You might also like
- Metaheuristics Algorithms for Medical Applications: Methods and ApplicationsFrom EverandMetaheuristics Algorithms for Medical Applications: Methods and ApplicationsNo ratings yet
- Magnetic Resonance Imaging: Recording, Reconstruction and AssessmentFrom EverandMagnetic Resonance Imaging: Recording, Reconstruction and AssessmentRating: 5 out of 5 stars5/5 (1)
- Final Complete Group7 1Document16 pagesFinal Complete Group7 1api-543862133No ratings yet
- Draft IIDocument11 pagesDraft IIapi-534702185No ratings yet
- Paper Draft2 Group7080821Document11 pagesPaper Draft2 Group7080821Amber CoffeyNo ratings yet
- Draft IDocument6 pagesDraft Iapi-534702185No ratings yet
- Research ProposalDocument4 pagesResearch Proposalapi-534702185No ratings yet
- Outline Group7 Final-EditDocument14 pagesOutline Group7 Final-EditAmber CoffeyNo ratings yet
- (NO) Chỉ nói về mấy thí nghiệm lâm sàng là chủ yếu, công nghệ cadcam không có gì nổi trộiDocument7 pages(NO) Chỉ nói về mấy thí nghiệm lâm sàng là chủ yếu, công nghệ cadcam không có gì nổi trộiNguyễn Đức TuấnNo ratings yet
- Bhandari2020 PaperDocument24 pagesBhandari2020 PapersaraswathiNo ratings yet
- Nihms 1556035Document17 pagesNihms 1556035ayed latifaNo ratings yet
- Comparison of Automated Grading of Digital Orthodontic Models and Hand Grading of 3-Dimensionally Printed ModelsDocument5 pagesComparison of Automated Grading of Digital Orthodontic Models and Hand Grading of 3-Dimensionally Printed ModelsGabriela Lou GomezNo ratings yet
- User-Guided 3D Active Contour Segmentation of Anatomical Structures: Significantly Improved Efficiency and ReliabilityDocument49 pagesUser-Guided 3D Active Contour Segmentation of Anatomical Structures: Significantly Improved Efficiency and ReliabilityNicholas KimNo ratings yet
- 11.deep Learning Applications in Medical Image Analysis-Brain TumorDocument4 pages11.deep Learning Applications in Medical Image Analysis-Brain TumorVenky Naidu BalineniNo ratings yet
- Out - 12 RadiologiDocument8 pagesOut - 12 RadiologiFelisiana KasmanNo ratings yet
- Research Paper RadiologyDocument8 pagesResearch Paper Radiologypolekymelyh3100% (1)
- EHF2017 EK FinalPaperDocument9 pagesEHF2017 EK FinalPaperdanimalxNo ratings yet
- JPNR - Regular Issue 03 - 357 PDFDocument8 pagesJPNR - Regular Issue 03 - 357 PDFAyesha NaeemNo ratings yet
- An Evolutionary Artificial Neural Networks Approach For Breast Cancer DiagnosisDocument30 pagesAn Evolutionary Artificial Neural Networks Approach For Breast Cancer DiagnosisSandeep ChaurasiaNo ratings yet
- Three-Dimensional Printing in Cleft CareDocument13 pagesThree-Dimensional Printing in Cleft CareBedah Mulut dan Maksilofasial 2023No ratings yet
- Association For Academic Surgery Virtual Pelvic Anatomy Simulator: A Pilot Study of Usability and Perceived EffectivenessDocument5 pagesAssociation For Academic Surgery Virtual Pelvic Anatomy Simulator: A Pilot Study of Usability and Perceived Effectivenesstri1994No ratings yet
- IJCD 1804 en Becker Jakstat Ahlers SCREEN-mWM-PUBLISH PDFDocument14 pagesIJCD 1804 en Becker Jakstat Ahlers SCREEN-mWM-PUBLISH PDFJames LinNo ratings yet
- Erekat 2019Document16 pagesErekat 2019ayed latifaNo ratings yet
