You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Multiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Document14 pagesMultiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Putri Rizky AmaliaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Outcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisDocument7 pagesOutcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisPutri Rizky AmaliaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- NeurogenicbladdermanagementwithcompleteurethraldistructionDocument11 pagesNeurogenicbladdermanagementwithcompleteurethraldistructionPutri Rizky AmaliaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Controversial TopicDocument11 pagesControversial TopicPutri Rizky AmaliaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Peterson 2012Document5 pagesPeterson 2012Putri Rizky AmaliaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Rhinitis Allergy and ElderlyDocument26 pagesRhinitis Allergy and ElderlyPutri Rizky AmaliaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Role of Rhinitis in Laryngitis: Another Dimension of The Unified AirwayDocument6 pagesRole of Rhinitis in Laryngitis: Another Dimension of The Unified AirwayPutri Rizky AmaliaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Epos Summary PDFDocument30 pagesEpos Summary PDFPutri Rizky AmaliaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Healthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidenceDocument9 pagesHealthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidencePutri Rizky AmaliaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Literature Reading Short StatureDocument34 pagesLiterature Reading Short StaturePutri Rizky AmaliaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- prm/2018/11 4/prm 11 4 prm170481/prm 11 prm170481Document9 pagesprm/2018/11 4/prm 11 4 prm170481/prm 11 prm170481Putri Rizky AmaliaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- HHS Public Access: 236 Children With Developmental Hydrocephalus: Causes and Clinical ConsequencesDocument22 pagesHHS Public Access: 236 Children With Developmental Hydrocephalus: Causes and Clinical ConsequencesPutri Rizky AmaliaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Doctor Patient RelationshipDocument21 pagesDoctor Patient RelationshipPutri Rizky AmaliaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Half-Life of Infusion Fluids An Educational ReviewDocument8 pagesThe Half-Life of Infusion Fluids An Educational ReviewPutri Rizky AmaliaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Post Partum ComplicationDocument29 pagesPost Partum ComplicationPutri Rizky AmaliaNo ratings yet
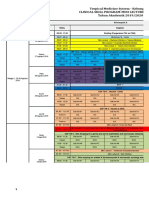
- Jadwal Perkulihanan THN 4 2019-2020 TM-FMDocument20 pagesJadwal Perkulihanan THN 4 2019-2020 TM-FMPutri Rizky AmaliaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2010 Stoma ReversalDocument5 pages2010 Stoma Reversaljay n shahNo ratings yet
- Mu 31Document4 pagesMu 31Lovkesh GoyalNo ratings yet
- Management of Trauma PatientsDocument10 pagesManagement of Trauma PatientsShennie C AnteNo ratings yet
- Capsular Tension Rings:: Current Indications and OutcomesDocument12 pagesCapsular Tension Rings:: Current Indications and OutcomesShahid ManzoorNo ratings yet
- 08 - Privileges - General SurgeryDocument3 pages08 - Privileges - General SurgeryAccreditation ConsultantNo ratings yet
- Bowa Cat 10764 Electrosurgery Complete 2019 02 15 de en FR Es ItDocument208 pagesBowa Cat 10764 Electrosurgery Complete 2019 02 15 de en FR Es Itinstrumed_globalNo ratings yet
- Coronary Artery Bypass GraftDocument9 pagesCoronary Artery Bypass GraftYen NgoNo ratings yet
- Clinical Outcomes of Lumbar Disc Herniation Treated by Minimaly Invasive Discectomy With Tubular RetractorDocument7 pagesClinical Outcomes of Lumbar Disc Herniation Treated by Minimaly Invasive Discectomy With Tubular RetractorPankaj VatsaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Subbrow Blepharoplasty For Upper Eyelid Rejuvenation in AsiansDocument5 pagesSubbrow Blepharoplasty For Upper Eyelid Rejuvenation in AsiansdoctorbanNo ratings yet
- Penile Inversion Vaginoplasty TechniqueDocument2 pagesPenile Inversion Vaginoplasty Techniquecathylamont816No ratings yet
- Surgery BoardsDocument16 pagesSurgery Boardscusom34100% (1)
- Cystostomy GABDocument27 pagesCystostomy GABsagaNo ratings yet
- Needle Dermabrasion: Abstract. in This Article We Describe A Technique of NeedleDocument2 pagesNeedle Dermabrasion: Abstract. in This Article We Describe A Technique of NeedleludyNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Health India Network ListDocument190 pagesHealth India Network ListManish BalpandeNo ratings yet
- CV - Dr. Manish Mandal GISDocument3 pagesCV - Dr. Manish Mandal GISChandan KumarNo ratings yet
- Programa NCR PedDocument3 pagesPrograma NCR PedLuiz AndersonNo ratings yet
- S LUPESCU Timpanoplastia Under OverlayDocument109 pagesS LUPESCU Timpanoplastia Under OverlayEdy MorarNo ratings yet
- Urine EliminationDocument33 pagesUrine EliminationInnocent MuhumuzaNo ratings yet
- Grs 2021 00059Document8 pagesGrs 2021 00059jonj72351No ratings yet
- Aesculap CaimanDocument6 pagesAesculap CaimanAnonymous Qo6L9YQsdNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Announcement Fiesta Urologi 2017Document8 pagesAnnouncement Fiesta Urologi 2017Alfin KamalNo ratings yet
- Recent Final Frca Vascular Anaesthesia QuestionsDocument4 pagesRecent Final Frca Vascular Anaesthesia Questionslim sjNo ratings yet
- Percutaneous Nephrolithotomy - WikipediaDocument7 pagesPercutaneous Nephrolithotomy - WikipediaZaheer UllahNo ratings yet
- AbbreviationDocument2 pagesAbbreviationdwlnuestro10No ratings yet
- Clinical Profile and Visual Outcome of Ocular Injuries in Tertiary Care Rural HospitalDocument8 pagesClinical Profile and Visual Outcome of Ocular Injuries in Tertiary Care Rural HospitalIJAR JOURNALNo ratings yet
- DR - KumarSonal No CVDocument3 pagesDR - KumarSonal No CVashish bondiaNo ratings yet
- Neuropsych Eval Report Sample mTBI 2Document3 pagesNeuropsych Eval Report Sample mTBI 2Sopho TsagareishviliNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakamemeeeyyyNo ratings yet
- Return Invoice 231.8.2023Document2 pagesReturn Invoice 231.8.2023ahmed.zulkhaireNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (82)