You might also like
- Pemphigus Vulgaris Update October 2016 - Lay Reviewed August 2016Document6 pagesPemphigus Vulgaris Update October 2016 - Lay Reviewed August 2016EbetWasuwayNo ratings yet
- Group 2Document10 pagesGroup 2amponsahgrace0015No ratings yet
- Blistering DisordersDocument34 pagesBlistering DisordersSucdi CabdiNo ratings yet
- Pemphigus Vulgaris: BY:-Parth Chauhan (6) B1 Raj Gundaniya (11) B1Document9 pagesPemphigus Vulgaris: BY:-Parth Chauhan (6) B1 Raj Gundaniya (11) B1Shakti RathodNo ratings yet
- Diagnosis and Treatment of ImpetigoDocument9 pagesDiagnosis and Treatment of Impetigonisha_furiNo ratings yet
- Bullous Pemphigoid: PathogenesisDocument5 pagesBullous Pemphigoid: PathogenesisLukman GhozaliNo ratings yet
- Psoriasis: Posted: 02 Aug 2010 11:18 PM PDTDocument5 pagesPsoriasis: Posted: 02 Aug 2010 11:18 PM PDTScamb TrekNo ratings yet
- GFDFDFDocument7 pagesGFDFDFRm98No ratings yet
- PemphigusDocument15 pagesPemphigusMelly Narzabal100% (1)
- Epidemiology: Aureus and GABHS 10% of The Time. Methicillin-Resistant S Aureus (MRSA) HasDocument8 pagesEpidemiology: Aureus and GABHS 10% of The Time. Methicillin-Resistant S Aureus (MRSA) HasPutra YdpaNo ratings yet
- ImpetigoDocument7 pagesImpetigoBenjamin VanlaltlansangaNo ratings yet
- Herpes Simplex Update Nov 2014 - Lay Reviewed Nov 2014 (Revised May 2015)Document5 pagesHerpes Simplex Update Nov 2014 - Lay Reviewed Nov 2014 (Revised May 2015)Nur Ayu SulastriNo ratings yet
- Case Iv: 1. What Is Your Diagnosis? and Why? 2. How Would You Establish A Diagnosis in Such A Patient?Document5 pagesCase Iv: 1. What Is Your Diagnosis? and Why? 2. How Would You Establish A Diagnosis in Such A Patient?2806dhruvNo ratings yet
- Mycoplasma Is An Overlooked Lyme Co-Infection: Got A Question?Document26 pagesMycoplasma Is An Overlooked Lyme Co-Infection: Got A Question?Anamaria BaloghNo ratings yet
- Hypersensitivity RxnsDocument41 pagesHypersensitivity RxnsAsressieNo ratings yet
- TYPES Khushi PatelDocument17 pagesTYPES Khushi PatelMeet PatelNo ratings yet
- Presentation 1Document14 pagesPresentation 1TCB makerNo ratings yet
- Common DiseasesDocument7 pagesCommon DiseasesAlter BadonNo ratings yet
- Erythema MultiformeDocument5 pagesErythema MultiformeNicco MarantsonNo ratings yet
- Herpes Simplex Oral: EpidemiologyDocument5 pagesHerpes Simplex Oral: EpidemiologyFariz RamadhanNo ratings yet
- MonkeypoxDocument5 pagesMonkeypoxrizaNo ratings yet
- Viral Skin InfectionsDocument9 pagesViral Skin InfectionsMa Sul JudayaNo ratings yet
- Antimonium Crudum in Pediatric Skin ConditionsDocument9 pagesAntimonium Crudum in Pediatric Skin ConditionsJohn LangeNo ratings yet
- Wound ManagementDocument33 pagesWound ManagementDeSi BiLLaNo ratings yet
- Mayores. Chicken Pox - Concept MapDocument3 pagesMayores. Chicken Pox - Concept MapAlvic Dy KowNo ratings yet
- Bullous PemphigoidDocument13 pagesBullous PemphigoidSharifah HanimNo ratings yet
- PBL 3 CNSDocument13 pagesPBL 3 CNSAbdullah SohailNo ratings yet