- ComparingScannerPrecision FinalDocument23 pagesComparingScannerPrecision Finalnegmenas2No ratings yet
- Operating Room SchedulingDocument20 pagesOperating Room SchedulingPrashanth Natarajan IyerNo ratings yet
- Pso 1Document21 pagesPso 1Goran WnisNo ratings yet
- Ultrasound Machine Research PaperDocument5 pagesUltrasound Machine Research Paperpukytij0wyg3100% (1)
- Thesis ProposalDocument21 pagesThesis Proposalniazpocof1No ratings yet
- Using Lean Principles To Optimise Inpatient Phlebotomy ServicesDocument7 pagesUsing Lean Principles To Optimise Inpatient Phlebotomy ServicesMuizzuddin MuizNo ratings yet
- Laryngoscope Investig Oto - 2018 - Corbett - Identifying and Reducing Risks in Functional Endoscopic Sinus Surgery ThroughDocument8 pagesLaryngoscope Investig Oto - 2018 - Corbett - Identifying and Reducing Risks in Functional Endoscopic Sinus Surgery ThroughIrisNo ratings yet
- Automated Radiation Treatment Planning For CervicaDocument8 pagesAutomated Radiation Treatment Planning For CervicaPutripurwo8664No ratings yet
- Thomson Reuters Indexing JournalsDocument7 pagesThomson Reuters Indexing JournalssanaNo ratings yet
- Final DraftDocument18 pagesFinal Draftapi-334402872No ratings yet
- Group 8 Research Proposal FinalDocument4 pagesGroup 8 Research Proposal Finalapi-575870032No ratings yet
- Radiation Planning Assistant - A Streamlined, Fully Automated Radiotherapy Treatment Planning SystemDocument9 pagesRadiation Planning Assistant - A Streamlined, Fully Automated Radiotherapy Treatment Planning Systemdrrajeshb77No ratings yet
- Base PaperDocument21 pagesBase Paper023-Subha KNo ratings yet
- TSP CMC 41333Document14 pagesTSP CMC 41333KEZZIA MAE ABELLANo ratings yet
- Automatic Recognition of Handwritten Medical Forms For Search EnginesDocument16 pagesAutomatic Recognition of Handwritten Medical Forms For Search EnginesAbhinav AnandNo ratings yet
- Performance Evaluation of Image Processing Algorithms in CadeDocument14 pagesPerformance Evaluation of Image Processing Algorithms in CadePAUL AKAMPURIRANo ratings yet
- A Computational Model The Human Hand 93-ERI-053: K. Hollerbach, P.I. T. Axelrod, Original P.IDocument14 pagesA Computational Model The Human Hand 93-ERI-053: K. Hollerbach, P.I. T. Axelrod, Original P.ISunčica Milan Otović BlagojevićNo ratings yet
- Dose Differences Due To Variance in Contours of The Optic ChiasmDocument15 pagesDose Differences Due To Variance in Contours of The Optic Chiasmapi-527662950No ratings yet
- Thrall 2014Document5 pagesThrall 2014Rudi IlhamsyahNo ratings yet
- Jurnal English 1Document16 pagesJurnal English 1Riska KurniawatiNo ratings yet
- Brain TumourDocument39 pagesBrain TumourCharitha IddumNo ratings yet
- A Comparative Study On Use of Manual Versus Digital Method Using Mobile Application For Cephalometric MeasurementsDocument6 pagesA Comparative Study On Use of Manual Versus Digital Method Using Mobile Application For Cephalometric MeasurementsBeniyaNo ratings yet
- A Case Study of Multiple Maintenance Efficacy in Gynaecological Surgery Assessed by Deep Learning 99Document21 pagesA Case Study of Multiple Maintenance Efficacy in Gynaecological Surgery Assessed by Deep Learning 99vinitaveeraniNo ratings yet
