You might also like
- Is It ADHD or Autism or BothDocument4 pagesIs It ADHD or Autism or BothTony Blair100% (1)
- Foot & Ankle PearlsDocument167 pagesFoot & Ankle PearlsPamela Hong100% (3)
- Maxillary Injection Techniques PPT I Sas 11-14Document45 pagesMaxillary Injection Techniques PPT I Sas 11-14mavirosemandawe08No ratings yet
- Minor Oral Surgical Procedures in Children ClassDocument65 pagesMinor Oral Surgical Procedures in Children ClassReenaChauhanNo ratings yet
- Post-Extraction Complications: Presented By, Abirami. K CrriDocument32 pagesPost-Extraction Complications: Presented By, Abirami. K Crriabi2189No ratings yet
- Bound Tree Active Shooter Response EbookDocument17 pagesBound Tree Active Shooter Response EbookVein100% (1)
- Pulp ProtectionDocument96 pagesPulp ProtectionAssssssNo ratings yet
- Minimally Invasive Dentistr YDocument61 pagesMinimally Invasive Dentistr YnishthaNo ratings yet
- Physical Assessment Answer 16 PrintedDocument3 pagesPhysical Assessment Answer 16 PrintedJune Dumdumaya100% (2)
- Acute Periodontal Conditions: PeriodonticsDocument9 pagesAcute Periodontal Conditions: Periodonticsmonica896No ratings yet
- Complication & Failure of Implants SEMDocument82 pagesComplication & Failure of Implants SEMArchana Dubey100% (1)
- Preterm Labor and BirthDocument55 pagesPreterm Labor and BirthEcel AggasidNo ratings yet
- Endo EmergenciesDocument95 pagesEndo EmergenciesVincent SerNo ratings yet
- The Australian and New Zealand Burn AssociationDocument97 pagesThe Australian and New Zealand Burn AssociationZarah Alifani Dzulhijjah100% (1)
- 1 Endodontic EmergencyDocument106 pages1 Endodontic EmergencyAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Cestodes and Trematodes - ReviewerDocument2 pagesCestodes and Trematodes - ReviewerAnna LouisaNo ratings yet
- Dentinal HypersensitivityDocument75 pagesDentinal HypersensitivityMica BernardoNo ratings yet
- Scaling and Root PlaningDocument12 pagesScaling and Root Planingbasel alogily100% (1)
- ORAL and MAXILLOFACIAL TRAUMA - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Document17 pagesORAL and MAXILLOFACIAL TRAUMA - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Vinnie SinghNo ratings yet
- Ultrasound and clinically guided Injection techniques on the musculoskeletal systemFrom EverandUltrasound and clinically guided Injection techniques on the musculoskeletal systemNo ratings yet
- Emergency Treatment in Endodontics: By: Mai Hamdy Ass. Prof. of Endodontics, Faculty of Dentistry, Suez Canal UniversityDocument70 pagesEmergency Treatment in Endodontics: By: Mai Hamdy Ass. Prof. of Endodontics, Faculty of Dentistry, Suez Canal Universitymahmoud100% (1)
- Pengendalian Rasa SakitDocument127 pagesPengendalian Rasa SakityouareNo ratings yet
- Mid Treatment FalreupsDocument4 pagesMid Treatment FalreupsAhmed AzizaNo ratings yet
- Ba Chapter Endodontics Principles and Practice 5ed 2015 - 388Document21 pagesBa Chapter Endodontics Principles and Practice 5ed 2015 - 388Mahdy AlShammariNo ratings yet
- 17 Osteomyelitis 140703140815 Phpapp02Document58 pages17 Osteomyelitis 140703140815 Phpapp02drkavintNo ratings yet
- 7a. Caria Complicata-PulpotomiaDocument64 pages7a. Caria Complicata-PulpotomiaNia AdibNo ratings yet
- Mingival Curettage PDFDocument52 pagesMingival Curettage PDFheycoolalexNo ratings yet
- Periodontal EmergenciesDocument47 pagesPeriodontal EmergenciesSubramanyam AarthiNo ratings yet
- Publication 11 16797 1880 PDFDocument49 pagesPublication 11 16797 1880 PDFMineet KaulNo ratings yet
- Dental PulpDocument112 pagesDental PulpLuciano AbbaNo ratings yet
- Article 1452106206 PDFDocument5 pagesArticle 1452106206 PDFYosu Obok HermanlieNo ratings yet
- Emergency Endodontics 1Document3 pagesEmergency Endodontics 1098 - SILVYARA AYU PRATIWINo ratings yet
