You might also like
- The Basics: A Comprehensive Outline of Nursing School ContentFrom EverandThe Basics: A Comprehensive Outline of Nursing School ContentRating: 5 out of 5 stars5/5 (3)
- STUDENT-Sickle - Cell-FUNDAMENTAL ReasoningDocument7 pagesSTUDENT-Sickle - Cell-FUNDAMENTAL ReasoningSharon Tanveer0% (1)
- Subjective Assessment FormDocument8 pagesSubjective Assessment FormTriana KarnadipaNo ratings yet
- Note Book For History Taking and Patient RecordDocument11 pagesNote Book For History Taking and Patient RecordSayed Muhammad Yousuf0% (1)
- EMT B Study Guid2Document11 pagesEMT B Study Guid2varela86100% (1)
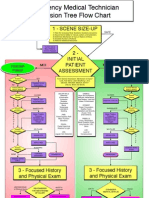
- Emt PosterDocument1 pageEmt PosterDrThant Zin Tun50% (2)
- Pre Lab Work Health AssessmentDocument11 pagesPre Lab Work Health AssessmentSarah Jane VasquezNo ratings yet
- This Study Resource Was: Assessment & Reasoning Cardiac SystemDocument6 pagesThis Study Resource Was: Assessment & Reasoning Cardiac SystemSharon TanveerNo ratings yet
- IM Platinum 3rd-EdDocument357 pagesIM Platinum 3rd-EdJust Some Files100% (2)
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Magic of The Minimum Dose PDFDocument221 pagesMagic of The Minimum Dose PDFminunat100% (1)
- Head-To-Toe Checklist: Beautiful Nursing LLCDocument4 pagesHead-To-Toe Checklist: Beautiful Nursing LLCcarlyNo ratings yet
- Head To ToeDocument4 pagesHead To Toenazbeen.ahmadiNo ratings yet
- Nursing Assessment New 1Document10 pagesNursing Assessment New 1smithapsNo ratings yet
- Case Study 3 CVD Bleed HCVD Type 2 DM CICD Stage 5 WorksheetDocument27 pagesCase Study 3 CVD Bleed HCVD Type 2 DM CICD Stage 5 WorksheetJade HemmingsNo ratings yet
- Guide To Clerking 2014Document24 pagesGuide To Clerking 2014Ridhwan Amid100% (1)
- Careplan II Fundamentals III FinalDocument28 pagesCareplan II Fundamentals III FinalRebecca RathburnNo ratings yet
- Medicine HandbookDocument43 pagesMedicine Handbookramavisalam100% (2)
- MedSurg SBARDocument2 pagesMedSurg SBARduaalipa18No ratings yet
- Cardio Pulmonary AssessmentDocument8 pagesCardio Pulmonary AssessmentSHAIK SHABEENANo ratings yet
- General Assessment TemplateDocument8 pagesGeneral Assessment TemplateBob HopeNo ratings yet
- CVS Case ProformaDocument2 pagesCVS Case ProformaRiyaSingh100% (1)
- Nurse Report Sheet OriginalDocument2 pagesNurse Report Sheet Originalhvera01No ratings yet
- Wallace State Community College NURSING DATABASE: Nursing HomeDocument9 pagesWallace State Community College NURSING DATABASE: Nursing HomeEnger NushunNo ratings yet
- AME-New Proforma-1Document4 pagesAME-New Proforma-1KRISHNA MOHAN PANDEY0% (1)
- RevisedDocument16 pagesRevisedZymer Lee AbasoloNo ratings yet
- 2014 06 21 KAB PT Assessment Form - GENERAL PDFDocument12 pages2014 06 21 KAB PT Assessment Form - GENERAL PDFDaniel raja SotardodoNo ratings yet
- NTILS GuideDocument11 pagesNTILS GuideNeil ThomasNo ratings yet
- Case ClosedDocument10 pagesCase ClosedIvel Kram DunoNo ratings yet
- 2 EsiDocument23 pages2 EsizianaNo ratings yet
- HistoryandPhysicalExamDocument105 pagesHistoryandPhysicalExamsilentscream0618No ratings yet
- PPPPPDocument5 pagesPPPPPksheckelNo ratings yet
- ASSESSMENT FORM: Spring 2006 Client's Number: InstructionsDocument6 pagesASSESSMENT FORM: Spring 2006 Client's Number: Instructionsdenisemw88No ratings yet
- I. Vital Information: W La Paz, Iloilo CityDocument7 pagesI. Vital Information: W La Paz, Iloilo CityelleNo ratings yet
- Charting GuidelinesDocument4 pagesCharting Guidelinesgrad_nurse_2015No ratings yet
- History Taking FormatDocument10 pagesHistory Taking FormatMuskaan DeepNo ratings yet
- Nursing Care Plan Patient's Name: Age: Sex: Address:: Nursing-Notes/communicable - Diseases - Notes/amoebiasisDocument4 pagesNursing Care Plan Patient's Name: Age: Sex: Address:: Nursing-Notes/communicable - Diseases - Notes/amoebiasisGILIANNE MARIE JIMENEANo ratings yet
- Diana Pefbrianti, S.Kep., NS., M.KepDocument33 pagesDiana Pefbrianti, S.Kep., NS., M.KepMursidah faNo ratings yet
- Medical Record & SheetDocument9 pagesMedical Record & SheetTawfek RedaNo ratings yet
- Weekly Patient Care Worksheet0Document4 pagesWeekly Patient Care Worksheet0mitchelltaiwo007No ratings yet
- Nursing Process - AdultDocument7 pagesNursing Process - Adultjoannamae molagaNo ratings yet
- 1-General ExaminationDocument5 pages1-General Examinationalmatrim10No ratings yet
