You might also like
- Dlsumc Paper111Document19 pagesDlsumc Paper111api-292484841No ratings yet
- Business Law and Regulations ReviewerDocument6 pagesBusiness Law and Regulations ReviewerJoris YapNo ratings yet
- Methods For Teaching PDFDocument114 pagesMethods For Teaching PDFPutra Bhungsu100% (2)
- Engaging Physicians in A Shared Quality Agenda: Innovation Series 2007Document52 pagesEngaging Physicians in A Shared Quality Agenda: Innovation Series 2007drabhi23No ratings yet
- Understanding Culture, Society, and Politics Quarter 2 - Module 5 EducationDocument19 pagesUnderstanding Culture, Society, and Politics Quarter 2 - Module 5 EducationLallaina AlexisNo ratings yet
- High Performance in Hospital Management PDFDocument232 pagesHigh Performance in Hospital Management PDFZaid R100% (1)
- AP-PW 91: Review Problems-1Document9 pagesAP-PW 91: Review Problems-1Joris YapNo ratings yet
- Audit of InventoriesDocument9 pagesAudit of InventoriesJoris YapNo ratings yet
- COURSE of Interior DesignDocument235 pagesCOURSE of Interior DesignAhmed MohmmedNo ratings yet
- Final Preboard ExaminationDocument14 pagesFinal Preboard ExaminationJoris YapNo ratings yet
- Quality Improvement Paper FinalDocument11 pagesQuality Improvement Paper Finalapi-291740538No ratings yet
- Improving ED Handoffs at SFGHDocument4 pagesImproving ED Handoffs at SFGHzakuan79100% (2)
- Annex2 Clinical Leadership and QualityDocument22 pagesAnnex2 Clinical Leadership and Qualitymyjunk299709No ratings yet
- MCQs IN PROPERTYDocument12 pagesMCQs IN PROPERTYAbegail AtokNo ratings yet
- RFBT Preweek 91Document30 pagesRFBT Preweek 91Joris YapNo ratings yet
- 8 - Bail ApplicationDocument3 pages8 - Bail ApplicationJalaj AgarwalNo ratings yet
- Clinical Governance Framework EssentialsDocument9 pagesClinical Governance Framework EssentialsSajid Rahman100% (1)
- MAS AbitiagoDocument6 pagesMAS AbitiagoJoris YapNo ratings yet
- High Performance in Hospital ManagementDocument232 pagesHigh Performance in Hospital ManagementTamil Selva100% (1)
- AFAR Preweek Lecture Part 2Document18 pagesAFAR Preweek Lecture Part 2Joris YapNo ratings yet
- Joint Commission Research PaperDocument8 pagesJoint Commission Research Paperuzypvhhkf100% (1)
- Master of Public Health Thesis ExamplesDocument5 pagesMaster of Public Health Thesis Examplesp0kasov1syd2100% (2)
- 02 ACHE-SETC Scholarship2015 CaseStudy CBNDocument9 pages02 ACHE-SETC Scholarship2015 CaseStudy CBNClaudia NeumannNo ratings yet
- In Good Hands ReportDocument8 pagesIn Good Hands ReportMartin ThomasNo ratings yet
- Hospital Quality Improvement StrategiesDocument70 pagesHospital Quality Improvement StrategiesSebrindaa GinaNo ratings yet
- Global Minimum Essential Requirements in Medical EducationDocument15 pagesGlobal Minimum Essential Requirements in Medical Educationa.jabal752019No ratings yet
- Research Paper On Hospital ManagementDocument6 pagesResearch Paper On Hospital Managementkifmgbikf100% (1)
- System Theory AssignDocument5 pagesSystem Theory AssignYnaffit Alteza UntalNo ratings yet
- Hosp Study MMH2Document26 pagesHosp Study MMH2Bhell MendiolaNo ratings yet
- How To Write A Research Paper NursingDocument7 pagesHow To Write A Research Paper Nursingoyrzvcrif100% (3)
- Producing Competent Physicians - More Paper Work or IndeedDocument48 pagesProducing Competent Physicians - More Paper Work or Indeedapi-26176346No ratings yet
- Innovation Awards Round 2 Batch 1Document7 pagesInnovation Awards Round 2 Batch 1iggybauNo ratings yet
- Hospital Management Research PapersDocument8 pagesHospital Management Research Papersaflbsybmc100% (1)
- Chief Registrar role at NUHDocument7 pagesChief Registrar role at NUHOzhenNo ratings yet
- Thesis For Hospital AdministrationDocument5 pagesThesis For Hospital Administrationlisajonesshreveport100% (2)
