You might also like
- Printable Tarot Card Meanings Reference GuideDocument6 pagesPrintable Tarot Card Meanings Reference Guidesonam100% (4)
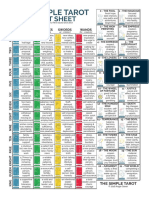
- The Simple Tarot: Cheat SheetDocument1 pageThe Simple Tarot: Cheat Sheetmonk100% (4)
- Abraham, Sylvia - How To Read The TarotDocument276 pagesAbraham, Sylvia - How To Read The Tarotchukchev100% (27)
- Printable TarotDocument20 pagesPrintable Tarottsililouli100% (2)
- Oracle of Mystical MomentsDocument48 pagesOracle of Mystical Momentsmashke8250% (2)
- Veterinary Virology PDFDocument96 pagesVeterinary Virology PDFShem Peter Mutua Mutuiri100% (1)
- Covid-19: Characteristics and TherapeuticsDocument29 pagesCovid-19: Characteristics and TherapeuticsHelenaNo ratings yet
- COVID-19: Pathophysiology of Acute Disease 1: SeriesDocument21 pagesCOVID-19: Pathophysiology of Acute Disease 1: SeriesMyatnoe KhinNo ratings yet
- Critical Reviews in Clinical Laboratory Sciences explores COVID-19 variants and vaccine efficacyDocument11 pagesCritical Reviews in Clinical Laboratory Sciences explores COVID-19 variants and vaccine efficacy别康民No ratings yet
- COVID-19: Pathophysiology of Acute Disease 1: SeriesDocument20 pagesCOVID-19: Pathophysiology of Acute Disease 1: SerieswiwiNo ratings yet
- Better Strategies For Covid VaccinationsDocument8 pagesBetter Strategies For Covid VaccinationsMiguel Angel Vilar HerreroNo ratings yet
- Toward Nanotechnology-Enabled Approaches Against The COVID-19 PandemicDocument24 pagesToward Nanotechnology-Enabled Approaches Against The COVID-19 Pandemicmadcraft9832No ratings yet
- Corona Virus VaccineDocument19 pagesCorona Virus VaccinekanazNo ratings yet
- Comparing The Clinical Efficacy of COVID 19 Vaccines: A Systematic Review and Network Meta AnalysisDocument9 pagesComparing The Clinical Efficacy of COVID 19 Vaccines: A Systematic Review and Network Meta AnalysisLieblingsmensch andipaNo ratings yet
- Acad Dermatol Venereol - 2021 - Gambichler - Cutaneous Findings Following COVID 19 Vaccination Review of World LiteratureDocument9 pagesAcad Dermatol Venereol - 2021 - Gambichler - Cutaneous Findings Following COVID 19 Vaccination Review of World LiteratureRoxanne KapNo ratings yet
- Cost Utility of Vaccination Against COVID-19 in BrazilDocument8 pagesCost Utility of Vaccination Against COVID-19 in BrazilTatiana DutraNo ratings yet
- Cureus 0015 00000045638Document7 pagesCureus 0015 00000045638SIVA P MNo ratings yet
- Ijmm 46 1 3 PDFDocument14 pagesIjmm 46 1 3 PDFmwdhtirahNo ratings yet
- Impact of COVID-19 Vaccination On Varicella Zoster Virus Reactivation: A Case Control StudyDocument7 pagesImpact of COVID-19 Vaccination On Varicella Zoster Virus Reactivation: A Case Control StudyPedroNo ratings yet
- PIIS1198743X21003670Document6 pagesPIIS1198743X21003670PanosNo ratings yet
- COVID-19 Vaccination Efficacy and Safety Literature Review: ArticleDocument19 pagesCOVID-19 Vaccination Efficacy and Safety Literature Review: ArticleBasma AboalezzNo ratings yet
- DNA Vaccines Against COVID 19 Perspectives and Challenges - 2021 - Life ScienceDocument7 pagesDNA Vaccines Against COVID 19 Perspectives and Challenges - 2021 - Life SciencePaoloMafaldoNo ratings yet
- Vaccines For COVID-19 - The Current State of Play PDFDocument8 pagesVaccines For COVID-19 - The Current State of Play PDFdiana.alyNo ratings yet
- Myocarditis Following COVID-19 VaccineDocument19 pagesMyocarditis Following COVID-19 VaccineVirginia Hernandez100% (1)
- COVID-19 Vaccination Efficacy and Safety Literature Review: Journal of Clinical and Medical Research February 2021Document19 pagesCOVID-19 Vaccination Efficacy and Safety Literature Review: Journal of Clinical and Medical Research February 2021guanellaNo ratings yet
- Stem Cell Based Therapy Option in COVID-19 - Is It Really Promising?Document17 pagesStem Cell Based Therapy Option in COVID-19 - Is It Really Promising?diana.alyNo ratings yet
