You might also like
- What Looks Like Crazy On An Ordinary DayDocument9 pagesWhat Looks Like Crazy On An Ordinary Dayapi-271170207100% (1)
- Step by Step Guide to Foreskin Restoration: The Natural Foreskin Restoration Treatment That Actually WorksFrom EverandStep by Step Guide to Foreskin Restoration: The Natural Foreskin Restoration Treatment That Actually WorksNo ratings yet
- Immediate Care of The NewbornDocument4 pagesImmediate Care of The NewbornGrace Ordinario Sabordo100% (1)
- Systemic Pathology Mnemonics Part IDocument18 pagesSystemic Pathology Mnemonics Part IHanan HamdyNo ratings yet
- Perineal Genital Care 4Document32 pagesPerineal Genital Care 4Ashley AbaNo ratings yet
- PERILIGHT EXPOSUREperinealcare Enema PDFDocument7 pagesPERILIGHT EXPOSUREperinealcare Enema PDFDanna Uy100% (1)
- Perineal Care ModuleDocument7 pagesPerineal Care ModuleHEIDE BASING-ANo ratings yet
- Midterm Nucama 460Document7 pagesMidterm Nucama 460Reysel MonteroNo ratings yet
- Module 14 Care of A Family Experiencing A Postpartum Complication Puerperal 1Document14 pagesModule 14 Care of A Family Experiencing A Postpartum Complication Puerperal 1Blair AnnNo ratings yet
- Group ReportingDocument9 pagesGroup ReportingHeli, Jny A.No ratings yet
- Antenatal ExaminationDocument18 pagesAntenatal ExaminationMiu MiuNo ratings yet
- Newborn Assessment and AbnormalitiesDocument18 pagesNewborn Assessment and Abnormalitieskimberson100% (4)
- NCM 102: Gynecology Nursing ManagementDocument7 pagesNCM 102: Gynecology Nursing ManagementdubhieNo ratings yet
- Perineal Care: Michael H. Esmilla, RN, MANDocument15 pagesPerineal Care: Michael H. Esmilla, RN, MANHannah Leigh CastilloNo ratings yet
- Cebu Institute of Technology University N. Bacalso Ave., Cebu City Philippines College of Nursing and Allied Health SciencesDocument4 pagesCebu Institute of Technology University N. Bacalso Ave., Cebu City Philippines College of Nursing and Allied Health SciencesMikha BorcesNo ratings yet
- Explain The Principles Invloved in Perineal Care and Perilite ExposureDocument5 pagesExplain The Principles Invloved in Perineal Care and Perilite ExposureCarmel Marie VenezuelaNo ratings yet
- O o o o o o O: DescriptionDocument34 pagesO o o o o o O: DescriptionDarren BalbasNo ratings yet
- Finalrationale CAGABCABDocument9 pagesFinalrationale CAGABCABCagabcab Canibel MelanyNo ratings yet
- Genitalia AssessmentDocument99 pagesGenitalia AssessmentGloriaCoronado75% (8)
- Essential Newborn Care Protocol: Warsame, Ahmed Sebanes, Kimberky Mae Silao, Emee JoyDocument35 pagesEssential Newborn Care Protocol: Warsame, Ahmed Sebanes, Kimberky Mae Silao, Emee JoyKathlyn SunicoNo ratings yet
- CHN Finals-ReviewerDocument14 pagesCHN Finals-ReviewerKayobi BuenviajeNo ratings yet
- DR Technique ChecklistDocument8 pagesDR Technique ChecklistPATRICIA JULIANNE CASTAÑETO RIVERANo ratings yet
- NCM 107 SKL FinalsDocument33 pagesNCM 107 SKL FinalsCyriz Ann Mae PacisNo ratings yet
- Einc Lectures - CeDocument5 pagesEinc Lectures - Ceboxed juiceNo ratings yet
- Upper Genital Tract InfectionDocument2 pagesUpper Genital Tract InfectiondanielNo ratings yet
- Purposes:: Perineal CareDocument4 pagesPurposes:: Perineal CareGodfrey AntolinNo ratings yet
- LRPD InglesDocument5 pagesLRPD InglesYuleika Zulema Pachas MachaNo ratings yet
- Perineal Care and CatheterizationDocument10 pagesPerineal Care and CatheterizationHarold DiasanaNo ratings yet
- Abnormalities of The Puerperium: Puerperal PyrexiaDocument28 pagesAbnormalities of The Puerperium: Puerperal Pyrexiadrravindermehetrey100% (2)
- Reviewer in NCMDocument12 pagesReviewer in NCMtamsmadjad18No ratings yet
- High Risk School Age and AdolescentDocument6 pagesHigh Risk School Age and AdolescentRamos, Janica De VeraNo ratings yet