- 40 A National Strategy Pp982 990Document9 pages40 A National Strategy Pp982 990cma909No ratings yet
- Download Building A High Value Health System Rifat Atun full chapterDocument67 pagesDownload Building A High Value Health System Rifat Atun full chapterbill.owens447100% (5)
- LTC-Hospital Collaboration to Prevent HAC ConditionsDocument2 pagesLTC-Hospital Collaboration to Prevent HAC Conditionskudo01No ratings yet
- MHA at Global Hospitals - Healthcare Leadership CareerDocument8 pagesMHA at Global Hospitals - Healthcare Leadership CareerRaja RamNo ratings yet
- Clinical Fellow in Sustainable Healthcare (Anaesthesia/MedicineDocument9 pagesClinical Fellow in Sustainable Healthcare (Anaesthesia/MedicineBibek AcharyaNo ratings yet
- PNACF510Document56 pagesPNACF510Jerusalem ShiferawNo ratings yet
- Building A Clinical Program in A Sin - 2001 - The Journal of Thoracic and CardioDocument5 pagesBuilding A Clinical Program in A Sin - 2001 - The Journal of Thoracic and Cardionouha jhiderNo ratings yet
- Medical Thesis Online Full Text IndiaDocument5 pagesMedical Thesis Online Full Text IndiaJames Heller100% (1)
- Unbundling The HospitalDocument5 pagesUnbundling The Hospitalcrb202No ratings yet
- Title - : 1.1 Introduction of TopicDocument17 pagesTitle - : 1.1 Introduction of TopicAtharv MehtaNo ratings yet
- Research ProposalDocument21 pagesResearch ProposalShuvashish Dey100% (1)
- Research Paper On Hospital DesignDocument7 pagesResearch Paper On Hospital Designj1zijefifin3100% (1)
- Your Hospitals Path Second CurveDocument43 pagesYour Hospitals Path Second CurveiggybauNo ratings yet
- Research Paper Delegation in NursingDocument6 pagesResearch Paper Delegation in Nursingafeavbrpd100% (1)
- Nursing Research Papers FreeDocument5 pagesNursing Research Papers Freec9sj0n70100% (1)
- UHCancer Center Review Report PDFDocument124 pagesUHCancer Center Review Report PDFHonolulu Star-AdvertiserNo ratings yet
- Leanring Outcomes and Threshold Concepts: Introduction To Complex Health SystemsDocument5 pagesLeanring Outcomes and Threshold Concepts: Introduction To Complex Health SystemsKweku Gepi-Attee100% (1)
- The Visionary Magazine - Spring 2011Document44 pagesThe Visionary Magazine - Spring 2011Nova Southeastern University's College of Optometry- Visionary MagazineNo ratings yet
- Hospital and It's OrganizationDocument48 pagesHospital and It's OrganizationMit PatelNo ratings yet
- Healthcare Service Lines - The State of The Future by Dr. Jon BurroughsDocument10 pagesHealthcare Service Lines - The State of The Future by Dr. Jon BurroughsAbidi HichemNo ratings yet
- Assignment Cover Sheet: Student DetailsDocument11 pagesAssignment Cover Sheet: Student DetailsHasan AhmadNo ratings yet
- Licensure Accreditation and CertificationDocument63 pagesLicensure Accreditation and Certificationradomir.boskovicNo ratings yet
- Patient Safety A Literature Review On The Impact of Nursing Empowerment Leadership and CollaborationDocument5 pagesPatient Safety A Literature Review On The Impact of Nursing Empowerment Leadership and Collaborationea428adhNo ratings yet
- 1 March 2017: Clinical Directorates Underpinning Principles & Operating FrameworkDocument12 pages1 March 2017: Clinical Directorates Underpinning Principles & Operating FrameworkJames SmallNo ratings yet
- Birk ReducingHospReadmissionsSTAAR HCExec Mar12Document7 pagesBirk ReducingHospReadmissionsSTAAR HCExec Mar12Diah PutriNo ratings yet
- The Importance of Clinical Leadership in The Hospital SettingDocument6 pagesThe Importance of Clinical Leadership in The Hospital SettinghikaruNo ratings yet
- Review of Literature On Health and Safety MeasuresDocument9 pagesReview of Literature On Health and Safety MeasuresfrqofvbndNo ratings yet