- What Is HistoplasmosisDocument7 pagesWhat Is HistoplasmosisLessaNo ratings yet
- Genitourinary SystemDocument7 pagesGenitourinary SystemMary Angel VelascoNo ratings yet
- Microbial ResearchDocument12 pagesMicrobial Researchharshit kumarNo ratings yet
- Stom ProfileDocument71 pagesStom ProfileStefan CretuNo ratings yet
- W9 Measles German Measles Influenza Chicken Pox Covid19Document16 pagesW9 Measles German Measles Influenza Chicken Pox Covid19Jamie De LunaNo ratings yet
- Presentation 21Document15 pagesPresentation 21RAVEEN malikNo ratings yet
- Mycoplasma Pneumonia DiscussionDocument18 pagesMycoplasma Pneumonia Discussionmuskaanmir108No ratings yet
- Signs and SymptomsDocument6 pagesSigns and SymptomsKajim SharibiNo ratings yet
- Ulcerations of The Oral Cavity Infection Causing Oral UlcerationDocument17 pagesUlcerations of The Oral Cavity Infection Causing Oral UlcerationSebastian QuinteroNo ratings yet
- Tinea Cruris Imp Points With ReferencesDocument35 pagesTinea Cruris Imp Points With ReferencesSyed Saqib AliNo ratings yet
- Viral InfectionsDocument34 pagesViral InfectionsAlaa MadmoujNo ratings yet
- Herpes - RomeroDocument9 pagesHerpes - RomeroJanine Mae MacaraigNo ratings yet
- Mumps Clinical Diagnosis Fact Sheet 508Document2 pagesMumps Clinical Diagnosis Fact Sheet 508Andrea DelgadoNo ratings yet
- Communicable Disease Lectures 2Document2 pagesCommunicable Disease Lectures 2Sheana TmplNo ratings yet
- Chicken-Pox Concept MapDocument4 pagesChicken-Pox Concept MapElle0% (1)
- ProQuestDocuments 2014-03-22 2Document7 pagesProQuestDocuments 2014-03-22 2Aji DwijayantoNo ratings yet
- Patho Unit 5Document37 pagesPatho Unit 5Shafiya ShaikNo ratings yet
- Toxic Epidermal Necrolysis: AetiologyDocument5 pagesToxic Epidermal Necrolysis: AetiologyreyhanrrNo ratings yet
- ImmunoBullous DisordersDocument18 pagesImmunoBullous DisordersNali peterNo ratings yet
- Abscess Case Pre FinalDocument41 pagesAbscess Case Pre FinalDavid DueñasNo ratings yet
- Medical Terms Kind of IlnessDocument11 pagesMedical Terms Kind of IlnessFani KimerliNo ratings yet
- Psoriasis A Case StudyDocument14 pagesPsoriasis A Case StudyYayin PestañoNo ratings yet
- Pemphigus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPemphigus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Https://ar - scribd.com/document/391648283/OET Future Land Full Book Final Edition July 2018Document52 pagesHttps://ar - scribd.com/document/391648283/OET Future Land Full Book Final Edition July 2018Qutaiba ShdaifatNo ratings yet
- InfectiousDocument4 pagesInfectiouszainabd1964No ratings yet
- Infection & Specific Wound InfectionsDocument39 pagesInfection & Specific Wound InfectionsAhmed ShorshNo ratings yet
- 留学生讲义2018 11 2Document8 pages留学生讲义2018 11 2Nidya PutriNo ratings yet
- Bullous PemphigoidDocument15 pagesBullous PemphigoidYOSEF DERDESAWENo ratings yet
- PemphigusDocument8 pagesPemphiguszuqiri ChanelNo ratings yet
