You might also like
- Clinical Deterioration - A Concept AnalysisDocument29 pagesClinical Deterioration - A Concept AnalysisPaulaNo ratings yet
- 1 s2.0 S2666577822001009 Main - 2Document10 pages1 s2.0 S2666577822001009 Main - 2Shandy Suwanto PutraNo ratings yet
- Kidney Transplant Management: A Guide to Evaluation and ComorbiditiesFrom EverandKidney Transplant Management: A Guide to Evaluation and ComorbiditiesNo ratings yet
- Jurnal 1Document6 pagesJurnal 1Pratiwi AyuningtyasNo ratings yet
- Desmarais 2015Document4 pagesDesmarais 2015Jesica DiazNo ratings yet
- Kidney Transplantation: A Guide to the Care of Kidney Transplant RecipientsFrom EverandKidney Transplantation: A Guide to the Care of Kidney Transplant RecipientsNo ratings yet
- Comparative Effectiveness of Shock Wave Lithotripsy and Ureteroscopy For Treating Patients With Kidney StonesDocument6 pagesComparative Effectiveness of Shock Wave Lithotripsy and Ureteroscopy For Treating Patients With Kidney StonesparamithadishNo ratings yet
- Nasal Feeding Tubes Are Associated With Fewer AdveDocument7 pagesNasal Feeding Tubes Are Associated With Fewer AdveuchoaNo ratings yet
- Incontinence Managed or Mismanaged in Hospital SettingsDocument9 pagesIncontinence Managed or Mismanaged in Hospital SettingsDarrell BernardNo ratings yet
- Costs of Hospital MalnutritionDocument6 pagesCosts of Hospital MalnutritionAmalia SarsolNo ratings yet
- State of The Art Fluid Management in Critically.2Document1 pageState of The Art Fluid Management in Critically.2riks21No ratings yet
- Contributing Factors To Hemodialysis Adherence in Aceh, Indonesia - ScienceDirectDocument6 pagesContributing Factors To Hemodialysis Adherence in Aceh, Indonesia - ScienceDirectlaamaghfirohNo ratings yet
- 1 s2.0 S105122762300105X MainDocument11 pages1 s2.0 S105122762300105X MainJulia KhaerunisaNo ratings yet
- Medicine and Research An Ever-Changing FieldDocument7 pagesMedicine and Research An Ever-Changing Fieldapi-665163291No ratings yet
- Artigo 2 CinhalDocument7 pagesArtigo 2 CinhalSara PereiraNo ratings yet
- NIH Public Access: Predictors of Clinical Outcome After Tracheotomy in Critically Ill Obese PatientsDocument9 pagesNIH Public Access: Predictors of Clinical Outcome After Tracheotomy in Critically Ill Obese PatientsNaye Gmen DezNo ratings yet
- Original Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization PracticesDocument12 pagesOriginal Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization Practicesandi kurniawanNo ratings yet
- Patient Safety During Sedation by Anesthesia ProfeDocument8 pagesPatient Safety During Sedation by Anesthesia ProfeIsmar MorenoNo ratings yet
- Imaging in Suspected Renal Colic: Systematic Review of The Literature and Multispecialty ConsensusDocument12 pagesImaging in Suspected Renal Colic: Systematic Review of The Literature and Multispecialty ConsensusRose ParkNo ratings yet
- Association Between The Choice of IV Crystalloid and In-Hospital Mortality Among Critically Ill Adults With SepsisDocument7 pagesAssociation Between The Choice of IV Crystalloid and In-Hospital Mortality Among Critically Ill Adults With SepsisbernardoNo ratings yet
- New England Journal Medicine: The ofDocument12 pagesNew England Journal Medicine: The ofFarizka Dwinda HNo ratings yet
- Economic and Survival Burden of Dysphagia Among Inpatients in The United StatesDocument7 pagesEconomic and Survival Burden of Dysphagia Among Inpatients in The United StatesClaudia Lorena MedinaNo ratings yet