- Prevalence of Reactogenicity of COVID-19 Vaccine Among Libyan Adults: A Cross-Sectional StudyDocument6 pagesPrevalence of Reactogenicity of COVID-19 Vaccine Among Libyan Adults: A Cross-Sectional StudyMediterr J Pharm Pharm SciNo ratings yet
- COVID-19 Vaccines To Prevent SARS-CoV-2 Infection - UpToDateDocument86 pagesCOVID-19 Vaccines To Prevent SARS-CoV-2 Infection - UpToDateXochilt Mejia GarciaNo ratings yet
- VaccineDocument9 pagesVaccineSarha MuñozNo ratings yet
- Mrna12 3Document14 pagesMrna12 3Annisa UlfaNo ratings yet
- 2023 11 15 23298565v1 FullDocument30 pages2023 11 15 23298565v1 FullgeosminNo ratings yet
- Mesenchymal Stem Cells (MSCS) As A Novel Therapeutic Option For Ncovid-19-A ReviewDocument16 pagesMesenchymal Stem Cells (MSCS) As A Novel Therapeutic Option For Ncovid-19-A ReviewBala BhaskarNo ratings yet
- Clinical Characteristics and Risk Factors For The IsolationDocument7 pagesClinical Characteristics and Risk Factors For The Isolationnanang hidayatullohNo ratings yet
- 1 s2.0 S1198743X21002846 MainDocument8 pages1 s2.0 S1198743X21002846 MaindrkhengkiNo ratings yet
- COVID-19 Vaccination Efficacy and Safety Literature Review: ArticleDocument19 pagesCOVID-19 Vaccination Efficacy and Safety Literature Review: ArticlePromiseNo ratings yet
- International Immunopharmacology: Hyun Jee Han, Chinekwu Nwagwu, Obumneme Anyim, Chinedu Ekweremadu, San KimDocument11 pagesInternational Immunopharmacology: Hyun Jee Han, Chinekwu Nwagwu, Obumneme Anyim, Chinedu Ekweremadu, San KimyoshefarieNo ratings yet
- MainDocument7 pagesMainFerdous HakimNo ratings yet
- Clinical Immunology: Susanna Felsenstein, Jenny A. Herbert, Paul S. Mcnamara, Christian M. Hedrich TDocument13 pagesClinical Immunology: Susanna Felsenstein, Jenny A. Herbert, Paul S. Mcnamara, Christian M. Hedrich TIrma NeyraNo ratings yet
- COVID-19 Vaccination of Patients With Chronic Immune-Mediated Inflammatory DiseaseDocument6 pagesCOVID-19 Vaccination of Patients With Chronic Immune-Mediated Inflammatory DiseaseSangeetha VijianNo ratings yet
- Can Covid-19 Vaccines Induce Premature NCDDocument35 pagesCan Covid-19 Vaccines Induce Premature NCDAlexandra CalleNo ratings yet
- Pi Is 0161642022006728Document8 pagesPi Is 0161642022006728Anca Florina GaceaNo ratings yet
- Critococcus IDSA PDFDocument32 pagesCritococcus IDSA PDFRodrigo AriasNo ratings yet
- 1 s2.0 S0924857920301059 MainDocument13 pages1 s2.0 S0924857920301059 MainNini RinNo ratings yet
- Vaccines 11 00112Document12 pagesVaccines 11 00112Felicia SutarliNo ratings yet
- Vaccine Strategies Against COVID19: A Review of Principal Vaccines Developed in India and WorldwideDocument12 pagesVaccine Strategies Against COVID19: A Review of Principal Vaccines Developed in India and WorldwideSubhrojyoti GhoshNo ratings yet
- Serious Complications of COVID-19 Vaccines A MiniDocument6 pagesSerious Complications of COVID-19 Vaccines A MiniRaul Sebastian Tello CaveroNo ratings yet
- Efficacy and safety of COVID-19 vaccines: a systematic reviewDocument16 pagesEfficacy and safety of COVID-19 vaccines: a systematic reviewJuan Paulo P. PulancoNo ratings yet
- Angeli Et Al (2022) Blood Preassure Increase Folowwing Covid 19 Vaccination PAPER 9pDocument9 pagesAngeli Et Al (2022) Blood Preassure Increase Folowwing Covid 19 Vaccination PAPER 9pCarlos Carrasco MuñozNo ratings yet
- Study of The Prevalence of Nosocomial Infections in The University Hospital Center of Béni-Messous, Algiers in 2023 - AlgeriaDocument6 pagesStudy of The Prevalence of Nosocomial Infections in The University Hospital Center of Béni-Messous, Algiers in 2023 - AlgeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Clinical Practice Guidelines For The Management IDSADocument32 pagesClinical Practice Guidelines For The Management IDSACarlos JorgeNo ratings yet
