You might also like
- Autolog Medtronic User ManualDocument34 pagesAutolog Medtronic User Manual111No ratings yet
- Microbiologist: 3.1.5 Isolation & Gram StainingDocument5 pagesMicrobiologist: 3.1.5 Isolation & Gram Stainingapi-534896073No ratings yet
- Comprehensive Geriatric Assessment Proforma Apr-15Document11 pagesComprehensive Geriatric Assessment Proforma Apr-15Udin Nicotinic100% (2)
- cl-DUTIES AND RESPONSIBILITIES OF LAB PERSONNELSDocument2 pagescl-DUTIES AND RESPONSIBILITIES OF LAB PERSONNELSRazel Ann Elagio100% (2)
- Martial Arts - Emei Qi Gong-ExercisesDocument3 pagesMartial Arts - Emei Qi Gong-ExercisesSolomon Cosmin Ionut100% (3)
- Pre & POst Operative ChecklistDocument2 pagesPre & POst Operative Checklistmangesh virkar75% (4)
- Swiss Airlines Medical FormDocument3 pagesSwiss Airlines Medical FormVidu ChaNo ratings yet
- Medif FormDocument4 pagesMedif FormVin RNo ratings yet
- Application For Carriage of Medical Passengers: Passenger'S DetailDocument3 pagesApplication For Carriage of Medical Passengers: Passenger'S DetailnitinNo ratings yet
- Attachment A of Medical RequirementDocument8 pagesAttachment A of Medical Requirementyoutuber AbheeNo ratings yet
- Case Sheet L3Document22 pagesCase Sheet L3Gulfeshan ArshiNo ratings yet
- Cashless Authorisation Requisition FormDocument1 pageCashless Authorisation Requisition FormPandurangaNo ratings yet
- Statement of Medical Examiner - Total Permanent Disability Section BDocument4 pagesStatement of Medical Examiner - Total Permanent Disability Section Brajecon543No ratings yet
- Attending Physician's Statement For Proposed Insured/OwnerDocument2 pagesAttending Physician's Statement For Proposed Insured/OwnerSincerely ReynNo ratings yet
- Form 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedDocument2 pagesForm 1: Cashless Request Form Iffco Tokio General Insurance Company LimitedRaju.PalNo ratings yet
- Medical Information Form: Medif NoDocument6 pagesMedical Information Form: Medif NoAnonymous yQKd2nv100% (1)
- CERTIFICATE OF HEALTH (To Be Filled Out by A Physician) - Page 1Document2 pagesCERTIFICATE OF HEALTH (To Be Filled Out by A Physician) - Page 1gnzbdbNo ratings yet
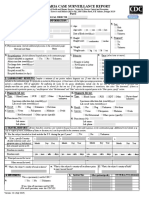
- Local Record Id: H. Local Subject Id:: Specimen Type CDC ID (From 50.34 Submission) Other Specimen (Specify)Document5 pagesLocal Record Id: H. Local Subject Id:: Specimen Type CDC ID (From 50.34 Submission) Other Specimen (Specify)Ashwin babuNo ratings yet
- Prerecruitment Medical Fitness Certificate FormDocument5 pagesPrerecruitment Medical Fitness Certificate FormAkella LokeshNo ratings yet
- Medif Information Sheet For Passengers Requiring Medical Clearence - Part 1-2 - Tarom From 4122 - 2Document2 pagesMedif Information Sheet For Passengers Requiring Medical Clearence - Part 1-2 - Tarom From 4122 - 2ViolleteMorenaNo ratings yet
- Request For Patient Transport V2020 - 1.5Document2 pagesRequest For Patient Transport V2020 - 1.5farm hostNo ratings yet
- Transfer Document Check List Hospital Handover To Another FacilityDocument3 pagesTransfer Document Check List Hospital Handover To Another Facilitydwirabiatul adwiyahaliNo ratings yet
- ISU Ogrenci Klinik Uygulama Bakim Plani Degerlendirme DönüştürüldüDocument23 pagesISU Ogrenci Klinik Uygulama Bakim Plani Degerlendirme DönüştürüldüMerve kdkkNo ratings yet
- MEDIFenglish Final 2021Document4 pagesMEDIFenglish Final 2021infoNo ratings yet
- Health Declaration Form - AMSB PDFDocument4 pagesHealth Declaration Form - AMSB PDFKhairul RazaliNo ratings yet
- FME Form Complainant FSSC July 2021Document4 pagesFME Form Complainant FSSC July 2021Mohaaz AbdiNo ratings yet
- Reimbursement Medical Form NewDocument2 pagesReimbursement Medical Form NewAtiko Atochi100% (1)