- Reliability of A Powerpoint Method For Wear Measurement After Total Hip ArthroplastyDocument8 pagesReliability of A Powerpoint Method For Wear Measurement After Total Hip Arthroplastyfahrul muhammadNo ratings yet
- Medical Insurance CostDocument12 pagesMedical Insurance CostKumara SNo ratings yet
- An Automated Medical Duties Scheduling System Using Queing Techniques (Chapter 1-5)Document19 pagesAn Automated Medical Duties Scheduling System Using Queing Techniques (Chapter 1-5)ABUBSAKAR SIDIQ AMINUNo ratings yet
- Nihms 1903570Document20 pagesNihms 1903570sam mehraNo ratings yet
- Ef Ficiency and Safety Increases After The Implementation of A Multi Institutional Automated Plan Check Tool at Our InstitutionDocument8 pagesEf Ficiency and Safety Increases After The Implementation of A Multi Institutional Automated Plan Check Tool at Our InstitutionAshok PokhrelNo ratings yet
- Quality Prediction Model For Drug Classification Using Machine Learning AlgorithmDocument11 pagesQuality Prediction Model For Drug Classification Using Machine Learning AlgorithmIJRASETPublicationsNo ratings yet
- Chapter 2 Literature Review: Describes ThatDocument26 pagesChapter 2 Literature Review: Describes Thatabusyed alhasanNo ratings yet
- Research Article: Automated Quantification of Pneumothorax in CTDocument8 pagesResearch Article: Automated Quantification of Pneumothorax in CTAnnisa HidayatiNo ratings yet
- J Applied Clin Med Phys - 2022 - Nealon - Development and Validation of A Checklist For Use With Automatically GeneratedDocument7 pagesJ Applied Clin Med Phys - 2022 - Nealon - Development and Validation of A Checklist For Use With Automatically GeneratedAli EssadokNo ratings yet
- An Evolutionary Artificial Neural Networks Approach For Breast Cancer DiagnosisDocument30 pagesAn Evolutionary Artificial Neural Networks Approach For Breast Cancer DiagnosisegondragonNo ratings yet
- Electronic Patient Record Use During Ward Rounds: A Qualitative Study of Interaction Between Medical StaffDocument8 pagesElectronic Patient Record Use During Ward Rounds: A Qualitative Study of Interaction Between Medical StaffpsikubNo ratings yet
- A Comparison of Cephalometric Measurements Obtained Using Conventional and Digital MethodsDocument7 pagesA Comparison of Cephalometric Measurements Obtained Using Conventional and Digital MethodsNereo LopezNo ratings yet
- Healthcare 10 01518Document24 pagesHealthcare 10 01518ayed latifaNo ratings yet
- Towards best practice in the Archetype Development ProcessFrom EverandTowards best practice in the Archetype Development ProcessNo ratings yet
- Outline Group7 Final-EditDocument14 pagesOutline Group7 Final-EditAmber CoffeyNo ratings yet
- Amber Coffey, M.S, R.T. (R) (T) (CT) (Arrt)Document2 pagesAmber Coffey, M.S, R.T. (R) (T) (CT) (Arrt)Amber CoffeyNo ratings yet
- ILS Amber CoffeyDocument3 pagesILS Amber CoffeyAmber CoffeyNo ratings yet
- Phase II - Research Organization Document - Group& FinalDocument4 pagesPhase II - Research Organization Document - Group& FinalAmber CoffeyNo ratings yet
- Mantle Competency Amber CoffeyDocument7 pagesMantle Competency Amber CoffeyAmber CoffeyNo ratings yet
- ASSESSMENT IN LEARNING 2 MODULE (Finals) With POSTTESTDocument63 pagesASSESSMENT IN LEARNING 2 MODULE (Finals) With POSTTESTcreqyaqaNo ratings yet
