You might also like
- Michelle J. Bayesky Comparação PGD EUA e EuropaDocument7 pagesMichelle J. Bayesky Comparação PGD EUA e EuropaVinicius Luiz FerreiraNo ratings yet
- Anticipating PGDDocument10 pagesAnticipating PGDArlin Chyntia DewiNo ratings yet
- Des 418Document10 pagesDes 418Saro RajeshNo ratings yet
- Self-assessment Questions for Clinical Molecular GeneticsFrom EverandSelf-assessment Questions for Clinical Molecular GeneticsRating: 5 out of 5 stars5/5 (1)
- Rega 505 Biotechnology - Designer BabiesDocument10 pagesRega 505 Biotechnology - Designer BabiesNermeen ElabiNo ratings yet
- Getting Pregnant in the 1980s: New Advances in Infertility Treatment and Sex PreselectionFrom EverandGetting Pregnant in the 1980s: New Advances in Infertility Treatment and Sex PreselectionNo ratings yet
- Aismun 2020 - Un Women Committee GuideDocument29 pagesAismun 2020 - Un Women Committee GuideLauraNo ratings yet
- Nutrigenetics: Applying the Science of Personal NutritionFrom EverandNutrigenetics: Applying the Science of Personal NutritionRating: 4.5 out of 5 stars4.5/5 (3)
- Clinical Management of Infertility: Problems and SolutionsFrom EverandClinical Management of Infertility: Problems and SolutionsJoseph G. SchenkerNo ratings yet
- Final Policy DraftDocument5 pagesFinal Policy Draftapi-319048393No ratings yet
- Practical Ethics Issues in Gene Therapy and Genetic TestingDocument9 pagesPractical Ethics Issues in Gene Therapy and Genetic TestingQueenie LouNo ratings yet
- The Advantages and Disadvantages of Assisted Reproduction and The Impact On SocietyDocument4 pagesThe Advantages and Disadvantages of Assisted Reproduction and The Impact On SocietyUsman MohsinNo ratings yet
- Moving Beyond Disrespect and Abuse Addressing The Structural Dimensions of Obstetric VioleDocument10 pagesMoving Beyond Disrespect and Abuse Addressing The Structural Dimensions of Obstetric VioleMaryNo ratings yet
- Preconception Health and Care: A Life Course ApproachFrom EverandPreconception Health and Care: A Life Course ApproachJill ShaweNo ratings yet
- Diagnostic Problems in Tumors of Gastrointestinal Tract: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Gastrointestinal Tract: Selected TopicsNo ratings yet
- Business Ethics and CSR Individual Assignment 1 Concept PaperDocument9 pagesBusiness Ethics and CSR Individual Assignment 1 Concept PaperZeeshan KhanNo ratings yet
- Life Histories of Genetic Disease: Patterns and Prevention in Postwar Medical GeneticsFrom EverandLife Histories of Genetic Disease: Patterns and Prevention in Postwar Medical GeneticsNo ratings yet
- Healthy Babies Are Worth The Wait: A Partnership to Reduce Preterm Births in Kentucky through Community-based Interventions 2007 - 2009From EverandHealthy Babies Are Worth The Wait: A Partnership to Reduce Preterm Births in Kentucky through Community-based Interventions 2007 - 2009No ratings yet
- Assisted Reproductive TechniquesDocument10 pagesAssisted Reproductive TechniquesSubhangi Lenka50% (2)
- Knowledge, Attitudes, and Perceptions of Preeclampsia Among First-Generation Nigerian Women in the United StatesFrom EverandKnowledge, Attitudes, and Perceptions of Preeclampsia Among First-Generation Nigerian Women in the United StatesNo ratings yet
- Questions From Textbook SolvedDocument3 pagesQuestions From Textbook SolvedniteeshNo ratings yet
- Perspectives: Genetic Profiling of Newborns: Ethical and Social IssuesDocument5 pagesPerspectives: Genetic Profiling of Newborns: Ethical and Social IssuesSimona CriveanuNo ratings yet
- 1 s2.0 S0015028223001425 MainDocument14 pages1 s2.0 S0015028223001425 MainMaged BedeawyNo ratings yet
- Introduction PR1 SemifinalDocument21 pagesIntroduction PR1 Semifinalalayanjoshua26No ratings yet
- Reproductive Health Policy Saga: Restrictive Abortion Laws in Low-And Middle-Income Countries (Lmics), Unnecessary Cause of Maternal MortalityDocument20 pagesReproductive Health Policy Saga: Restrictive Abortion Laws in Low-And Middle-Income Countries (Lmics), Unnecessary Cause of Maternal Mortality7 MNTNo ratings yet
- CRISPR 2018 Draft Ethical Principles JiankuiDocument3 pagesCRISPR 2018 Draft Ethical Principles JiankuiEsteban VegaNo ratings yet
