You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- NeurogenicbladdermanagementwithcompleteurethraldistructionDocument11 pagesNeurogenicbladdermanagementwithcompleteurethraldistructionPutri Rizky AmaliaNo ratings yet
- Outcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisDocument7 pagesOutcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisPutri Rizky AmaliaNo ratings yet
- Controversial TopicDocument11 pagesControversial TopicPutri Rizky AmaliaNo ratings yet
- Multiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Document14 pagesMultiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Putri Rizky AmaliaNo ratings yet
- Peterson 2012Document5 pagesPeterson 2012Putri Rizky AmaliaNo ratings yet
- Role of Rhinitis in Laryngitis: Another Dimension of The Unified AirwayDocument6 pagesRole of Rhinitis in Laryngitis: Another Dimension of The Unified AirwayPutri Rizky AmaliaNo ratings yet
- Rhinitis Allergy and ElderlyDocument26 pagesRhinitis Allergy and ElderlyPutri Rizky AmaliaNo ratings yet
- prm/2018/11 4/prm 11 4 prm170481/prm 11 prm170481Document9 pagesprm/2018/11 4/prm 11 4 prm170481/prm 11 prm170481Putri Rizky AmaliaNo ratings yet
- HHS Public Access: 236 Children With Developmental Hydrocephalus: Causes and Clinical ConsequencesDocument22 pagesHHS Public Access: 236 Children With Developmental Hydrocephalus: Causes and Clinical ConsequencesPutri Rizky AmaliaNo ratings yet
- Literature Reading Short StatureDocument34 pagesLiterature Reading Short StaturePutri Rizky AmaliaNo ratings yet
- Post Partum ComplicationDocument29 pagesPost Partum ComplicationPutri Rizky AmaliaNo ratings yet
- Healthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidenceDocument9 pagesHealthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidencePutri Rizky AmaliaNo ratings yet
- Doctor Patient RelationshipDocument21 pagesDoctor Patient RelationshipPutri Rizky AmaliaNo ratings yet
- The Half-Life of Infusion Fluids An Educational ReviewDocument8 pagesThe Half-Life of Infusion Fluids An Educational ReviewPutri Rizky AmaliaNo ratings yet
- Epos Summary PDFDocument30 pagesEpos Summary PDFPutri Rizky AmaliaNo ratings yet
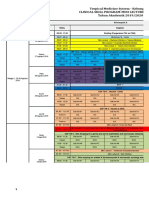
- Jadwal Perkulihanan THN 4 2019-2020 TM-FMDocument20 pagesJadwal Perkulihanan THN 4 2019-2020 TM-FMPutri Rizky AmaliaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Guide For Writing NotesDocument10 pagesGuide For Writing Notesiamsera100% (1)
- Psychoactive Drugs ChartDocument5 pagesPsychoactive Drugs ChartAlessandra WilliamsNo ratings yet
- Exercises For DiabetesDocument25 pagesExercises For DiabetesrichaNo ratings yet
- Group 4 Environmental Pollution and Impacts On Public HealthDocument10 pagesGroup 4 Environmental Pollution and Impacts On Public HealthBen KuNo ratings yet
- Arterial Line Analysis PresentationDocument35 pagesArterial Line Analysis PresentationLisa GilbertNo ratings yet
- Feed Additives, Antibodies, Poultry Vaccines 2023.3Document6 pagesFeed Additives, Antibodies, Poultry Vaccines 2023.3Bruce YangNo ratings yet
- Burning Mouth Syndrome 1Document16 pagesBurning Mouth Syndrome 1Mihika BalaNo ratings yet
- Meiosis GizmosDocument9 pagesMeiosis GizmosShaylee TorresNo ratings yet
- Agc332 Lecture 10-Wheat DiseasesDocument33 pagesAgc332 Lecture 10-Wheat DiseasesSolomon MbeweNo ratings yet
- Ultimate Guide To Surviving in The WildDocument175 pagesUltimate Guide To Surviving in The WildSal Ot100% (1)
- Bril (2002) - Validation of The Toronto Clinical Scoring System For Diabetic PolyneuropathyDocument5 pagesBril (2002) - Validation of The Toronto Clinical Scoring System For Diabetic PolyneuropathyRicky WatariNo ratings yet
- Breast Cancer Staging SystemDocument4 pagesBreast Cancer Staging SystemGabriella PatriciaNo ratings yet
- MMC 8Document27 pagesMMC 8Neil Patrick AngelesNo ratings yet
- Soca Review Genitourinary System Case 1-Urinary StoneDocument6 pagesSoca Review Genitourinary System Case 1-Urinary StoneImania Salim Ahmad BawazierNo ratings yet
- Dr. Marcelia Suryatenggara, Sp. S - How To Choose Your AnalgeticsDocument9 pagesDr. Marcelia Suryatenggara, Sp. S - How To Choose Your AnalgeticsFreade AkbarNo ratings yet
- Clinical Microbiology and Infection: Original ArticleDocument6 pagesClinical Microbiology and Infection: Original ArticleAkira Masumi100% (1)
- Effectiveness of Psychoeducation For Relapse, Symptoms, Knowledge, Adherence and Functioning in Psychotic Disorders: A Meta-AnalysisDocument14 pagesEffectiveness of Psychoeducation For Relapse, Symptoms, Knowledge, Adherence and Functioning in Psychotic Disorders: A Meta-AnalysisPatty IzquierdoNo ratings yet
- Critical Care of Children With Heart Disease 2010Document735 pagesCritical Care of Children With Heart Disease 2010Haikel Mhamed100% (1)
- Mental Health Class NotesDocument3 pagesMental Health Class Notessuz100% (4)
- Sanum Therapy Book Helios PDFDocument314 pagesSanum Therapy Book Helios PDFOscarNo ratings yet
- Analytical Case Study of Bmiof Mildly Symptomatic Covid-19 Patients With Reference To MizajDocument7 pagesAnalytical Case Study of Bmiof Mildly Symptomatic Covid-19 Patients With Reference To MizajyusufNo ratings yet
- What Is Rheumatoid ArthritisDocument16 pagesWhat Is Rheumatoid ArthritisDurge Raj GhalanNo ratings yet
- Par QDocument1 pagePar Qapi-39512869100% (1)
- Home Quarantine Compliance 2022 1Document1 pageHome Quarantine Compliance 2022 1Puting KahoyNo ratings yet
- Presc Audit ReportDocument85 pagesPresc Audit ReportAnuj KaushalNo ratings yet
- Child Abuse and Juvenile DelinquencyDocument42 pagesChild Abuse and Juvenile DelinquencyArmarni Seany Desmangles100% (2)
- Maret 18 PDFDocument178 pagesMaret 18 PDFAnonymous vLgCd0U7No ratings yet
- Euthanasia ThesisDocument11 pagesEuthanasia ThesisAyush MathurNo ratings yet
- Caffein Intox PDFDocument3 pagesCaffein Intox PDFSejahtera SurbaktiNo ratings yet
- Contact Lens Complications and ManagementDocument10 pagesContact Lens Complications and Managementstrawberry8832850% (2)