You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Amazing Liver and Gallbladder Flush by Andreas MoritzDocument16 pagesThe Amazing Liver and Gallbladder Flush by Andreas MoritzTruth100% (6)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Justine Jackson Capstone AatDocument29 pagesJustine Jackson Capstone AatJuliana IshakNo ratings yet
- AMDLI COVID-19 Test ResultDocument2 pagesAMDLI COVID-19 Test ResultMarco Dela CruzNo ratings yet
- Blood Transfusion Reaction Vsim - Sept 16 22 NSGD 2106Document5 pagesBlood Transfusion Reaction Vsim - Sept 16 22 NSGD 2106api-631170779No ratings yet
- Emergency Response Planning For A Potent PDFDocument8 pagesEmergency Response Planning For A Potent PDFcphanNo ratings yet
- Distribution of Casualties in A Mass Cas-1 PDFDocument8 pagesDistribution of Casualties in A Mass Cas-1 PDFcphanNo ratings yet
- The First Boat People PDFDocument331 pagesThe First Boat People PDFcphanNo ratings yet
- Terrorism in Japan The Sarin Gas Attacks PDFDocument6 pagesTerrorism in Japan The Sarin Gas Attacks PDFcphanNo ratings yet
- Resilience 1 PDFDocument32 pagesResilience 1 PDFcphanNo ratings yet
- FSI Nuclear Terrorism The Threat of NuclDocument4 pagesFSI Nuclear Terrorism The Threat of NuclcphanNo ratings yet
- Thehomelandsecurity PDFDocument274 pagesThehomelandsecurity PDFcphanNo ratings yet
- Managingemerconseq PDFDocument116 pagesManagingemerconseq PDFcphanNo ratings yet
- Nuclear Terrorism and Maritime SecurityDocument264 pagesNuclear Terrorism and Maritime SecuritycphanNo ratings yet
- The Evolution of Counterterrorism Will T PDFDocument20 pagesThe Evolution of Counterterrorism Will T PDFcphanNo ratings yet
- Securing Global Maritime Supply ChainsDocument25 pagesSecuring Global Maritime Supply ChainscphanNo ratings yet
- The Sum of All Fears Israel S PerceptionDocument13 pagesThe Sum of All Fears Israel S PerceptioncphanNo ratings yet
- Cyber Terrorism A Clear and Present Danger The SumDocument17 pagesCyber Terrorism A Clear and Present Danger The SumcphanNo ratings yet
- Watching 9 11 in The Time of The Event PDFDocument14 pagesWatching 9 11 in The Time of The Event PDFcphanNo ratings yet
- U.S. Grand Strategy and Counterterrorism PDFDocument23 pagesU.S. Grand Strategy and Counterterrorism PDFcphanNo ratings yet
- Watching Chinese Indonesians Through The Lens of CameraDocument20 pagesWatching Chinese Indonesians Through The Lens of CameraAndrew LimNo ratings yet
- The Basics For Understanding Qassams Scu PDFDocument184 pagesThe Basics For Understanding Qassams Scu PDFcphanNo ratings yet
- Car Bomb Strikes Military Convoy in AnkaDocument3 pagesCar Bomb Strikes Military Convoy in AnkacphanNo ratings yet
- Covid 19 Virus Situation Report 2020309Document9 pagesCovid 19 Virus Situation Report 2020309cphanNo ratings yet
- Very Final Thesis Democracy and Terroris PDFDocument234 pagesVery Final Thesis Democracy and Terroris PDFcphanNo ratings yet
- Watching Chinese Indonesians Through The Lens of CameraDocument20 pagesWatching Chinese Indonesians Through The Lens of CameraAndrew LimNo ratings yet
- Securing America S Mass Transit SystemsDocument3 pagesSecuring America S Mass Transit SystemscphanNo ratings yet
- I Did My Bit' - Terrorism, Tarde and The Vehicle Ramming Attack As An Imitative Event PDFDocument23 pagesI Did My Bit' - Terrorism, Tarde and The Vehicle Ramming Attack As An Imitative Event PDFcphanNo ratings yet
- Master Technical Questions - SARS-CoV-2 - 04MAR20Document18 pagesMaster Technical Questions - SARS-CoV-2 - 04MAR20cphanNo ratings yet
- Taylor Transit Security PDFDocument11 pagesTaylor Transit Security PDFcphanNo ratings yet
- Vehicular Terrorism The Threat Behind The Wheel PDFDocument13 pagesVehicular Terrorism The Threat Behind The Wheel PDFcphanNo ratings yet
- I Did My Bit' - Terrorism, Tarde and The Vehicle Ramming Attack As An Imitative Event PDFDocument23 pagesI Did My Bit' - Terrorism, Tarde and The Vehicle Ramming Attack As An Imitative Event PDFcphanNo ratings yet
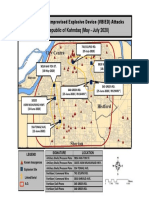
- Vehicle Borne Improvised Explosive Devic PDFDocument1 pageVehicle Borne Improvised Explosive Devic PDFcphanNo ratings yet