- Mumps NoteDocument4 pagesMumps Noteemmanuelnwa943No ratings yet
- Behcet Disease AND Toxoplasmosis: by DR Shahzada Khan Tmo Eye A Ward HMCDocument67 pagesBehcet Disease AND Toxoplasmosis: by DR Shahzada Khan Tmo Eye A Ward HMCShahzada KhanNo ratings yet
- Anatomy of The Vertebral Column: Supervisor: DR - Younis ZandyDocument36 pagesAnatomy of The Vertebral Column: Supervisor: DR - Younis ZandyZA IDNo ratings yet
- Parkinson's DiseaseDocument11 pagesParkinson's DiseaseZA IDNo ratings yet
- Frequency: Frequency Is A Cycles/sec (CPS) : The Number of Cycles Completed Each SecondDocument8 pagesFrequency: Frequency Is A Cycles/sec (CPS) : The Number of Cycles Completed Each SecondZA IDNo ratings yet
- Electro Acupuncture TherapyDocument16 pagesElectro Acupuncture TherapyZA IDNo ratings yet
- Lecture 2 Fundamental of NursingDocument6 pagesLecture 2 Fundamental of NursingZA IDNo ratings yet
- Introduction - Electrothe 1Document21 pagesIntroduction - Electrothe 1ZA IDNo ratings yet
- Faradic Current: Masood Abdullah Hussein MSC PhysiotherapyDocument30 pagesFaradic Current: Masood Abdullah Hussein MSC PhysiotherapyZA IDNo ratings yet
- Physical Therapy Patient Assessment FormDocument7 pagesPhysical Therapy Patient Assessment FormZA IDNo ratings yet
- Lect 2 - 3rd StageDocument9 pagesLect 2 - 3rd StageZA IDNo ratings yet
- Dynamic Flexibility TrainingDocument12 pagesDynamic Flexibility TrainingZA IDNo ratings yet
- Report About HypertensionDocument11 pagesReport About HypertensionZA IDNo ratings yet
- Lecture 4.anatomyppsDocument14 pagesLecture 4.anatomyppsZA IDNo ratings yet
- Skeletal System: Structure & Function of JointsDocument15 pagesSkeletal System: Structure & Function of JointsZA IDNo ratings yet
- Lecture 3 AnatomyDocument14 pagesLecture 3 AnatomyZA IDNo ratings yet
- Cell InjuryDocument15 pagesCell InjuryZA IDNo ratings yet
- Parrafin Wax ApplicationDocument20 pagesParrafin Wax ApplicationZA IDNo ratings yet
- Diathermy: Diathermy Is A Greek Word Meaning Through HeatingDocument8 pagesDiathermy: Diathermy Is A Greek Word Meaning Through HeatingZA IDNo ratings yet
- Minerals: Role of Minerals in The BodyDocument12 pagesMinerals: Role of Minerals in The BodyZA IDNo ratings yet
- Ultrasound Therapy The Nature of Acoustic EnergyDocument7 pagesUltrasound Therapy The Nature of Acoustic EnergyZA IDNo ratings yet
- How To Achive Your GoalDocument18 pagesHow To Achive Your GoalZA IDNo ratings yet
- The Muscles in The Anterior Compartment: Knee JointDocument9 pagesThe Muscles in The Anterior Compartment: Knee JointZA IDNo ratings yet
- Joint of Lower LimbDocument16 pagesJoint of Lower LimbZA ID100% (1)
- Computer SoftwareDocument9 pagesComputer SoftwareZA IDNo ratings yet
- Urinary Tract InfectionDocument10 pagesUrinary Tract InfectionMira Mariana UlfahNo ratings yet
- 6 DR NarsimuluDocument67 pages6 DR Narsimulushirish gundalaNo ratings yet
- Kaposi SarcomaDocument41 pagesKaposi SarcomaMihaela Pal0% (1)