- Lean PsicologyDocument8 pagesLean PsicologyMartajp7No ratings yet
- To Become The World's Best Tertiary Healthcare ProviderDocument13 pagesTo Become The World's Best Tertiary Healthcare ProviderShah BrijeshkumarNo ratings yet
- Thesis Topics For Masters in Public HealthDocument6 pagesThesis Topics For Masters in Public Healthhptfbggig100% (2)
- For The Clinical Translation of Stem Cells. Originally Published in DecemberDocument2 pagesFor The Clinical Translation of Stem Cells. Originally Published in DecemberMarian Alexis FernandezNo ratings yet
- Evidence Based RUADocument12 pagesEvidence Based RUAAsma AliNo ratings yet
- From Solution Shop' Model To Focused Factory' in Hospital Surgery: Increasing Care Value and PredictabilityDocument10 pagesFrom Solution Shop' Model To Focused Factory' in Hospital Surgery: Increasing Care Value and PredictabilityDhruv JindalNo ratings yet
- profileMolly-Coyepublication23759904 Remote Patient Management Technology-Enabled Innovation andDocument26 pagesprofileMolly-Coyepublication23759904 Remote Patient Management Technology-Enabled Innovation andptriw nigsihNo ratings yet
- Healthcare Management Research PaperDocument10 pagesHealthcare Management Research Paperkbcymacnd100% (1)
- Improve patient care with integrated care pathwaysDocument3 pagesImprove patient care with integrated care pathwaysFitri EmiNo ratings yet
- Manila MAY 5, 2022 Preweek Material: Management Advisory ServicesDocument25 pagesManila MAY 5, 2022 Preweek Material: Management Advisory ServicesJoris YapNo ratings yet
- At-91 PW (Part 1)Document11 pagesAt-91 PW (Part 1)Joris YapNo ratings yet
- Final Preboard Batch 91 Reviewees PDFDocument18 pagesFinal Preboard Batch 91 Reviewees PDFJoris YapNo ratings yet
- Batch 91 Final Preboard April 2022 - SolutionsDocument6 pagesBatch 91 Final Preboard April 2022 - SolutionsJoris YapNo ratings yet
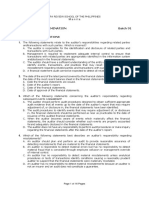
- AUD Final Preboard Examination QuestionnaireDocument16 pagesAUD Final Preboard Examination QuestionnaireJoris YapNo ratings yet
- Batch 91 Final Preboard April 2022Document13 pagesBatch 91 Final Preboard April 2022Joris YapNo ratings yet
- Afar Self TestDocument8 pagesAfar Self Testfor youNo ratings yet
- Final Audpb-91st-Apr 2022 (Solutions)Document5 pagesFinal Audpb-91st-Apr 2022 (Solutions)Joris YapNo ratings yet
- GROUP 1 - Sec 53-58Document3 pagesGROUP 1 - Sec 53-58Joris YapNo ratings yet
- At-91 PW (Part 2)Document12 pagesAt-91 PW (Part 2)Joris YapNo ratings yet
- Advanced Financial Accounting and Reporting Preweek LectureDocument19 pagesAdvanced Financial Accounting and Reporting Preweek LectureVanessa Anne Acuña DavisNo ratings yet
- 7019 - Preweek Lecture FAR TheoryDocument6 pages7019 - Preweek Lecture FAR TheoryJoris YapNo ratings yet
- 7018 - Preweek Lecture FAR ProblemsDocument9 pages7018 - Preweek Lecture FAR ProblemsJoris YapNo ratings yet
- 7017 - Preweek Lecture FAR ProblemsDocument8 pages7017 - Preweek Lecture FAR ProblemsJohn Paul ArrozaNo ratings yet
- B-Tmas401 Sy 2021 - 2022Document17 pagesB-Tmas401 Sy 2021 - 2022Joris YapNo ratings yet
- YAP Joris - BSA 22 - Midterms Online Quiz 1Document3 pagesYAP Joris - BSA 22 - Midterms Online Quiz 1Joris YapNo ratings yet
- 91 - Final Preaboard AFAR Solutions (WEEKENDS)Document9 pages91 - Final Preaboard AFAR Solutions (WEEKENDS)Joris YapNo ratings yet
- 91 - Final Preaboard Afar (Weekends)Document18 pages91 - Final Preaboard Afar (Weekends)Joris YapNo ratings yet
- YAP Joris - BSA 22 - Midterms Online Quiz 1 - Item 2Document1 pageYAP Joris - BSA 22 - Midterms Online Quiz 1 - Item 2Joris YapNo ratings yet
- 2010-2015 Tax Bar Based On The 2015 Bar Syllabus PDFDocument124 pages2010-2015 Tax Bar Based On The 2015 Bar Syllabus PDFNin BANo ratings yet
