You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
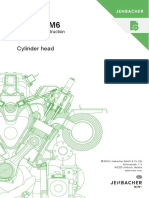
- Cylinder Head: Maintenance InstructionDocument12 pagesCylinder Head: Maintenance InstructionReny NapitupuluNo ratings yet
- En 10025 PDFDocument35 pagesEn 10025 PDFAbdelali88% (8)
- 100 transaction cycle in VisionPLUS banking systemDocument7 pages100 transaction cycle in VisionPLUS banking systemGoushik Balakrishnan100% (1)
- LING-05 Assets and Liabilities of The English Language Prepared by Mario Pei and John Nist Edited by David F. MaasDocument17 pagesLING-05 Assets and Liabilities of The English Language Prepared by Mario Pei and John Nist Edited by David F. MaasDavid F Maas71% (7)
- Jurnal 13 Bu RoroDocument21 pagesJurnal 13 Bu RoroReny NapitupuluNo ratings yet
- Rekap SO 30-31 OktDocument827 pagesRekap SO 30-31 OktReny NapitupuluNo ratings yet
- Jurnal UTS Ibu RinaDocument7 pagesJurnal UTS Ibu RinaReny NapitupuluNo ratings yet
- Innovality - Sentra Medika CibinongDocument39 pagesInnovality - Sentra Medika CibinongReny NapitupuluNo ratings yet
- The Effect of Work From Home OnDocument13 pagesThe Effect of Work From Home OnReny NapitupuluNo ratings yet
- Doctor Schedule and Staff ListDocument25 pagesDoctor Schedule and Staff ListReny NapitupuluNo ratings yet
- Jurnal 13 Bu RoroDocument21 pagesJurnal 13 Bu RoroReny NapitupuluNo ratings yet
- Jurnal 13 Bu Roro (Word)Document21 pagesJurnal 13 Bu Roro (Word)Reny NapitupuluNo ratings yet
- Jurnal Case Control UTS (Idrus) 3Document8 pagesJurnal Case Control UTS (Idrus) 3Reny NapitupuluNo ratings yet
- Certificate Jenbacher ReaderDocument1 pageCertificate Jenbacher ReaderReny NapitupuluNo ratings yet
- Role of HRM Practices in Performance of Organization and Employee RetentionDocument7 pagesRole of HRM Practices in Performance of Organization and Employee RetentionMuhammad Ismail LashariNo ratings yet
- Role of HRM Practices in Performance of Organization and Employee RetentionDocument7 pagesRole of HRM Practices in Performance of Organization and Employee RetentionMuhammad Ismail LashariNo ratings yet
- Product Specification XR6000 PDFDocument1 pageProduct Specification XR6000 PDFrafikNo ratings yet
- Jurnal Kasus Kontrol Singapore (Idrus)Document6 pagesJurnal Kasus Kontrol Singapore (Idrus)Reny NapitupuluNo ratings yet
- Jurnal Case Control UTS (Idrus) 4Document4 pagesJurnal Case Control UTS (Idrus) 4Reny NapitupuluNo ratings yet
- Jurnal Case Control UTS (Idrus) 5Document8 pagesJurnal Case Control UTS (Idrus) 5Reny NapitupuluNo ratings yet
- Jurnal Case Control UTS (Idrus) 3Document8 pagesJurnal Case Control UTS (Idrus) 3Reny NapitupuluNo ratings yet
- BMC Health Services ResearchDocument10 pagesBMC Health Services ResearchReny NapitupuluNo ratings yet
- HVAHVA KosonganDocument7 pagesHVAHVA KosonganRaden Mas RiyoNo ratings yet
- KEL.B2.1 ARS 102 IPC Final-1Document22 pagesKEL.B2.1 ARS 102 IPC Final-1Reny NapitupuluNo ratings yet
- KEL.B2.1 ARS 102 IPC Final-1Document22 pagesKEL.B2.1 ARS 102 IPC Final-1Reny NapitupuluNo ratings yet
- Penelitian Tentang Word of Mouth Prof EndangDocument6 pagesPenelitian Tentang Word of Mouth Prof EndangNurul Azizatus SolehahNo ratings yet
- Penelitian Tentang Word of Mouth Prof EndangDocument6 pagesPenelitian Tentang Word of Mouth Prof EndangNurul Azizatus SolehahNo ratings yet
- BMC Health Services Research: Replacing The Projected Retiring Baby Boomer Nursing Cohort 2001 - 2026Document6 pagesBMC Health Services Research: Replacing The Projected Retiring Baby Boomer Nursing Cohort 2001 - 2026Reny NapitupuluNo ratings yet