- Nurse-Directed Interventions To Reduce Catheter-Associated Urinary Tract InfectionsDocument10 pagesNurse-Directed Interventions To Reduce Catheter-Associated Urinary Tract InfectionsAngernani Trias WulandariNo ratings yet
- Sherri Ll 2020Document7 pagesSherri Ll 2020Yeudiel SuroNo ratings yet
- Decreasing Hospital Readmissions in Ileostomy PatientsDocument6 pagesDecreasing Hospital Readmissions in Ileostomy PatientsMEKSELINA KALENDERNo ratings yet
- Prehospital Airway Management A Systematic ReviewDocument13 pagesPrehospital Airway Management A Systematic Reviewembun pagiNo ratings yet
- Chen 2017Document7 pagesChen 2017Miranti Dea DoraNo ratings yet
- ABDOME AGUDO IDOSO Modified Hospital Elder Life Program Effects On Abdominal Surgery Patients.Document8 pagesABDOME AGUDO IDOSO Modified Hospital Elder Life Program Effects On Abdominal Surgery Patients.Joao FonsecaNo ratings yet
- One-Year Health Care Costs Associated With Delirium in The Elderly Population Editorial CommentDocument7 pagesOne-Year Health Care Costs Associated With Delirium in The Elderly Population Editorial CommentAmanda WongNo ratings yet
- Fluid Overload in Infants Following Congenital Heart SurgeryDocument6 pagesFluid Overload in Infants Following Congenital Heart SurgeryAngelica Lucero OrtizNo ratings yet
- Long-Term Rates of Bladder Dysfunction After Decompression in Patients With Cauda Equina SyndromeDocument7 pagesLong-Term Rates of Bladder Dysfunction After Decompression in Patients With Cauda Equina Syndrome刘希No ratings yet
- Achieving Sustainability in Reducing Unplanned Extubations in PICUDocument7 pagesAchieving Sustainability in Reducing Unplanned Extubations in PICUKevin Bazán TorrealvaNo ratings yet
- CirPed Diferença JPS 2014Document6 pagesCirPed Diferença JPS 2014Valmir MouraNo ratings yet
- Cronfa - Swansea University Open Access Repository: Diabetes Research and Clinical PracticeDocument7 pagesCronfa - Swansea University Open Access Repository: Diabetes Research and Clinical PracticeDimasjamalia SafiqriNo ratings yet
- Trauma, and Genital and Urethral Reconstruction: Re: Natural History of Low-Stage Urethral StricturesDocument2 pagesTrauma, and Genital and Urethral Reconstruction: Re: Natural History of Low-Stage Urethral StricturesWahyu IndraNo ratings yet
- JOT - 2015 - Childs - Obesity Is Associated W More Complicatiosn and Longer Hospital Stays After Ortho TraumaDocument6 pagesJOT - 2015 - Childs - Obesity Is Associated W More Complicatiosn and Longer Hospital Stays After Ortho TraumaJacob DoughertyNo ratings yet
- State-Of-The-Art Fluid Management in Critically Ill PatientsDocument1 pageState-Of-The-Art Fluid Management in Critically Ill PatientsVlady78No ratings yet
- Jurnal 6Document17 pagesJurnal 6Dhiny RatuNo ratings yet
- Pediatrics 2000 Johnson 1006 12Document9 pagesPediatrics 2000 Johnson 1006 12Amelia ArnisNo ratings yet
- The Association Between High Volume Intraoperative Fluid Administration and Outcomes Among Pediatric Patients Undergoing Large Bowel ResectionDocument7 pagesThe Association Between High Volume Intraoperative Fluid Administration and Outcomes Among Pediatric Patients Undergoing Large Bowel ResectionPablo Segales BautistaNo ratings yet
- Acute Abdomen in The Medical Intensive Care Unit: ArticleDocument5 pagesAcute Abdomen in The Medical Intensive Care Unit: ArticleChiriţoiu AnamariaNo ratings yet