- Peza LawDocument31 pagesPeza LawFebz CanutabNo ratings yet
- List of Operating Medical Tourism Zone: Total No. 2Document28 pagesList of Operating Medical Tourism Zone: Total No. 2Joris YapNo ratings yet
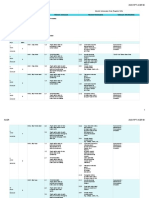
- Detailed Class Schedules B-TMAS401Document1 pageDetailed Class Schedules B-TMAS401Joris YapNo ratings yet
- Siaton Science High School 2nd Grading Exam ReportDocument1 pageSiaton Science High School 2nd Grading Exam ReportEugene JamandronNo ratings yet
- Chapter 4: Logistics Customer Service: - Definition and Measurement. - Fundamental TradeoffDocument14 pagesChapter 4: Logistics Customer Service: - Definition and Measurement. - Fundamental TradeoffawaisjinnahNo ratings yet
- Health10 - Q2 - Mod4 (SHLD Be Mod3 Based On MELC) - ManagingHealthTrendsIssuesAndConcerns - V1Document26 pagesHealth10 - Q2 - Mod4 (SHLD Be Mod3 Based On MELC) - ManagingHealthTrendsIssuesAndConcerns - V1Dreyzen GanotisiNo ratings yet
- Mock 8Document75 pagesMock 8satyajitadrijaNo ratings yet
- Reflection On Distance Learning - CompressedDocument1 pageReflection On Distance Learning - Compressedapi-500622015No ratings yet
- Usha Bhatiya: Actress & ModelDocument9 pagesUsha Bhatiya: Actress & ModelDisha SharmaNo ratings yet
- Ward 7 SurveyDocument7 pagesWard 7 SurveyThe London Free PressNo ratings yet
- CHAPTER2 Thesis Ryan Computer EnhancementDocument21 pagesCHAPTER2 Thesis Ryan Computer Enhancementlyca omapasNo ratings yet
- Difference Between MBA and PGDMDocument2 pagesDifference Between MBA and PGDMAnjanaKrishnanNo ratings yet
- PregovaranjeDocument11 pagesPregovaranjeMarijana Djordjevic0% (1)
- PGX F ParticipatoryPolicy MakingDocument16 pagesPGX F ParticipatoryPolicy MakingRifqi Andika ArsyadNo ratings yet
- The Benefits and Challenges of Collaborative Multi-Agency WorkingDocument20 pagesThe Benefits and Challenges of Collaborative Multi-Agency WorkingRawbema MarzNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument15 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsYonese GonzalesNo ratings yet
- Marketing Communication Assessment 08Document3 pagesMarketing Communication Assessment 08Balaji altNo ratings yet
- Application Form FOR AffiliationDocument9 pagesApplication Form FOR AffiliationBrilliance International AcademyNo ratings yet
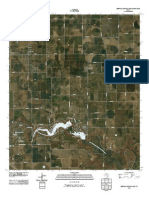
- Topographic Map of Buffalo Springs LakeDocument1 pageTopographic Map of Buffalo Springs LakeHistoricalMapsNo ratings yet
- English - G8 - Q2 - W3-4 - Samantha Bea GasingDocument10 pagesEnglish - G8 - Q2 - W3-4 - Samantha Bea GasingGennrick PajaronNo ratings yet
- Form 4. LAC Engagement Report 1Document2 pagesForm 4. LAC Engagement Report 1Janelkris Plaza100% (1)
- Flowering vs Non-Flowering Plants LessonDocument3 pagesFlowering vs Non-Flowering Plants LessonMariel AronNo ratings yet
- In This Unit My Pupils Will Learn To : Discovering LanguageDocument16 pagesIn This Unit My Pupils Will Learn To : Discovering LanguageAmine BougNo ratings yet
- Milani Cosmetics: Marketing PlanDocument8 pagesMilani Cosmetics: Marketing PlanAYUSHI SONINo ratings yet
- The Enduring Context of IhrmDocument23 pagesThe Enduring Context of IhrmhunzakhalidNo ratings yet
- German Short Stories: 9 Simple and Captivating Stories For Effective German Learning For BeginnersDocument51 pagesGerman Short Stories: 9 Simple and Captivating Stories For Effective German Learning For BeginnersRamsai ChigurupatiNo ratings yet
- Narrative Margin Format 1Document27 pagesNarrative Margin Format 1Shira Mae GulfericNo ratings yet
- Rancangan Pengajaran Tahunan Bahasa Inggeris Tahun 1 Semakan 2017Document9 pagesRancangan Pengajaran Tahunan Bahasa Inggeris Tahun 1 Semakan 2017sitinorhidayahazmeeNo ratings yet