- Jamia Millia Islamia University Faculty of LawDocument18 pagesJamia Millia Islamia University Faculty of LawShimran ZamanNo ratings yet
- Mackenzie Marr Marketing ReportDocument13 pagesMackenzie Marr Marketing Reportapi-250686425100% (2)
- Dectetor de Drones Por El SonidoDocument66 pagesDectetor de Drones Por El SonidoRodrigo ObregonNo ratings yet
- Antim Prahar Marketing Managment 2023Document25 pagesAntim Prahar Marketing Managment 2023Vineeta GautamNo ratings yet
- P.E - 16MDocument16 pagesP.E - 16M20EUEE053- MADHUBALAN.SNo ratings yet
- Dunning Objects ListsDocument1 pageDunning Objects ListsSachin SinghNo ratings yet
- MAXIMUS - 516 руководство пользователя - 1Document214 pagesMAXIMUS - 516 руководство пользователя - 1MMM-MMM100% (1)
- Issues in Economics TodayDocument559 pagesIssues in Economics TodayNikhil Singhal71% (7)
- Report On Cordect TechnologyDocument22 pagesReport On Cordect TechnologyAnkush JamthikarNo ratings yet
- Microprocessors and Microcontrollers: Unit I The 8086 Microprocessor Unit I The 8086 MicroprocessorDocument133 pagesMicroprocessors and Microcontrollers: Unit I The 8086 Microprocessor Unit I The 8086 MicroprocessornivasiniNo ratings yet
- De Thi Hoc Ky 2 Mon Tieng Anh Lop 10 Thi Diem So GD DT Binh PhuocDocument12 pagesDe Thi Hoc Ky 2 Mon Tieng Anh Lop 10 Thi Diem So GD DT Binh Phuoc17. Phạm Tuyết Nga 10HNo ratings yet
- IntegrationDocument23 pagesIntegrationnikowawaNo ratings yet
- LM123/LM223 LM323: Three-Terminal 3A-5V Positive Voltage RegulatorsDocument8 pagesLM123/LM223 LM323: Three-Terminal 3A-5V Positive Voltage Regulatorscarrasquel0No ratings yet
- Ten Common SQL Server Reporting Services Challenges and SolutionsDocument25 pagesTen Common SQL Server Reporting Services Challenges and Solutionssrisrinivas76No ratings yet
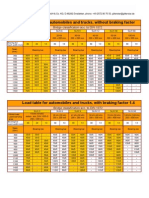
- 9 Gitterstar LoadTable Autom TrucksDocument1 page9 Gitterstar LoadTable Autom TrucksSnaz_nedainNo ratings yet
- Explanation LetterDocument1 pageExplanation LetterBebe KwahNo ratings yet
- Ket Exam 3 ListeningDocument6 pagesKet Exam 3 ListeningFranciscaBalasSuarezNo ratings yet
- Hysys Installation V 7.3Document1 pageHysys Installation V 7.3Naik LarkaNo ratings yet
- DL 256qam & Ul 64qamDocument8 pagesDL 256qam & Ul 64qamanushraj401No ratings yet
- Control System InstrumentationDocument88 pagesControl System Instrumentationyeay_meNo ratings yet
- Proof of AnsweresDocument40 pagesProof of AnsweresDream SquareNo ratings yet
- Biofuels Industry ReportDocument2 pagesBiofuels Industry ReportNiravNo ratings yet
- PapelDocument8 pagesPapelignacio galindoNo ratings yet
- ASME B31.8 Riser CalcDocument23 pagesASME B31.8 Riser Calcisrar khan100% (2)
- Government Memo On Claimed Farms - Part 1Document25 pagesGovernment Memo On Claimed Farms - Part 1noko-makgato-6232No ratings yet
- SPCO 2007 PPTDocument9 pagesSPCO 2007 PPTBerhanu Zemecha HabteNo ratings yet
- M.tech Structural Engineering Syllabus 2nd SemesterDocument5 pagesM.tech Structural Engineering Syllabus 2nd SemesterPriyankaNo ratings yet
- Chart InstallationDocument138 pagesChart InstallationPaul Lucian VentelNo ratings yet
- Bmom5203 Assignment Part 1Document15 pagesBmom5203 Assignment Part 1ALBERT AK SIPAT STUDENTNo ratings yet