- Thompson & Thompson Genetics in Medicine Genetik EthicDocument21 pagesThompson & Thompson Genetics in Medicine Genetik EthickartalxyusufNo ratings yet
- Varmus y Satcher Ethical Complexities of Conducting Research in Developing CountriesDocument8 pagesVarmus y Satcher Ethical Complexities of Conducting Research in Developing CountriesMaria RivasNo ratings yet
- Psychological Evaluations for Assisted Reproductive Intervention: Guidelines for Clinical PracticeDocument8 pagesPsychological Evaluations for Assisted Reproductive Intervention: Guidelines for Clinical PracticeandreaNo ratings yet
- Influence of Prematurity and Sex on the Health of a Child: A Transdiscliplinary ApproachFrom EverandInfluence of Prematurity and Sex on the Health of a Child: A Transdiscliplinary ApproachNo ratings yet
- The ASMBS Textbook of Bariatric Surgery: Volume 1: Bariatric SurgeryFrom EverandThe ASMBS Textbook of Bariatric Surgery: Volume 1: Bariatric SurgeryNo ratings yet
- Emery and Rimoin’s Principles and Practice of Medical Genetics and Genomics: FoundationsFrom EverandEmery and Rimoin’s Principles and Practice of Medical Genetics and Genomics: FoundationsReed E. PyeritzNo ratings yet
- Contraception for the Medically Challenging PatientFrom EverandContraception for the Medically Challenging PatientRebecca H. AllenNo ratings yet
- Activity FormDocument3 pagesActivity FormC137No ratings yet
- Puberty Blockers For Children Can They ConsentDocument25 pagesPuberty Blockers For Children Can They Consentnina.konekoNo ratings yet
- Contraception: Science and PracticeFrom EverandContraception: Science and PracticeMarcus FilshieNo ratings yet
- IVF Unveiled: A Comprehensive Guide to Fertility TreatmentsFrom EverandIVF Unveiled: A Comprehensive Guide to Fertility TreatmentsNo ratings yet
- Management of Occult GI Bleeding: A Clinical GuideFrom EverandManagement of Occult GI Bleeding: A Clinical GuideMicheal TadrosNo ratings yet
- Clinical Management of Male InfertilityFrom EverandClinical Management of Male InfertilityGiorgio CavalliniNo ratings yet
- Advances in Male Contraception: Stephanie T. Page, John K. Amory, and William J. BremnerDocument29 pagesAdvances in Male Contraception: Stephanie T. Page, John K. Amory, and William J. BremnerLinguumNo ratings yet
- Student Name Institutional Affiliation Instructor Course DateDocument4 pagesStudent Name Institutional Affiliation Instructor Course DatemogreyNo ratings yet
- Incorporating Bioethics Education into School CurriculumsFrom EverandIncorporating Bioethics Education into School CurriculumsNo ratings yet
- Ignorance Is Not Bliss: The Case For Comprehensive Reproductive Counseling For Women With Chronic Kidney DiseaseDocument14 pagesIgnorance Is Not Bliss: The Case For Comprehensive Reproductive Counseling For Women With Chronic Kidney DiseaseAnnette ChavezNo ratings yet
- Position Paper-RH Bill-Dr ManaloDocument14 pagesPosition Paper-RH Bill-Dr ManaloCBCP for LifeNo ratings yet
- Research Paper On FGMDocument7 pagesResearch Paper On FGMtgyuhdvkg100% (2)
- FibroidsFrom EverandFibroidsJames H. SegarsNo ratings yet
- Ethics and Quality Assurance in Biomedical Laboratory ScienceDocument6 pagesEthics and Quality Assurance in Biomedical Laboratory ScienceNear D'arezzo-AvengerzNo ratings yet
- Birth Defects Research PaperDocument7 pagesBirth Defects Research Paperjhwmemrhf100% (1)
- Genetics/Genomics Nursing: Scope and Standards of PracticeFrom EverandGenetics/Genomics Nursing: Scope and Standards of PracticeRating: 5 out of 5 stars5/5 (1)
- Brunke T n332 EthicalpaperDocument13 pagesBrunke T n332 Ethicalpaperapi-260168909No ratings yet
- Savior SiblingsDocument4 pagesSavior Siblingsapi-305513870No ratings yet
- PGD Article1 Department of HealthDocument11 pagesPGD Article1 Department of Healthjoeboyd10No ratings yet
- SSM10161 - Revised Proof 2015Document8 pagesSSM10161 - Revised Proof 2015Véronique MirlesseNo ratings yet
- Global database tracks abortion laws, policies and health standardsDocument6 pagesGlobal database tracks abortion laws, policies and health standardsRahmadani NabilaNo ratings yet
- 201 Files CoverDocument12 pages201 Files CoverHazel ButalNo ratings yet