- The Most Frequent Diagnosis On Patients Undergoing HemodialysisDocument5 pagesThe Most Frequent Diagnosis On Patients Undergoing HemodialysisChristine Rose EmNo ratings yet
- The Perioperative Complication Rate of Orthopedic PDFDocument10 pagesThe Perioperative Complication Rate of Orthopedic PDFAnh Nguyen HuuNo ratings yet
- Quality Metrics for ColonoscopyDocument204 pagesQuality Metrics for ColonoscopyWilliam Ricardo Effio GalvezNo ratings yet
- Pediatric Pancreatic Pseudocyst TreatmentDocument6 pagesPediatric Pancreatic Pseudocyst TreatmentChristian MolinaNo ratings yet
- SR and Guidelines For Periop MGMT of Peds Patients Undergoing Major Plastic SurgeryDocument10 pagesSR and Guidelines For Periop MGMT of Peds Patients Undergoing Major Plastic SurgeryPaul MarjiNo ratings yet
- Get Homework/Assignment DoneDocument6 pagesGet Homework/Assignment Donehomeworkping1No ratings yet
- 1 s2.0 S0002934314006871 Main PDFDocument9 pages1 s2.0 S0002934314006871 Main PDFcarlos orjuelaNo ratings yet
- Discharge Delay in Acute Care Reasons and DeterminantsDocument9 pagesDischarge Delay in Acute Care Reasons and DeterminantsGabriela ObonNo ratings yet
- Jamasurg E216902 s003Document30 pagesJamasurg E216902 s003Génesis HermidaNo ratings yet
- Pa Shik Anti 2012Document8 pagesPa Shik Anti 2012Irfan FauziNo ratings yet
- Main 16Document6 pagesMain 16pokharelriwaj82No ratings yet
- Shin 2017Document9 pagesShin 2017Nikos MavroudisNo ratings yet
- Biblio ObesityDocument7 pagesBiblio ObesitysimplyputmonicNo ratings yet
- Efficacy and Safety of Restrictive Blood TransfusiDocument4 pagesEfficacy and Safety of Restrictive Blood TransfusiJustin Jay Dar INo ratings yet
- Putting Evidence Into Practice® - Evidence-Based Interventions For The Prevention and Management of Constipation in Patients With CancerDocument19 pagesPutting Evidence Into Practice® - Evidence-Based Interventions For The Prevention and Management of Constipation in Patients With CancerMuhammadTaukhidNo ratings yet
- Early TIPS Versus Endoscopic Therapy For Secondary Prophylaxis After Management of Acute Esophageal Variceal Bleeding in Cirrhotic Patients: A Meta-Analysis of Randomized Controlled TrialsDocument26 pagesEarly TIPS Versus Endoscopic Therapy For Secondary Prophylaxis After Management of Acute Esophageal Variceal Bleeding in Cirrhotic Patients: A Meta-Analysis of Randomized Controlled Trialsray liNo ratings yet
- Velasquezreyes 2017Document11 pagesVelasquezreyes 2017Margarida ReisNo ratings yet
- Nurs478 HealthcaredeliveryDocument14 pagesNurs478 Healthcaredeliveryapi-316709773No ratings yet
- Azad 2019Document7 pagesAzad 2019Eka BagaskaraNo ratings yet
- Controversial TopicDocument11 pagesControversial TopicPutri Rizky AmaliaNo ratings yet
- NeurogenicbladdermanagementwithcompleteurethraldistructionDocument11 pagesNeurogenicbladdermanagementwithcompleteurethraldistructionPutri Rizky AmaliaNo ratings yet
- Multiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Document14 pagesMultiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Putri Rizky AmaliaNo ratings yet
- Surgical Management of The Neurogenic Bladder After Spinal CordDocument8 pagesSurgical Management of The Neurogenic Bladder After Spinal CordPutri Rizky AmaliaNo ratings yet
- Outcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisDocument7 pagesOutcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisPutri Rizky AmaliaNo ratings yet
- Multiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Document14 pagesMultiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Putri Rizky AmaliaNo ratings yet
- Rhinitis Allergy and ElderlyDocument26 pagesRhinitis Allergy and ElderlyPutri Rizky AmaliaNo ratings yet
- Role of Rhinitis in Laryngitis: Another Dimension of The Unified AirwayDocument6 pagesRole of Rhinitis in Laryngitis: Another Dimension of The Unified AirwayPutri Rizky AmaliaNo ratings yet
- Multiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Document14 pagesMultiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Putri Rizky AmaliaNo ratings yet
- Allergic Rhinitis, Asthma and Laryngopharyngeal Reflux Disease: A Cross Sectional Study On Their Reciprocal RelationsDocument8 pagesAllergic Rhinitis, Asthma and Laryngopharyngeal Reflux Disease: A Cross Sectional Study On Their Reciprocal RelationsPutri Rizky AmaliaNo ratings yet
- The Role of Allergy in Phonation: Athens, GreeceDocument9 pagesThe Role of Allergy in Phonation: Athens, GreecePutri Rizky AmaliaNo ratings yet
- Delong 2011Document6 pagesDelong 2011Putri Rizky AmaliaNo ratings yet
- 26 Jurnal LPRDocument5 pages26 Jurnal LPRaulia sufarnapNo ratings yet
- Healthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidenceDocument9 pagesHealthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidencePutri Rizky AmaliaNo ratings yet
- Otorhinolaryngology: Allergic Laryngitis: Chronic Laryngitis and Allergic SensitizationDocument4 pagesOtorhinolaryngology: Allergic Laryngitis: Chronic Laryngitis and Allergic SensitizationSyafira AlimNo ratings yet
- A New Definition For Wide-Necked Cerebral Aneurysms: Original ArticleDocument6 pagesA New Definition For Wide-Necked Cerebral Aneurysms: Original ArticlePutri Rizky AmaliaNo ratings yet
- Journal Reading Nasal Obstructive DisordersDocument37 pagesJournal Reading Nasal Obstructive DisordersPutri Rizky AmaliaNo ratings yet
- Rinitis Alergy Dan LPRDocument7 pagesRinitis Alergy Dan LPRcitra dewiNo ratings yet
- Literature Reading Short StatureDocument34 pagesLiterature Reading Short StaturePutri Rizky AmaliaNo ratings yet
- prm/2018/11 4/prm 11 4 prm170481/prm 11 prm170481Document9 pagesprm/2018/11 4/prm 11 4 prm170481/prm 11 prm170481Putri Rizky AmaliaNo ratings yet
- Jamaotolaryngology Lee 2019 Oi 190047Document7 pagesJamaotolaryngology Lee 2019 Oi 190047NadanNadhifahNo ratings yet
- Epos Summary PDFDocument30 pagesEpos Summary PDFPutri Rizky AmaliaNo ratings yet
- Evaluation of Functional Outcomes in Congenital HydrocephalusDocument2 pagesEvaluation of Functional Outcomes in Congenital HydrocephalusPutri Rizky AmaliaNo ratings yet
- Doctor Patient RelationshipDocument21 pagesDoctor Patient RelationshipPutri Rizky AmaliaNo ratings yet
- Post Partum ComplicationDocument29 pagesPost Partum ComplicationPutri Rizky AmaliaNo ratings yet
- GUS CASE 6 SummaryDocument2 pagesGUS CASE 6 SummaryPutri Rizky AmaliaNo ratings yet
- HHS Public Access: 236 Children With Developmental Hydrocephalus: Causes and Clinical ConsequencesDocument22 pagesHHS Public Access: 236 Children With Developmental Hydrocephalus: Causes and Clinical ConsequencesPutri Rizky AmaliaNo ratings yet
- The Half-Life of Infusion Fluids An Educational ReviewDocument8 pagesThe Half-Life of Infusion Fluids An Educational ReviewPutri Rizky AmaliaNo ratings yet
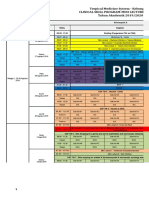
- Jadwal Perkulihanan THN 4 2019-2020 TM-FMDocument20 pagesJadwal Perkulihanan THN 4 2019-2020 TM-FMPutri Rizky AmaliaNo ratings yet