- 11 Pediatric Anesthesia Pre-Evaluation Form (New!!!)Document4 pages11 Pediatric Anesthesia Pre-Evaluation Form (New!!!)Aina HaravataNo ratings yet
- Cme: Dengue Fever: by Nur ShafikaDocument47 pagesCme: Dengue Fever: by Nur ShafikaSyuk IdhamNo ratings yet
- Anglais Médical1Document23 pagesAnglais Médical1Nettah MarouaNo ratings yet
- Diagnostic Features of Disease: Based on French's Index of Differential DiagnosisFrom EverandDiagnostic Features of Disease: Based on French's Index of Differential DiagnosisRating: 1 out of 5 stars1/5 (1)
- Chronic Disease Management for Small AnimalsFrom EverandChronic Disease Management for Small AnimalsW. Dunbar GramNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Superior Vena Cava Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSuperior Vena Cava Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A Gene Primer for Health Care Providers: The Genomics of Cirs and Associated Molecular PathwaysFrom EverandA Gene Primer for Health Care Providers: The Genomics of Cirs and Associated Molecular PathwaysNo ratings yet
- 9 Steps To Reverse DementiaDocument36 pages9 Steps To Reverse DementiaLavinia PirlogNo ratings yet
- home-delhimed-downloadfile-IMA NATCON SCIENTIFIC PROGRAME PDFDocument15 pageshome-delhimed-downloadfile-IMA NATCON SCIENTIFIC PROGRAME PDFRaveenaNo ratings yet
- Card Medical HistoryDocument4 pagesCard Medical HistoryDanonino12No ratings yet
- ReferensiDocument2 pagesReferensiYuanita RosalinaNo ratings yet
- Labiomandibular Paresthesia Caused by Endodontic Treatment - An Anatomic and Clinical Study PDFDocument13 pagesLabiomandibular Paresthesia Caused by Endodontic Treatment - An Anatomic and Clinical Study PDFAlexandra DumitracheNo ratings yet
- Food Crisis in The World !Document6 pagesFood Crisis in The World !ChrissBright E. HermanNo ratings yet
- Reconocimiento Del Acv CLINISC 2012Document21 pagesReconocimiento Del Acv CLINISC 2012Camilo GomezNo ratings yet
- Molecular Biology of BacteriaDocument57 pagesMolecular Biology of BacteriaSean ArifinNo ratings yet
- P.E 3A Learning Activity Sheet WEEK 5 6Document7 pagesP.E 3A Learning Activity Sheet WEEK 5 6Ris CorreaNo ratings yet
- Bilirubin Metabolism Jaundice PPP 9Document27 pagesBilirubin Metabolism Jaundice PPP 9Regina Marsha Xaveria100% (1)
- Assessment, Northwick ParkDocument2 pagesAssessment, Northwick ParkMelian Anita100% (1)
- Formative Gen EdDocument119 pagesFormative Gen EdDan GertezNo ratings yet
- Difficult Airway AlgorithmDocument48 pagesDifficult Airway AlgorithmshikhaNo ratings yet
- Analytical Exposition TextDocument30 pagesAnalytical Exposition TextdenisakusumawardhaniNo ratings yet
- Case Studies - EditedDocument5 pagesCase Studies - EditedFunny LifeNo ratings yet
- Cardiovascular Risk Factors in Airline PilotsDocument4 pagesCardiovascular Risk Factors in Airline Pilotsluis11256No ratings yet
- Detect Pharmaceutical Health Hazards and ActDocument81 pagesDetect Pharmaceutical Health Hazards and Acttemesgen dinsaNo ratings yet
- NewFood 2015 Nr004Document88 pagesNewFood 2015 Nr004XavierNo ratings yet
- Foot and Ankle Injuries Kylee Phillips - 0Document74 pagesFoot and Ankle Injuries Kylee Phillips - 0rizwan.mughal1997No ratings yet
- Excel Dentistry 3rd Year Sample 2022Document25 pagesExcel Dentistry 3rd Year Sample 2022Mohammed hisham khanNo ratings yet
- Material Safety Data Sheet: 80W-90 Gear LubeDocument4 pagesMaterial Safety Data Sheet: 80W-90 Gear LubeFrank RodriguezNo ratings yet
- DNS ENT Case Write UpDocument8 pagesDNS ENT Case Write UpShafiq ZahariNo ratings yet
- Dry Needling Doc. Jan 18,13Document1 pageDry Needling Doc. Jan 18,13Rebecca SchirberNo ratings yet
- Notice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsDocument1 pageNotice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsJustia.comNo ratings yet
- Contraindications Herbal Remedies 2018Document8 pagesContraindications Herbal Remedies 2018skylarkmdNo ratings yet
- Common Mistakes-BiologyDocument8 pagesCommon Mistakes-BiologyteahockNo ratings yet
- Community Radio Script - Why We Have COVID Vaccines NowDocument2 pagesCommunity Radio Script - Why We Have COVID Vaccines NowBenBuilds PHNo ratings yet
- Lung Cancer Prediction Using Data Mining TechniquesDocument6 pagesLung Cancer Prediction Using Data Mining TechniquesKEZZIA MAE ABELLANo ratings yet
- Community Theatre and AIDS Studies in International Performance PDFDocument194 pagesCommunity Theatre and AIDS Studies in International Performance PDFgabriella feliciaNo ratings yet