- Emt Physical FormDocument1 pageEmt Physical FormLeeann LopezNo ratings yet
- Rumah Sakit Katolik Widya Mandala Surabaya Form Transfer PasienDocument3 pagesRumah Sakit Katolik Widya Mandala Surabaya Form Transfer PasienULFA NADIYANo ratings yet
- Cigna TTK-preauthDocument2 pagesCigna TTK-preauthBOOKREADER_NOWNo ratings yet
- Önemli ECLS Registry FormDocument9 pagesÖnemli ECLS Registry Formyowewe7363No ratings yet
- HDFC ERGO Preauth FormDocument2 pagesHDFC ERGO Preauth FormM/s MicrotechNo ratings yet
- Hydrotherapy Referral Form and Risk Assessment Template For SystmOneDocument3 pagesHydrotherapy Referral Form and Risk Assessment Template For SystmOnetajwer amjadNo ratings yet
- AORN Comprehensive Surgical Checklist 2016Document1 pageAORN Comprehensive Surgical Checklist 2016Firma WahyuNo ratings yet
- Medical Report FormDocument2 pagesMedical Report FormAdo StoreNo ratings yet
- Medif Form 080216njDocument3 pagesMedif Form 080216njDenver SimNo ratings yet
- Enous Hromboembolism Report Form:: HospitalDocument4 pagesEnous Hromboembolism Report Form:: HospitalHosam GomaaNo ratings yet
- Universal Sompo Cashless Request FormDocument2 pagesUniversal Sompo Cashless Request FormM/s MicrotechNo ratings yet
- Hospital Seal (Must Contain Hospital ID) : Patient / Insured Name & SignatureDocument6 pagesHospital Seal (Must Contain Hospital ID) : Patient / Insured Name & SignaturePrince GargNo ratings yet
- MEDIFDocument6 pagesMEDIFNikola TorbicaNo ratings yet
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormPaul Angelo E. Caliva0% (1)
- Medical Report FormDocument2 pagesMedical Report FormPaolo AndoNo ratings yet
- Raksha New Pre-Authorization FormDocument1 pageRaksha New Pre-Authorization Formjigerpanchal0% (1)
- Inter Global Claim Form 2010Document4 pagesInter Global Claim Form 2010ywa00No ratings yet
- Formulir TransferDocument1 pageFormulir TransferPutri BalqisNo ratings yet
- Cashless Claim FormDocument1 pageCashless Claim FormhariharanccetNo ratings yet
- Nursing School Care Plan TemplateDocument17 pagesNursing School Care Plan TemplateChiamakaNo ratings yet
- NUR 263 Daily Assessment Worksheet Rubric 2024Document12 pagesNUR 263 Daily Assessment Worksheet Rubric 2024vercia8877No ratings yet
- Physical Fitness - Certificate 2022Document2 pagesPhysical Fitness - Certificate 2022Warrior SoulNo ratings yet
- VBA-21-0960J-2-ARE Male Reproductive PDFDocument6 pagesVBA-21-0960J-2-ARE Male Reproductive PDFCombat CraigNo ratings yet
- Liver Disease Questionnaire For Proposed Insured/OwnerDocument2 pagesLiver Disease Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- TRF For COVID-19 TEST (Coronavirus) : History Yes NoDocument1 pageTRF For COVID-19 TEST (Coronavirus) : History Yes NoRajendra ChavanNo ratings yet
- TDM Request FormDocument3 pagesTDM Request FormMuhammad IqbalNo ratings yet
- TDM Request FormDocument3 pagesTDM Request FormWildan Setyo RayandiNo ratings yet
- DRR-04 Ambulance Patient Care ReportDocument2 pagesDRR-04 Ambulance Patient Care ReportJulie AnnNo ratings yet
- Preprocedure Check-In Sign-In Time-Out Sign-Out: Teal Joint Commission and WHODocument2 pagesPreprocedure Check-In Sign-In Time-Out Sign-Out: Teal Joint Commission and WHOYL LYNo ratings yet
- Cashless FormDocument2 pagesCashless FormHitendra PatelNo ratings yet
- CIF DiphDocument2 pagesCIF DiphIvy marie BonNo ratings yet
- Teachers Health Examination Card CS Form 86Document1 pageTeachers Health Examination Card CS Form 86Sherchen Antonio-CortesNo ratings yet
- HakaDocument7 pagesHakaGudang Training K3No ratings yet
- FDARDocument2 pagesFDARChristian AzulNo ratings yet