- The Development ofDocument13 pagesThe Development ofGaspar PonceNo ratings yet
- Herpesviruses Reactivation Following COVID-19 Vaccination: A Systematic Review and Meta-AnalysisDocument15 pagesHerpesviruses Reactivation Following COVID-19 Vaccination: A Systematic Review and Meta-Analysisbekapol772No ratings yet
- Computational Chemistry To Repurposing Drugs For The Control of COVID-19Document18 pagesComputational Chemistry To Repurposing Drugs For The Control of COVID-19Mai Mohamed HasanNo ratings yet
- Demyelinating Disorders Following COVID-19 Vaccines, A VAERS-based StudyDocument9 pagesDemyelinating Disorders Following COVID-19 Vaccines, A VAERS-based StudyStephen DonovanNo ratings yet
- Artikel VaksinDocument9 pagesArtikel VaksinrajyurafNo ratings yet
- Golchin2020 Article MesenchymalStemCellTherapyForCDocument7 pagesGolchin2020 Article MesenchymalStemCellTherapyForCJuan Pablo Rodríguez CoronaNo ratings yet
- The Use of Oral Human Grade Ivermectin With Supplements Known As Immunomodulators For Treating Patients With COVID 19 Infections at HomeDocument16 pagesThe Use of Oral Human Grade Ivermectin With Supplements Known As Immunomodulators For Treating Patients With COVID 19 Infections at HomeAthenaeum Scientific PublishersNo ratings yet
- Review Article Mesenchymal Stem Cells and COVID-19: Cure, Prevention, and VaccinationDocument12 pagesReview Article Mesenchymal Stem Cells and COVID-19: Cure, Prevention, and VaccinationBala BhaskarNo ratings yet
- 2020 08 03 20167361v1 FullDocument28 pages2020 08 03 20167361v1 FullNovel SaputraNo ratings yet
- Clinical Practice Guidelines For The Management of Cryptococcal Disease: 2010 Update by The Infectious Diseases Society of AmericaDocument32 pagesClinical Practice Guidelines For The Management of Cryptococcal Disease: 2010 Update by The Infectious Diseases Society of AmericaHendrawanDianAgungWicaksanaNo ratings yet
- Nosocomial Infection of COVID 19: A New Challenge For Healthcare Professionals (Review)Document10 pagesNosocomial Infection of COVID 19: A New Challenge For Healthcare Professionals (Review)lagi magerNo ratings yet
- Vaccines For COVID-19 The Current State of PlayDocument8 pagesVaccines For COVID-19 The Current State of PlayNazmul IslamNo ratings yet
- Sinovac COVID-19 Vaccine EUL Assessment ReportDocument36 pagesSinovac COVID-19 Vaccine EUL Assessment Reportindra sanjayaNo ratings yet
- COVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsFrom EverandCOVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsNo ratings yet
- Elena Lucchi - Environmental Risk Management For Museums in Historic Buildings Through An Innovative Approach: A Case Study of The Pinacoteca Di Brera in Milan (Italy)Document22 pagesElena Lucchi - Environmental Risk Management For Museums in Historic Buildings Through An Innovative Approach: A Case Study of The Pinacoteca Di Brera in Milan (Italy)_____irisNo ratings yet
- Japanese TarotDocument29 pagesJapanese Tarotshalott4948100% (1)
- Performance Appraisal Self AssessmentDocument3 pagesPerformance Appraisal Self AssessmentAniket AgrawalNo ratings yet
- Spreads Through The Major ArcanaDocument29 pagesSpreads Through The Major Arcanaaamir100% (1)
- Spreads Through The Major ArcanaDocument29 pagesSpreads Through The Major Arcanaaamir100% (1)
- Cardillio 1: General InformationDocument1 pageCardillio 1: General Informationmashke82No ratings yet
- The Dual Role of Bacteriocins As Anti - and ProbioticsDocument25 pagesThe Dual Role of Bacteriocins As Anti - and Probioticsmashke82No ratings yet
- Katarina BtinsDocument58 pagesKatarina Btinsmashke82No ratings yet
- Soluble Factors From Lactobacillus GG Activate MAPKs and InduceDocument15 pagesSoluble Factors From Lactobacillus GG Activate MAPKs and Inducemashke82No ratings yet
