You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- NeurogenicbladdermanagementwithcompleteurethraldistructionDocument11 pagesNeurogenicbladdermanagementwithcompleteurethraldistructionPutri Rizky AmaliaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Outcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisDocument7 pagesOutcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisPutri Rizky AmaliaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Controversial TopicDocument11 pagesControversial TopicPutri Rizky AmaliaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Multiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Document14 pagesMultiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Putri Rizky AmaliaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Peterson 2012Document5 pagesPeterson 2012Putri Rizky AmaliaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Role of Rhinitis in Laryngitis: Another Dimension of The Unified AirwayDocument6 pagesRole of Rhinitis in Laryngitis: Another Dimension of The Unified AirwayPutri Rizky AmaliaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Rhinitis Allergy and ElderlyDocument26 pagesRhinitis Allergy and ElderlyPutri Rizky AmaliaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- prm/2018/11 4/prm 11 4 prm170481/prm 11 prm170481Document9 pagesprm/2018/11 4/prm 11 4 prm170481/prm 11 prm170481Putri Rizky AmaliaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- HHS Public Access: 236 Children With Developmental Hydrocephalus: Causes and Clinical ConsequencesDocument22 pagesHHS Public Access: 236 Children With Developmental Hydrocephalus: Causes and Clinical ConsequencesPutri Rizky AmaliaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Literature Reading Short StatureDocument34 pagesLiterature Reading Short StaturePutri Rizky AmaliaNo ratings yet
- Post Partum ComplicationDocument29 pagesPost Partum ComplicationPutri Rizky AmaliaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Healthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidenceDocument9 pagesHealthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidencePutri Rizky AmaliaNo ratings yet
- Doctor Patient RelationshipDocument21 pagesDoctor Patient RelationshipPutri Rizky AmaliaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Half-Life of Infusion Fluids An Educational ReviewDocument8 pagesThe Half-Life of Infusion Fluids An Educational ReviewPutri Rizky AmaliaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Epos Summary PDFDocument30 pagesEpos Summary PDFPutri Rizky AmaliaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
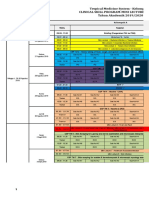
- Jadwal Perkulihanan THN 4 2019-2020 TM-FMDocument20 pagesJadwal Perkulihanan THN 4 2019-2020 TM-FMPutri Rizky AmaliaNo ratings yet
- Ob MidtermDocument5 pagesOb MidtermSheila Tolentino-BelanioNo ratings yet
- 10Document19 pages10Bruno100% (3)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Risk Assessment: Severity (1, 2 or 3)Document1 pageRisk Assessment: Severity (1, 2 or 3)Ulviyye ElesgerovaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Chitale Dairy Uses RFID To Improve MilkYieldsDocument6 pagesChitale Dairy Uses RFID To Improve MilkYieldsAnnaNo ratings yet
- Manual Steamvection ThermasolDocument6 pagesManual Steamvection ThermasolJosse RuizNo ratings yet
- Worksheet Normal Distribution PDFDocument3 pagesWorksheet Normal Distribution PDFJustin Eduard MarzanNo ratings yet
- Mental Health Resources - OrganizedDocument39 pagesMental Health Resources - OrganizedGabrielle Costello-GuerraNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Msds CatDocument7 pagesMsds CatraniNo ratings yet
- Stress Management Stress Management: NptelDocument99 pagesStress Management Stress Management: NptelDKNo ratings yet
- Paper7 Syl22 Dec23 Set2 SolDocument20 pagesPaper7 Syl22 Dec23 Set2 SolAkash AgarwalNo ratings yet
- Benchmark Report 2011Document80 pagesBenchmark Report 2011summitdailyNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Post-Exercise Recovery Strategies in Basketball: Practical Applications Based On Scientific EvidenceDocument17 pagesPost-Exercise Recovery Strategies in Basketball: Practical Applications Based On Scientific EvidenceMari PaoNo ratings yet
- 478 PeriodizationDocument13 pages478 Periodizationomarou1867% (3)
- 03-2 Essay - Robinson CrusoeDocument15 pages03-2 Essay - Robinson CrusoeIsa RodríguezNo ratings yet
- 2016 Article InternationalEcoHealthOneHealtDocument139 pages2016 Article InternationalEcoHealthOneHealtMauricio FemeníaNo ratings yet
- Hiradc Om - Talian AtasDocument57 pagesHiradc Om - Talian AtasapnadiNo ratings yet
- Emergency Response Procedures Manual - PT. Saberindo Pacific - 2011Document15 pagesEmergency Response Procedures Manual - PT. Saberindo Pacific - 2011Indah Rida Afriyanti100% (1)
- Flashcards About Medical DefinitionsDocument62 pagesFlashcards About Medical DefinitionsSrikanth PagidiNo ratings yet
- P.E & Health G11-Q1-M7Document13 pagesP.E & Health G11-Q1-M7John Gerald CantancioNo ratings yet
- Dengue Virus: A Vexatious "RED" FeverDocument6 pagesDengue Virus: A Vexatious "RED" FeverDr. Hussain NaqviNo ratings yet
- Fall Prevention: How Can Older Adults Prevent Falls?Document4 pagesFall Prevention: How Can Older Adults Prevent Falls?Amalina ZahariNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Theology of The BodyDocument2 pagesTheology of The BodyKim JuanNo ratings yet
- Relationship Among Levels of DFDsDocument8 pagesRelationship Among Levels of DFDssunny_242574No ratings yet
- Modern Canada Worksheet ESLDocument2 pagesModern Canada Worksheet ESLRafaelMacielNo ratings yet
- Case Study Keme 1Document9 pagesCase Study Keme 1JhovelNo ratings yet
- Biological Basis of HomosexulaityDocument22 pagesBiological Basis of HomosexulaityDhimitri BibolliNo ratings yet
- Pan India WED Report 21Document162 pagesPan India WED Report 21nioh envisNo ratings yet
- Dr. Hordinsky's ObituatiaryDocument1 pageDr. Hordinsky's ObituatiaryDiane HaugenNo ratings yet
- TUM CoursesDocument3 pagesTUM CoursesJoao N Da SilvaNo ratings yet
- Lung Contusion & Traumatic AsphyxiaDocument17 pagesLung Contusion & Traumatic AsphyxiaLady KeshiaNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)