- Vehicular Terrorism The Threat Behind The Wheel PDFDocument13 pagesVehicular Terrorism The Threat Behind The Wheel PDFcphanNo ratings yet
- Appointment Letter Non Teaching StaffDocument7 pagesAppointment Letter Non Teaching StaffJolleah Belmonte AltezaNo ratings yet
- 4128i HSRN 192700105 04 000Document18 pages4128i HSRN 192700105 04 000Padma ShivanandaNo ratings yet
- ICD-10 Neoplasm Coding GuidelinesDocument59 pagesICD-10 Neoplasm Coding GuidelinesMuhammad Syamsul ArifinNo ratings yet
- Intellectual DiabilityDocument10 pagesIntellectual DiabilityAngelo PapimNo ratings yet
- Golden Notes for PSM_3rd Edition_Dr Parimal_2024Document9 pagesGolden Notes for PSM_3rd Edition_Dr Parimal_2024AnjuNo ratings yet
- The Radiation Boom - Case Studies - When Medical Radiation Goes Awry - NYTimesDocument4 pagesThe Radiation Boom - Case Studies - When Medical Radiation Goes Awry - NYTimesMuh Taufik Dwi PutraNo ratings yet
- Kenny's Anatomy and Pediatrics Review | March 2023Document254 pagesKenny's Anatomy and Pediatrics Review | March 2023Huguette Marie NseleNo ratings yet
- The Post-Market Priority: Understanding and Meeting Demand For Effective Post-Market Clinical Follow-UpDocument8 pagesThe Post-Market Priority: Understanding and Meeting Demand For Effective Post-Market Clinical Follow-UpbasakerpolatNo ratings yet
- De Torres Labor Law I ReportDocument11 pagesDe Torres Labor Law I ReportErole John AtienzaNo ratings yet
- International General Certificate Assessor's Marking Sheet (2011 Specification) Igc3 - The Health and Safety Practical ApplicationDocument11 pagesInternational General Certificate Assessor's Marking Sheet (2011 Specification) Igc3 - The Health and Safety Practical ApplicationVigneshwaraNo ratings yet
- Coping Methods and Counseling for Grief Across AgesDocument8 pagesCoping Methods and Counseling for Grief Across AgesDaciana DumitrescuNo ratings yet
- JobDocument5 pagesJobLalaluluNo ratings yet
- Air Force Body Composition Policy MemoDocument3 pagesAir Force Body Composition Policy MemoRichard PollinaNo ratings yet
- CORAD 101, Health and Welfare ProgramsDocument5 pagesCORAD 101, Health and Welfare ProgramsdaybudsvaldezNo ratings yet
- Measures of Health InequalitiesDocument16 pagesMeasures of Health InequalitiesMusonda LumbweNo ratings yet
- © 2016 The Guilford Press: Introduction To The ADHD Rating ScalesDocument6 pages© 2016 The Guilford Press: Introduction To The ADHD Rating ScalesJennifer Soares de Souza de FreitasNo ratings yet
- Unit 11 Other Hospital Information System PDFDocument18 pagesUnit 11 Other Hospital Information System PDFRobinJohnII100% (1)
- Standard Operating Procedure (SOP)Document2 pagesStandard Operating Procedure (SOP)Rudrajit KarguptaNo ratings yet
- The Architecture of Hospitals ConferenceDocument6 pagesThe Architecture of Hospitals ConferenceJavier SiñaniNo ratings yet
- REPORT - Crossroads of People - Place - ProsperityDocument57 pagesREPORT - Crossroads of People - Place - ProsperityVeny KimNo ratings yet
- 2 CGMPDocument78 pages2 CGMPRICHELLE JIELEN QUEBECNo ratings yet
- Social Security and Labor Welfare (MBA-961) : Q.1 What Is The Concept of Social Security?Document16 pagesSocial Security and Labor Welfare (MBA-961) : Q.1 What Is The Concept of Social Security?Nisha RineshNo ratings yet
- Effects of High Intensity Interval Training On Increasing Explosive Power, Speed, and AgilityDocument6 pagesEffects of High Intensity Interval Training On Increasing Explosive Power, Speed, and AgilityGytis GarbačiauskasNo ratings yet
- Obstetric HemorrhageDocument14 pagesObstetric Hemorrhageb3djo_76No ratings yet
- Media Bulletin 03 09 21 COVID 19Document17 pagesMedia Bulletin 03 09 21 COVID 19Ram KrishnanNo ratings yet
- Manifestations of Systemic Diseases and Conditions That Affect The Periodontal Attachment Apparatus: Case Definitions and Diagnostic ConsiderationsDocument22 pagesManifestations of Systemic Diseases and Conditions That Affect The Periodontal Attachment Apparatus: Case Definitions and Diagnostic ConsiderationsMarco Antonio García LunaNo ratings yet