- UCLA Application Information Packet As of April 04 2014Document18 pagesUCLA Application Information Packet As of April 04 2014UCLA Center for Prehospital CareNo ratings yet
- Flow RateDocument2 pagesFlow Rateفيرمان ريشادNo ratings yet
- Keys To The Spirit World (Empath U)Document53 pagesKeys To The Spirit World (Empath U)Ruthy Balot100% (1)
- National Polio Lab ChecklistDocument12 pagesNational Polio Lab ChecklistSelaina NawadraNo ratings yet
- Highlights of key changes under the TRAIN LawDocument13 pagesHighlights of key changes under the TRAIN LawMiguel Anas Jr.No ratings yet
- Abnormal Cervical CytologyDocument21 pagesAbnormal Cervical CytologyNatalia HaikaliNo ratings yet
- Unit 726 WORK NVQDocument5 pagesUnit 726 WORK NVQMet nicolaouNo ratings yet
- Case Studies For PharmacyDocument3 pagesCase Studies For PharmacyMahima Sindhi50% (2)
- Flow rate uniformity of TARAL 200 PITON TURBO sprayer for pest controlDocument4 pagesFlow rate uniformity of TARAL 200 PITON TURBO sprayer for pest controlAndreea DiaconuNo ratings yet
- PR 2Document14 pagesPR 2Eduardo TalamanNo ratings yet
- DM-PH&SD-GU17-HCKS2 - Health Requirements For Kids SalonsDocument13 pagesDM-PH&SD-GU17-HCKS2 - Health Requirements For Kids SalonsPraveenKatkooriNo ratings yet
- Modes of Ventilation Chart - 1Document5 pagesModes of Ventilation Chart - 1Khamra SalahuddinNo ratings yet
- Abc of Burns: Kanwal Khan Lecturer ZCPTDocument35 pagesAbc of Burns: Kanwal Khan Lecturer ZCPTKanwal KhanNo ratings yet
- Fungal ClassificationDocument109 pagesFungal ClassificationMirza Shaharyar BaigNo ratings yet
- Cystocentesis K4Document24 pagesCystocentesis K4Sze KhayNo ratings yet
- pm597 Week15 Capstone Project AqsahchoudharyDocument14 pagespm597 Week15 Capstone Project Aqsahchoudharyapi-560364244No ratings yet
- Introductory Lecture by DR Prafull VijayakarDocument139 pagesIntroductory Lecture by DR Prafull Vijayakarpredictive amar100% (1)
- 09 ICSH Review of The Measurement of The ESR PDFDocument8 pages09 ICSH Review of The Measurement of The ESR PDFMuslim Majlis UojNo ratings yet
- Pathophysiology of Ligament Injuries-1Document21 pagesPathophysiology of Ligament Injuries-1abdul haseebNo ratings yet
- WIC Authorized Food List: Shopping GuideDocument17 pagesWIC Authorized Food List: Shopping GuideGanda PrajaNo ratings yet
- Medical Clearance Letter TemplateDocument3 pagesMedical Clearance Letter TemplateSebastián CoronadoNo ratings yet
- A-DEWS 2015 - Design Engineering in the Context of AsiaDocument568 pagesA-DEWS 2015 - Design Engineering in the Context of AsiaMukhlis Al QahharNo ratings yet
- Fear of Vomiting EmetophobiaDocument4 pagesFear of Vomiting EmetophobiaMagishaa ThiyagarajahNo ratings yet
- Far North Thrive Expo 2015 BookletDocument20 pagesFar North Thrive Expo 2015 BookletNicola YoungNo ratings yet
- Dr. Carmelita Divinagracia's COMPOSURE Model and its Impact on Patient WellnessDocument9 pagesDr. Carmelita Divinagracia's COMPOSURE Model and its Impact on Patient WellnessTRAZZY JEZRYL LASALA PLAZANo ratings yet
- Homework Tang KimHuyDocument2 pagesHomework Tang KimHuyseng songhaNo ratings yet
- Esthetiques Spa 201005Document134 pagesEsthetiques Spa 201005Kristina0% (1)
- Clinical Audit ReportDocument6 pagesClinical Audit Reportjhonron100% (1)
- Shean19 VaPID RefthroughGeneBankDocument8 pagesShean19 VaPID RefthroughGeneBankAnh H NguyenNo ratings yet
- God's Cancer ParmacyDocument5 pagesGod's Cancer ParmacyNick BantoloNo ratings yet