- Immunostimulatory Effect of The Aqueous Leaf Extract of Responses of Oreochromis Mossambicus PetersDocument3 pagesImmunostimulatory Effect of The Aqueous Leaf Extract of Responses of Oreochromis Mossambicus PetersDavid ThangaduraiNo ratings yet
- Onikomikosis JournalDocument16 pagesOnikomikosis Journalwidya melianitaNo ratings yet
- IMMUNOPROPHYLAXISDocument30 pagesIMMUNOPROPHYLAXISAli TARARNo ratings yet
- Rajiv Gandhi University: of Health SciencesDocument40 pagesRajiv Gandhi University: of Health SciencesAnirudhGopalNo ratings yet
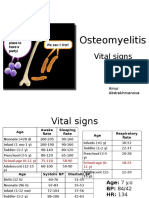
- PBL 2 - OsteomyelitisDocument10 pagesPBL 2 - OsteomyelitisAinur AbdrakhmanovaNo ratings yet
- National Immunization Program: Manual of Procedures Booklet 4Document32 pagesNational Immunization Program: Manual of Procedures Booklet 4Blue Pielago100% (1)
- Cream: For Eczema and Skin IrritationDocument2 pagesCream: For Eczema and Skin IrritationseluarbolaNo ratings yet
- 282585293Document208 pages282585293hebaNo ratings yet
- Control Strategies of Infectious BronchitisDocument4 pagesControl Strategies of Infectious Bronchitisfurqan915No ratings yet
- What Is HIV?Document6 pagesWhat Is HIV?JOSHUA PALMANo ratings yet
- HIV - AIDS Quiz - Health Encyclopedia - University of Rochester Medical CenterDocument1 pageHIV - AIDS Quiz - Health Encyclopedia - University of Rochester Medical CenterWz bel DfNo ratings yet
- Hepatits: Nitha K 2nd Year MSC NursingDocument88 pagesHepatits: Nitha K 2nd Year MSC NursingNITHA KNo ratings yet
- Lymphoma: An Overview: DR Louise Connell 05/03/2103Document66 pagesLymphoma: An Overview: DR Louise Connell 05/03/2103Dodo Saputera Damian100% (1)
- ACOG Practice Bulletin No 82 Management Of.50Document10 pagesACOG Practice Bulletin No 82 Management Of.50Ccorita GuerraNo ratings yet
- T Cell Development Thymic Education of T CellDocument34 pagesT Cell Development Thymic Education of T Cellapi-273068056No ratings yet
- Virulence Factors of Streptococcus PyogenesDocument6 pagesVirulence Factors of Streptococcus PyogenesAmador GielasNo ratings yet
- Superficial MycosisDocument17 pagesSuperficial Mycosisapi-19969058100% (2)
- 7 ImunisasiDocument85 pages7 ImunisasiElfa RiniNo ratings yet
- Gashu Afework 23Document88 pagesGashu Afework 23Alemayehu KebedeNo ratings yet
- Glomerulo Nephritis PathologyDocument3 pagesGlomerulo Nephritis PathologysssajiNo ratings yet
- Blood ComponentsDocument17 pagesBlood ComponentsJohnSmithNo ratings yet
- Scrub Typhus Guideline On Prevention and ControlDocument3 pagesScrub Typhus Guideline On Prevention and ControlVir balNo ratings yet
- Oral Allergy SyndromeDocument3 pagesOral Allergy SyndromeAlan A. AlexanderNo ratings yet
- SpirochetosisDocument14 pagesSpirochetosisBhaveshNo ratings yet
- Betnesol NDocument7 pagesBetnesol NKûmår ĀmrītëshNo ratings yet
- Microbiology Memorization SheetDocument5 pagesMicrobiology Memorization Sheetalobrien100% (1)
- 1 s2.0 S0882401023003340 MainDocument10 pages1 s2.0 S0882401023003340 MainEzekiel GreenNo ratings yet