- Trephination For AcuteDocument3 pagesTrephination For AcuteDr.Ibrahim Al-QwizanyNo ratings yet
- ENDODONTIC EMERGENCIES MitaliDocument31 pagesENDODONTIC EMERGENCIES MitalianmolNo ratings yet
- Pulpal Emergency SeminarDocument44 pagesPulpal Emergency SeminarHoda ZainNo ratings yet
- PeriapikalDocument7 pagesPeriapikalHanindyaNoorAgusthaNo ratings yet
- Enlargement Gingiva Treatment On Teeth 11 and 21Document18 pagesEnlargement Gingiva Treatment On Teeth 11 and 21Silva Eliana AspriyantiNo ratings yet
- Local AnesthesiaDocument27 pagesLocal AnesthesiaHudh HudNo ratings yet
- Blue Modern Medical - Health PresentationDocument22 pagesBlue Modern Medical - Health Presentationكرم الباريNo ratings yet
- Oralmucocele AcasereportDocument5 pagesOralmucocele AcasereportxxxNo ratings yet
- Complications of Local AnesthesiaDocument59 pagesComplications of Local AnesthesiaNishithaNo ratings yet
- Endodontics (31 Questions) : Pulpal DiseaseDocument51 pagesEndodontics (31 Questions) : Pulpal DiseaseTayaba Naim KhanNo ratings yet
- Dental PulpDocument112 pagesDental PulpRoja LakshmiNo ratings yet
- ProP TropicalSerumforTreatmentDocument4 pagesProP TropicalSerumforTreatmentGhita Andreea-IoanaNo ratings yet
- Bài điều trị tủy răngDocument3 pagesBài điều trị tủy răngMai MinhNo ratings yet
- 5phase II Periodontal TherapyDocument54 pages5phase II Periodontal TherapyKaraz StudiosNo ratings yet
- Management of Pericoronitis of Newly-Erupted Permanent Tooth Using ElectrosurgeryDocument4 pagesManagement of Pericoronitis of Newly-Erupted Permanent Tooth Using ElectrosurgeryLatifa Hanif ZuhriNo ratings yet
- Lecture3Y4S7 ENGDocument25 pagesLecture3Y4S7 ENGShany SchwarzwaldNo ratings yet
- Blue Modern Medical - Health Presentation - 2Document22 pagesBlue Modern Medical - Health Presentation - 2كرم الباريNo ratings yet
- Occlusion in Endodontic Management: Cases: Role of Report ofDocument6 pagesOcclusion in Endodontic Management: Cases: Role of Report ofSophia SaudNo ratings yet
- Neurological Disturbances of FaceDocument33 pagesNeurological Disturbances of FaceDrMuskan AroraNo ratings yet
- ENGanesthesiamaxillaryDocument25 pagesENGanesthesiamaxillaryRoxanaAnaHociungNo ratings yet
- Nervio AlveolarDocument3 pagesNervio AlveolarLuis GustavoNo ratings yet
- Capsular Pain: Submitted by DR - Amithbabu Mscd-EndoDocument17 pagesCapsular Pain: Submitted by DR - Amithbabu Mscd-EndoDR.AMITHBABU.C.BNo ratings yet
- Tema 14Document15 pagesTema 14EstreLLA ValenciaNo ratings yet
- Endodontic EmergenciesDocument12 pagesEndodontic EmergenciesnimNo ratings yet
- Pain ControlDocument88 pagesPain ControlShubham KingraNo ratings yet
- Oral SurgeryDocument52 pagesOral Surgerykhaled alahmadNo ratings yet
- Pemphigus Vulgaris and Mucous Membrane Pemphigoid: Dis-Similarly Similar LesionsDocument9 pagesPemphigus Vulgaris and Mucous Membrane Pemphigoid: Dis-Similarly Similar LesionsarushNo ratings yet
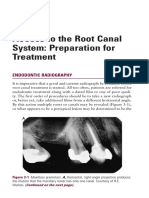
- Access To The Root Canal System: Preparation For Treatment: Endodontic RadiographyDocument13 pagesAccess To The Root Canal System: Preparation For Treatment: Endodontic RadiographyMonika LohakpureNo ratings yet
- Gingival CurettageDocument29 pagesGingival Curettagesahad100% (1)
- Gingival Tissue ManagementDocument144 pagesGingival Tissue ManagementMakkapati AmaniNo ratings yet
- InterpretDocument4 pagesInterpretAdzkia Dheyatika AsriNo ratings yet
- Injection Technique: Kirana Lina G., DRGDocument45 pagesInjection Technique: Kirana Lina G., DRGFinnyalfNo ratings yet
- Physicalandchemicalinjuriesoforalcavity 180120174153Document71 pagesPhysicalandchemicalinjuriesoforalcavity 180120174153draryajyoti1No ratings yet
- Periodontal Abscess and Periodontal DressingsDocument51 pagesPeriodontal Abscess and Periodontal DressingsHassan QadeerNo ratings yet