- Notice seeking refund and compensation for defective Asian paintsDocument4 pagesNotice seeking refund and compensation for defective Asian paintsMr.M.Dhinakar Asst.ProfessorNo ratings yet
- Topic-1: Otto Von Bismarck's Foreign Policy: Assignment HSB-675: MODERN WORLD (1871-1992)Document7 pagesTopic-1: Otto Von Bismarck's Foreign Policy: Assignment HSB-675: MODERN WORLD (1871-1992)MOHAMAMD ZIYA ANSARINo ratings yet
- Regulations of The Occupational Health and Safety DepartmentDocument62 pagesRegulations of The Occupational Health and Safety DepartmentCruz CruzNo ratings yet
- ACCA AA (F8) Course Notes PDFDocument258 pagesACCA AA (F8) Course Notes PDFayesha najam100% (2)
- En Banc: Romeo A. Zarcilla and Marita Bumanglag, Complainants, V. Atty. Jose C. Quesada, JR., Respondent. DecisionDocument11 pagesEn Banc: Romeo A. Zarcilla and Marita Bumanglag, Complainants, V. Atty. Jose C. Quesada, JR., Respondent. DecisionM A J esty FalconNo ratings yet
- (G.r. No. 1503, March 14, 1905) Us Vs RavidasDocument7 pages(G.r. No. 1503, March 14, 1905) Us Vs RavidasDonna Grace GuyoNo ratings yet
- Additional ClausesDocument13 pagesAdditional ClausesPankaj GuptaNo ratings yet
- DEED OF ASSIGNMENT of Shares of Stocks (Draft)Document2 pagesDEED OF ASSIGNMENT of Shares of Stocks (Draft)Darryl Jay MedinaNo ratings yet
- Elie Wiesel - Night NotesDocument3 pagesElie Wiesel - Night NotesFrancisco Solis AilonNo ratings yet
- Test Bank For Advertising and Promotion: An Integrated Marketing Communications Perspective, 12th Edition, George Belch Michael BelchDocument28 pagesTest Bank For Advertising and Promotion: An Integrated Marketing Communications Perspective, 12th Edition, George Belch Michael BelchPauline Chavez100% (12)
- CS Form No. 9 Request For Publication of Vacant Positions With Instructions jUNE 7 2019Document2 pagesCS Form No. 9 Request For Publication of Vacant Positions With Instructions jUNE 7 2019John SantoNo ratings yet
- Representations of TeenagersDocument3 pagesRepresentations of TeenagersSaaemaxoNo ratings yet
- Vander Nat and Keep - MLM 2002Document13 pagesVander Nat and Keep - MLM 2002Bill KeepNo ratings yet
- Constitutional Law 4Document33 pagesConstitutional Law 4Glen Mark SimbilloNo ratings yet
- Auditing Theory RA 9298 Auditing Theory RA 9298Document10 pagesAuditing Theory RA 9298 Auditing Theory RA 9298sninaricaNo ratings yet
- Maserati Granturismo Coupe 4 2l 2009 2018 Workshop Manual Wiring DiagramsDocument22 pagesMaserati Granturismo Coupe 4 2l 2009 2018 Workshop Manual Wiring Diagramschristopherwhite251290ywa100% (111)
- Certificate of Increase in Capital Stock-Sample FormDocument2 pagesCertificate of Increase in Capital Stock-Sample FormvenaphaniaglysdimungcalNo ratings yet
- CCN Home Health Quick Reference GuideDocument3 pagesCCN Home Health Quick Reference GuidekciresamaNo ratings yet
- The Law on PartnershipDocument22 pagesThe Law on PartnershipLorjyll Shyne Luberanes TomarongNo ratings yet
- People v. VergaraDocument2 pagesPeople v. VergaraVoid LessNo ratings yet
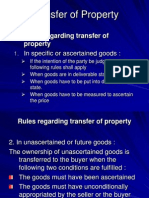
- Transfer of PropertyDocument13 pagesTransfer of PropertyPrashanth GowdaNo ratings yet
- ALARM DEVICE-Science FairDocument15 pagesALARM DEVICE-Science FairJesnefa JovitaNo ratings yet
- Professional Conduct and Ethical Module 3Document10 pagesProfessional Conduct and Ethical Module 3moradasj0502No ratings yet
- Sabelo J Ndlovugatsheni Global Coloniality and The Challenges of Creating African Futures PDFDocument22 pagesSabelo J Ndlovugatsheni Global Coloniality and The Challenges of Creating African Futures PDFJakub CzmychNo ratings yet
- Goku Hakaishin Plantillas RexpapersDocument46 pagesGoku Hakaishin Plantillas RexpapersjoseNo ratings yet
- Motion For Discovery of An Injury in Fact To Prove Personal JurisdictionDocument13 pagesMotion For Discovery of An Injury in Fact To Prove Personal JurisdictionDavid Dienamik89% (9)
- Karla Vargas Prada guideDocument2 pagesKarla Vargas Prada guideKarla Stephany VARGAS PRADANo ratings yet
- (II) Ibn KhaldunDocument17 pages(II) Ibn KhaldunAdnan RaheemNo ratings yet
- gpujpthjp rk;kd; - Notice of Hearing in a Summary SuitDocument25 pagesgpujpthjp rk;kd; - Notice of Hearing in a Summary Suitsharanmit6630No ratings yet