- Jurnal Ibu RinaDocument16 pagesJurnal Ibu RinaReny NapitupuluNo ratings yet
- BMC Health Services ResearchDocument14 pagesBMC Health Services ResearchReny NapitupuluNo ratings yet
- BMC Health Services ResearchDocument10 pagesBMC Health Services ResearchReny NapitupuluNo ratings yet
- BMC Health Services ResearchDocument11 pagesBMC Health Services ResearchReny NapitupuluNo ratings yet
- 51 Power SteeringDocument72 pages51 Power Steeringlymeng porNo ratings yet
- Vampire Stories in GreeceDocument21 pagesVampire Stories in GreeceΓιώργος ΣάρδηςNo ratings yet
- BeadsDocument8 pagesBeadsMukesh MonuNo ratings yet
- (English (Auto-Generated) ) Reviving The Labor Movement - Margaret Levi - TEDxSeattle (DownSub - Com)Document14 pages(English (Auto-Generated) ) Reviving The Labor Movement - Margaret Levi - TEDxSeattle (DownSub - Com)Surat PEHKTNo ratings yet
- Pdic LawDocument30 pagesPdic LawDadangNo ratings yet
- TRW WHP PDFDocument20 pagesTRW WHP PDFmonica_codNo ratings yet
- IEC 61850 Configuration of A Phoenix Contact IED: User ManualDocument68 pagesIEC 61850 Configuration of A Phoenix Contact IED: User ManualHarold PuinNo ratings yet
- Perceptions of Organizational Structure in The Hospitality IndustryDocument11 pagesPerceptions of Organizational Structure in The Hospitality IndustryLeah Williams100% (1)
- Partnership Dissolution QuizDocument8 pagesPartnership Dissolution QuizLee SuarezNo ratings yet
- Ceramic Foam Filter PDFDocument4 pagesCeramic Foam Filter PDFPaen ZulkifliNo ratings yet
- MTSC QuestionsDocument8 pagesMTSC QuestionsAbhi RamNo ratings yet
- NIMS University Jaipur - Ph.D. Economics Selection Process, Course Fee, PlacementDocument6 pagesNIMS University Jaipur - Ph.D. Economics Selection Process, Course Fee, PlacementstepincollegeNo ratings yet
- Oracle Analytics Cloud 2018 Solution Engineer Specialist AssessmentDocument4 pagesOracle Analytics Cloud 2018 Solution Engineer Specialist AssessmentRamón MedinaNo ratings yet
- Pas 220Document71 pagesPas 220JuwitaNo ratings yet
- Introduction To Robotics: Why Build Robots?Document10 pagesIntroduction To Robotics: Why Build Robots?api-115728880No ratings yet
- Jane Austen's Literary StyleDocument4 pagesJane Austen's Literary StyleGulfam RashidNo ratings yet
- Sec. Gr. To BT History Temp Panel 2013Document50 pagesSec. Gr. To BT History Temp Panel 2013edwin_prakash75No ratings yet
- Commodities Storage V CADocument4 pagesCommodities Storage V CAElah ViktoriaNo ratings yet
- B IngDocument2 pagesB IngsyfnanyNo ratings yet
- Course Registration Slip MBA 2023Document3 pagesCourse Registration Slip MBA 2023Piyush RaghuwanshiNo ratings yet
- En Subject C08Document13 pagesEn Subject C08jmolfigueiraNo ratings yet
- Arctic Monkeys Do I Wanna KnowDocument4 pagesArctic Monkeys Do I Wanna KnowElliot LangfordNo ratings yet
- Handout-Wisdom QuestionsDocument1 pageHandout-Wisdom Questionsapi-369459770No ratings yet
- Detailed 200L Course OutlineDocument8 pagesDetailed 200L Course OutlineBoluwatife OloyedeNo ratings yet
- Data Center Cooling Solutions That Lower Costs With High Energy SavingsDocument5 pagesData Center Cooling Solutions That Lower Costs With High Energy Savingskhamsone pengmanivongNo ratings yet
- ITC Gardenia LavendreriaDocument6 pagesITC Gardenia LavendreriaMuskan AgarwalNo ratings yet
- Sindhi 2020Document1 pageSindhi 2020Engr Javed AkhtarNo ratings yet