- Patient's Name & Surname:: Questions Related To A Medical Condition of Our ClientDocument1 pagePatient's Name & Surname:: Questions Related To A Medical Condition of Our ClientAlex CusminNo ratings yet
- Unitedhealthcare Parekh Tpa Pvt. LTDDocument2 pagesUnitedhealthcare Parekh Tpa Pvt. LTDSameer MandgeNo ratings yet
- Diagnostic Features of Disease: Based on French's Index of Differential DiagnosisFrom EverandDiagnostic Features of Disease: Based on French's Index of Differential DiagnosisRating: 1 out of 5 stars1/5 (1)
- Physical AssesmentDocument5 pagesPhysical AssesmentLina LagaNo ratings yet
- Soal Kelas 8 Kompetensi 3Document5 pagesSoal Kelas 8 Kompetensi 3Lina LagaNo ratings yet
- Soal Kelas 8 Kompetensi 2-WPS OfficeDocument5 pagesSoal Kelas 8 Kompetensi 2-WPS OfficeLina LagaNo ratings yet
- SOAL KELAS 8-WPS OfficeDocument6 pagesSOAL KELAS 8-WPS OfficeLina LagaNo ratings yet
- Depression FactsDocument5 pagesDepression FactsStargazerNo ratings yet
- MSU-Iligan Institute of Technology: Nursing Health Assessment IDocument2 pagesMSU-Iligan Institute of Technology: Nursing Health Assessment IBianca Mikaela DosdosNo ratings yet
- PROBIÓTICOSDocument5 pagesPROBIÓTICOSstephanielopes2020No ratings yet
- Udder & TeatDocument23 pagesUdder & TeatAdarshBijapurNo ratings yet
- SpecialistDocument1 pageSpecialistShashiNo ratings yet
- Textbook of Neural Repair and Rehabilitation Medical Neurorehabilitation 2006Document802 pagesTextbook of Neural Repair and Rehabilitation Medical Neurorehabilitation 2006enigelNo ratings yet
- Temporomandibular Joint Syndrome PDFDocument4 pagesTemporomandibular Joint Syndrome PDFMaxim BzoviiNo ratings yet
- Evidence Based Dietetics PracticeDocument11 pagesEvidence Based Dietetics PracticeLinaTrisnawatiNo ratings yet
- Reporte 2020 de La Oficina de Asuntos Globales de Estados UnidosDocument72 pagesReporte 2020 de La Oficina de Asuntos Globales de Estados UnidosAristegui NoticiasNo ratings yet
- Gotthard Bulau Closed Water-Seal Drainage For Empyema,: John A. MeyerDocument3 pagesGotthard Bulau Closed Water-Seal Drainage For Empyema,: John A. Meyerputri aprilianiNo ratings yet
- Escalas de EfronDocument2 pagesEscalas de Efronkarina100% (1)
- Handout and Questions of HysterosalpingDocument12 pagesHandout and Questions of Hysterosalpingahmad shaltout100% (2)
- Diagnostic Tests PDFDocument2 pagesDiagnostic Tests PDFBenedict AlvarezNo ratings yet
- Review and Correction of The Previous Minutes of The MeetingDocument3 pagesReview and Correction of The Previous Minutes of The MeetingDani CawaiNo ratings yet
- Celutrat FM EngDocument2 pagesCelutrat FM EngVíctor Digón TrabadoNo ratings yet
- AJOG Modelo Predictivo para Preeclampsia Nicolaides 2019Document13 pagesAJOG Modelo Predictivo para Preeclampsia Nicolaides 2019Ana PadillaNo ratings yet
- Anatomy of The Genitourinary TractDocument5 pagesAnatomy of The Genitourinary TractQonitaaNo ratings yet
- Uworld Skin DisordersDocument5 pagesUworld Skin DisordersJoan ChoiNo ratings yet
- Hospital ProfileDocument40 pagesHospital ProfileSeeSubsea50% (2)
- Adobe Scan 27-May-2021Document1 pageAdobe Scan 27-May-2021Raja SekharNo ratings yet
- Electronic Edge ExampleDocument138 pagesElectronic Edge Examplezarrin77No ratings yet
- Beg Talk To Doctor - Unit 1Document66 pagesBeg Talk To Doctor - Unit 1Eliza Cristea OneciNo ratings yet
- Etiologi Krisis Tiroid Dan Koma MiksedemaDocument4 pagesEtiologi Krisis Tiroid Dan Koma MiksedemaRaafi Puristya Aries DarmawanNo ratings yet
- Research Paper FinalDocument7 pagesResearch Paper Finalapi-643588876No ratings yet
- Hiatus Hernia - Chinese Herbs, Chinese Medicine, AcupunctureDocument6 pagesHiatus Hernia - Chinese Herbs, Chinese Medicine, AcupunctureCarlCordNo ratings yet
- Hypo Thyroid Is MDocument2 pagesHypo Thyroid Is MRaisah Bint AbdullahNo ratings yet