- Confined-Space-Entry ProcedureDocument18 pagesConfined-Space-Entry ProcedureMayur100% (1)
- Chapter One: 1.4.1 General ObjectiveDocument3 pagesChapter One: 1.4.1 General ObjectivejohnNo ratings yet
- SHERWIN WILLIAMS-Macropoxy Part B-6401-25027-SDSDocument13 pagesSHERWIN WILLIAMS-Macropoxy Part B-6401-25027-SDSjcrenteriajimenezNo ratings yet