- Effects of Lactobacillus Bulgaricus After Radiation enDocument2 pagesEffects of Lactobacillus Bulgaricus After Radiation enmashke82No ratings yet
- MA7 5 Istrazivanja Obradovic I MedoBogdanovic OsM LDocument18 pagesMA7 5 Istrazivanja Obradovic I MedoBogdanovic OsM Lmashke82No ratings yet
- New Text DocumentDocument1 pageNew Text Documentmashke82No ratings yet
- Current Status and Emerging Role of GlutathioneDocument14 pagesCurrent Status and Emerging Role of Glutathionemashke82No ratings yet
- Removal of Aflatoxin B1 From Contaminated Liquid Media byDocument5 pagesRemoval of Aflatoxin B1 From Contaminated Liquid Media bymashke82No ratings yet
- Photoshop TechniquesDocument6 pagesPhotoshop Techniquesmashke82No ratings yet
- Herpes Zoster in Diverse Situations - A Review PDFDocument21 pagesHerpes Zoster in Diverse Situations - A Review PDFLaras KinasihNo ratings yet
- Viruses and Virology: Structure, Replication, and Diseases Like AIDSDocument57 pagesViruses and Virology: Structure, Replication, and Diseases Like AIDSSophan HadieNo ratings yet
- HERPESVIRIDAEDocument8 pagesHERPESVIRIDAEPauline MaryNo ratings yet
- DNA VirusesDocument154 pagesDNA VirusesRod Pasion0% (1)
- Basic Virology 3rd EditionDocument16 pagesBasic Virology 3rd EditionrouzbehnoroozyNo ratings yet
- 5.01 DNA VirusesDocument54 pages5.01 DNA VirusesPatricia Nicole Alcaraz100% (1)
- CVIR401 Lecture on HerpesvirusesDocument48 pagesCVIR401 Lecture on HerpesvirusesJeanPaule JoumaaNo ratings yet
- Viruses BasicsDocument53 pagesViruses Basicsmokashe1987No ratings yet
- Viral Structure and ReplicationDocument4 pagesViral Structure and Replicationcanela1527100% (1)
- SBI3U Unit 1Document5 pagesSBI3U Unit 1Sara SNo ratings yet
- J Oral Pathology Medicine - 2007 - Arduino - Herpes Simplex Virus Type 1 Infection Overview On RelevantDocument15 pagesJ Oral Pathology Medicine - 2007 - Arduino - Herpes Simplex Virus Type 1 Infection Overview On RelevantTestNo ratings yet
- Pathogenesis of Ruminant Herpesvirus Infections: Monika Engels, Mathias AckermannDocument13 pagesPathogenesis of Ruminant Herpesvirus Infections: Monika Engels, Mathias AckermannRosafina SetyantariNo ratings yet
- Epstein-Barr Virus: Biology and Clinical DiseaseDocument19 pagesEpstein-Barr Virus: Biology and Clinical Diseasealbabiega2No ratings yet
- Mauo 2018 Infeksi Ebv 2Document44 pagesMauo 2018 Infeksi Ebv 2OmeNo ratings yet
- Microbial DiversityDocument9 pagesMicrobial DiversityPresley Joy Graneta RamosNo ratings yet
- Report KoDocument6 pagesReport KobrucemarwinNo ratings yet
- Viruses, Viroids, and PrionsDocument65 pagesViruses, Viroids, and PrionsIvenks EeNo ratings yet
- 15 Virusne Infekcije U Trudnoci - PrevedenoDocument7 pages15 Virusne Infekcije U Trudnoci - PrevedenoVelibor StankovićNo ratings yet
- Virology Learning TableDocument6 pagesVirology Learning Table//No ratings yet
- 2010 Hiv Aids GrantsDocument216 pages2010 Hiv Aids GrantsSherry HeinzNo ratings yet
- Herpes Zoster Diagnostic Therapeutic and Preventive ApproachesDocument15 pagesHerpes Zoster Diagnostic Therapeutic and Preventive ApproacheswulanNo ratings yet
- VirologyDocument7 pagesVirologyKyle EoineNo ratings yet
- MicrobiologyDocument20 pagesMicrobiologySarah JaneNo ratings yet
- Infectious Diseases General 21Document151 pagesInfectious Diseases General 21Esma GündoğduNo ratings yet
- Disease Process HIVDocument4 pagesDisease Process HIValeksdj1987No ratings yet
- Replication of VirusesDocument6 pagesReplication of VirusesAhmad DamatiNo ratings yet
- HIBERNACIONDocument29 pagesHIBERNACIONMariana MuñozNo ratings yet
- 2014-2018 Past Exam Qs + Example Qs For MICR3001Document52 pages2014-2018 Past Exam Qs + Example Qs For MICR3001ekampreetNo ratings yet
- BASIC VIROLOGY, Third Edition by Wagner, Hewlett, Bloom and CameriniDocument25 pagesBASIC VIROLOGY, Third Edition by Wagner, Hewlett, Bloom and CameriniJason PhalangeNo ratings yet