- External Dacryocystorhinostomy - DCR - Surgery TechniqueDocument14 pagesExternal Dacryocystorhinostomy - DCR - Surgery TechniquekityamuwesiNo ratings yet
- Amir Mirhagi - Role ModelingDocument12 pagesAmir Mirhagi - Role ModelingBiju P NairNo ratings yet
- SimulationDocument2 pagesSimulationBiju P NairNo ratings yet
- AndragogyDocument2 pagesAndragogyBiju P NairNo ratings yet
- IGADC Refresher - Part 1Document53 pagesIGADC Refresher - Part 1Biju P NairNo ratings yet
- Cone Beam Computed Tomography in Endodontics - A Review of The LiteratureDocument15 pagesCone Beam Computed Tomography in Endodontics - A Review of The LiteratureBiju P NairNo ratings yet
- Kerala Public Service Commission E: Xamination Programme For The Month of JANUARY 2020Document13 pagesKerala Public Service Commission E: Xamination Programme For The Month of JANUARY 2020Biju P NairNo ratings yet
- Dated, Thiruvananthapuram, 11th July 2012. Sub:-Medical Reimbursement-Further Instructions-Issued-RegardingDocument10 pagesDated, Thiruvananthapuram, 11th July 2012. Sub:-Medical Reimbursement-Further Instructions-Issued-RegardingBiju P NairNo ratings yet
- RL 411 2019 Ssii PDFDocument1 pageRL 411 2019 Ssii PDFBiju P NairNo ratings yet
- Breast Cancer Screening ResDocument7 pagesBreast Cancer Screening Resomegasauron0gmailcomNo ratings yet
- Personal Grooming & Fitness-Online Written AssignmentDocument5 pagesPersonal Grooming & Fitness-Online Written AssignmentChanchal Kumari100% (1)
- Hope - 1 Grade 11: Exercise For FitnessDocument12 pagesHope - 1 Grade 11: Exercise For FitnessSonnel CalmaNo ratings yet
- Colposcopy, Cervical Screening, and HPV, An Issue of Obstetrics and Gynecology Clinics (The Clinics - Internal Medicine)Document155 pagesColposcopy, Cervical Screening, and HPV, An Issue of Obstetrics and Gynecology Clinics (The Clinics - Internal Medicine)Annca RoXanna100% (1)
- DefibrillatorDocument17 pagesDefibrillatorsamuellivingston100% (1)
- Daft Arp Us TakaDocument3 pagesDaft Arp Us Takaudinamin1007No ratings yet
- Asthma Case Study Complet.Document2 pagesAsthma Case Study Complet.robertobuezo2No ratings yet
- World Health Organisation: - Dr.P.R.Thirumalai KumarDocument55 pagesWorld Health Organisation: - Dr.P.R.Thirumalai KumarMadhumithaa SelvarajanNo ratings yet
- Long Face: New Proposals For Taxonomy, Diagnosis, TreatmentDocument10 pagesLong Face: New Proposals For Taxonomy, Diagnosis, TreatmentnikitaNo ratings yet
- Concept Map Cabg PTDocument8 pagesConcept Map Cabg PTapi-607926939No ratings yet
- School Health & Preventive Care Programs in India Jarma WellnessDocument3 pagesSchool Health & Preventive Care Programs in India Jarma WellnessJarma WellnessNo ratings yet
- Cystic FibrosisDocument14 pagesCystic FibrosisAishistic thingsNo ratings yet
- The Boston C StoryDocument3 pagesThe Boston C StoryVincent John RigorNo ratings yet
- Zoo Dentists - Quiz NATALY YULIET GOMEZ CHAGUA PDFDocument2 pagesZoo Dentists - Quiz NATALY YULIET GOMEZ CHAGUA PDFNATALYYULIETNo ratings yet
- Finshed Profread Preboard NCM1Document29 pagesFinshed Profread Preboard NCM1imyutheyu07No ratings yet
- Tube Shunt Procedure StepsDocument3 pagesTube Shunt Procedure StepsAlex YoungNo ratings yet
- Reaction PaperDocument5 pagesReaction PaperSophia LiteratoNo ratings yet
- Karakteristik ISK DI RUMAH SAKIT MARTHADocument7 pagesKarakteristik ISK DI RUMAH SAKIT MARTHAAndi Ridhah NANo ratings yet
- Skip To MainDocument35 pagesSkip To MainAnonymous DqeRReNo ratings yet
- Klasifikasi Tumor Jaringan Lunak PDFDocument10 pagesKlasifikasi Tumor Jaringan Lunak PDFzakibonnie100% (1)
- Meningismus Vs MeningitisDocument19 pagesMeningismus Vs MeningitisRanna HertenizaNo ratings yet
- MirasolDocument7 pagesMirasolJan Chrispian MirasolNo ratings yet
- Soal USM STAN 2014 - Kunci Jawaban-1Document6 pagesSoal USM STAN 2014 - Kunci Jawaban-1mochshenNo ratings yet