- Communicable Diseases Affecting The Reproductive SystemDocument49 pagesCommunicable Diseases Affecting The Reproductive SystemJR Rolf NeuqeletNo ratings yet
- Presentation 4Document28 pagesPresentation 4Carmel Marie VenezuelaNo ratings yet
- Intrapartum: Delivery Room Technique PurposeDocument8 pagesIntrapartum: Delivery Room Technique PurposeRoshin TejeroNo ratings yet
- DR Technique ChecklistDocument8 pagesDR Technique ChecklistChristine Joy MolinaNo ratings yet
- Intrapartum: Delivery Room Technique PurposeDocument8 pagesIntrapartum: Delivery Room Technique PurposeChristine Joy MolinaNo ratings yet
- DR Technique Checklist101Document8 pagesDR Technique Checklist101Christine Joy MolinaNo ratings yet
- DR Technique Checklist 1Document10 pagesDR Technique Checklist 1Omar James Abdulgani LimNo ratings yet
- Postoperative Nursing CareDocument2 pagesPostoperative Nursing CareYeana AlonNo ratings yet
- NCM 109 RLE PROCEDURE Vaginal Suppository InsertionDocument6 pagesNCM 109 RLE PROCEDURE Vaginal Suppository InsertionFRANCES EMMA NIERE GUMAHADNo ratings yet
- Newbornassessment EDITED FOR LECTUREDocument37 pagesNewbornassessment EDITED FOR LECTUREAllen Caine TaabbilNo ratings yet
- Perineal CareDocument4 pagesPerineal CareHONEY NICOLE PACOMANo ratings yet
- Chang AnDocument36 pagesChang AnErrol LlanesNo ratings yet
- Newborn Care ChecklistDocument5 pagesNewborn Care Checklistburntashes100% (1)
- GYLLE Meningitis Otitis Media Pertussis Pneumonia Rotavirus 1Document37 pagesGYLLE Meningitis Otitis Media Pertussis Pneumonia Rotavirus 1Marie Ashley CasiaNo ratings yet
- Immediate Care of The NewbornDocument4 pagesImmediate Care of The Newbornmelinda100% (1)
- Perineal CareDocument8 pagesPerineal Careclint xavier odango100% (1)
- Intrapartum: Delivery Room Technique PurposeDocument7 pagesIntrapartum: Delivery Room Technique Purposesharmena harunNo ratings yet
- EpilepsyDocument9 pagesEpilepsyEcha Kania DivaNo ratings yet
- External DoucheDocument6 pagesExternal DoucheSha AbdulaNo ratings yet
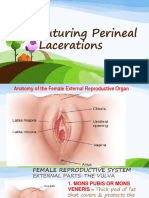
- Suturing Perineal LacerationsDocument49 pagesSuturing Perineal LacerationsOfel Santillan100% (2)
- Immediate Care of The NewbornDocument10 pagesImmediate Care of The NewbornRaffy100% (2)
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument1 pageNursing Care Plan: Cues Objectives Interventions Rationale EvaluationAugustine kahlil ArquizaNo ratings yet
- Skill 13 (1) ..Collection of A MidstreamDocument1 pageSkill 13 (1) ..Collection of A MidstreamnetsquadNo ratings yet
- Postpartal ComplicationDocument4 pagesPostpartal ComplicationHanna AligatoNo ratings yet
- Elimination - Urinary and BowelDocument58 pagesElimination - Urinary and BowelAnn A.No ratings yet
- Manual For Basic Procedure - UpdateDocument19 pagesManual For Basic Procedure - UpdateAssasination Classroom100% (1)
- For EmailDocument1 pageFor EmailJonSabaniaNo ratings yet
- Perineal Care FinalDocument9 pagesPerineal Care Finalp4sion100% (2)
- ReviewerDocument3 pagesReviewerJhayneNo ratings yet
- Preparation of BuffersDocument5 pagesPreparation of BuffersJULLIENE IVES BUQUIDNo ratings yet
- Experiment No. 2 CarbohydratesDocument2 pagesExperiment No. 2 CarbohydratesYellow100% (1)
- Experiment No1 Protein AnalysisDocument3 pagesExperiment No1 Protein AnalysisYellowNo ratings yet
- Republic of The Philippines Cavite State University Don Severino Delas Alas Campus Indang, CaviteDocument6 pagesRepublic of The Philippines Cavite State University Don Severino Delas Alas Campus Indang, CaviteYellowNo ratings yet
- Buquid Grades ExampleDocument1 pageBuquid Grades ExampleYellowNo ratings yet
- Note To Learners: Plan A 60-Minute Fitness Program Daily From Warm-Up To Cooling Down and Allot Time in The Morning To Execute ItDocument1 pageNote To Learners: Plan A 60-Minute Fitness Program Daily From Warm-Up To Cooling Down and Allot Time in The Morning To Execute ItYellowNo ratings yet
- Physical Fitness Score CardDocument2 pagesPhysical Fitness Score CardYellowNo ratings yet
- Reference 2Document4 pagesReference 2Tari De ArimbieNo ratings yet
- Surgery 4 - Answers v1 (Wide)Document55 pagesSurgery 4 - Answers v1 (Wide)Humzala BashamNo ratings yet
- Masunaga Renaissance ManDocument24 pagesMasunaga Renaissance ManEri ArchavliNo ratings yet
- District Health Management Information System (Dhmis) PolicyDocument38 pagesDistrict Health Management Information System (Dhmis) PolicySiti AlfianaNo ratings yet
- Cross ReactivityDocument40 pagesCross ReactivityjanieinMNNo ratings yet
- Prevention of Pressure Ulcers Among Individuals Cared For in The Prone Position: Lessons For The COVID-19 EmergencyDocument9 pagesPrevention of Pressure Ulcers Among Individuals Cared For in The Prone Position: Lessons For The COVID-19 Emergencyzaenab anissaNo ratings yet
- WHOReportHearingCare EnglishDocument49 pagesWHOReportHearingCare EnglishRicardo MartinezNo ratings yet
- Microcarrier Cell Culture ScaleUp Procedures HandbookDocument32 pagesMicrocarrier Cell Culture ScaleUp Procedures HandbookDolphingNo ratings yet
- HuwaSan Brochure PDFDocument8 pagesHuwaSan Brochure PDFKaneki KenNo ratings yet
- Urolithiasis SeminarDocument50 pagesUrolithiasis SeminarSiddharth GuptaNo ratings yet
- Bio-Enhancers: A Potential Tool To Improve Soil Fertility and Plant Health in Organic Production of Horticultural CropsDocument19 pagesBio-Enhancers: A Potential Tool To Improve Soil Fertility and Plant Health in Organic Production of Horticultural CropsAzizrahman AbubakarNo ratings yet
- HFOV - Dragonfly - The Next Primary Mode of Neonatal VentilationDocument16 pagesHFOV - Dragonfly - The Next Primary Mode of Neonatal VentilationflowlineNo ratings yet
- School Nursing ServicesDocument22 pagesSchool Nursing ServicesJimmellee EllenNo ratings yet
- MSC in Clinical Dermatology: (MSCCD) Course ProspectusDocument6 pagesMSC in Clinical Dermatology: (MSCCD) Course ProspectusxaltraNo ratings yet
- Referat 6. Daftar Pustaka HipertiroidDocument2 pagesReferat 6. Daftar Pustaka HipertiroidSigit Dwi RahardjoNo ratings yet
- Esi Scheme in Tamil Nadu: Directorate of Medical and Rural Health Services (Esi) Chennai - 6Document33 pagesEsi Scheme in Tamil Nadu: Directorate of Medical and Rural Health Services (Esi) Chennai - 6Ash MohNo ratings yet
- Anatomy Rat Lab Report Digestive & RespiratoryDocument11 pagesAnatomy Rat Lab Report Digestive & RespiratoryHema Jothy0% (1)
- Chapter One 1.0 Introduction/Literature Review 1.1 Background of StudyDocument62 pagesChapter One 1.0 Introduction/Literature Review 1.1 Background of StudySolomonNo ratings yet
- Nasm FlashcardsDocument172 pagesNasm FlashcardsHilde Camp100% (3)
- Artikel GasDocument113 pagesArtikel GasI Gusti Ayu Astrid SNo ratings yet
- Characterization of Ube Coconut Pulp Muffin Fortified With JuteDocument95 pagesCharacterization of Ube Coconut Pulp Muffin Fortified With JuteroselynmaenavarroNo ratings yet
- Bài Writing VstepDocument9 pagesBài Writing VstepThuỳ Linh Nguyễn ThịNo ratings yet
- Prelims: Test SeriesDocument75 pagesPrelims: Test SeriesAnil SharmaNo ratings yet
- Basic Standards For Organic Rice Cultivation:: I. AdmissibilityDocument6 pagesBasic Standards For Organic Rice Cultivation:: I. Admissibilitytogaten10aNo ratings yet
- FIA Meter: Fluorescence Immunoassay Rapid Quantitative TestDocument2 pagesFIA Meter: Fluorescence Immunoassay Rapid Quantitative TestOkura JoshuaNo ratings yet
- Executive Function PDFDocument2 pagesExecutive Function PDFpc2webNo ratings yet
- Introduction To Contemporary Social Problems PDFDocument90 pagesIntroduction To Contemporary Social Problems PDFhayenje rebecca100% (1)
- Medical Surgical Nursing Exams BoardDocument36 pagesMedical Surgical Nursing Exams BoardCINDY� BELMESNo ratings yet