You might also like
- Ob2 Sas 13Document8 pagesOb2 Sas 13Ralph Louie ManagoNo ratings yet
- 3 March 6, 2022 Postpartum Complications: Module No. Date: TopicDocument10 pages3 March 6, 2022 Postpartum Complications: Module No. Date: Topicanon ymousNo ratings yet
- M102 Remedial ModuleDocument14 pagesM102 Remedial ModuleMA. JYRELL BONITONo ratings yet
- Module 5 - MCN TransesDocument6 pagesModule 5 - MCN TransesCarl UyNo ratings yet
- Postpatum Obstetric EmergenciesDocument46 pagesPostpatum Obstetric EmergenciesSooryaNo ratings yet
- NCM109 Maternal - Child Nursing (A-C) - Module 5Document6 pagesNCM109 Maternal - Child Nursing (A-C) - Module 5iratsyukieNo ratings yet
- Module 5 - MCN TransesDocument6 pagesModule 5 - MCN TransesCarl UyNo ratings yet
- Postpartum ComplicationsDocument6 pagesPostpartum ComplicationsALCANTARA ALYANNANo ratings yet
- Generic NameDocument3 pagesGeneric NameSittie Nashieva A. UsmanNo ratings yet
- Uterine Inversion Uterine Rupture Amniotic Fluid Embolism MaglangitDocument6 pagesUterine Inversion Uterine Rupture Amniotic Fluid Embolism Maglangitmaglangitjoannamarie1920No ratings yet
- POSTPARTUM-HEMORRHAGE LecDocument13 pagesPOSTPARTUM-HEMORRHAGE LecMay MayNo ratings yet
- Post Partum Haemorrhage 1 - LoadDocument47 pagesPost Partum Haemorrhage 1 - Loadkalpananstl100% (1)
- Nursing Care of The High Risk Postpartal ClientDocument11 pagesNursing Care of The High Risk Postpartal ClientMarielle J GarciaNo ratings yet
- MCN 80 114Document35 pagesMCN 80 114Jianne CaloNo ratings yet
- Bhabani OBG SeminarDocument28 pagesBhabani OBG SeminarSonali SamalNo ratings yet
- HIGH RISK AND SICK MOTHER 5PsDocument16 pagesHIGH RISK AND SICK MOTHER 5Psbaracream.exeNo ratings yet
- Subinvolution of The UterusDocument5 pagesSubinvolution of The UterusJanica Rose Maloloy-onNo ratings yet
- Precipitate LaborDocument3 pagesPrecipitate LaborAbbeygale Galan100% (2)
- Injuries To The Birth CanalDocument67 pagesInjuries To The Birth CanalnamitaNo ratings yet
- Subacute Uterine Inversion With Shock - A Distinct Surgical ManagementDocument3 pagesSubacute Uterine Inversion With Shock - A Distinct Surgical ManagementBima GhovaroliyNo ratings yet
- Operative Vaginal DeliveryDocument8 pagesOperative Vaginal DeliveryGerben VillanuevaNo ratings yet
- Inversion, Retained Placenta, AfeDocument95 pagesInversion, Retained Placenta, Afesushma sharmaNo ratings yet
- NCM109 RLE 1st Term ReviewerDocument40 pagesNCM109 RLE 1st Term ReviewerCarelle Faith Serrano AsuncionNo ratings yet
- LACERATION - Large Laceration Can Be VAGINAL Laceration - Easier To Locate andDocument2 pagesLACERATION - Large Laceration Can Be VAGINAL Laceration - Easier To Locate andرجمه ديوانNo ratings yet
- Ncma219 Week 4Document9 pagesNcma219 Week 4Aruxi YoshiNo ratings yet
- Uterine Atony 1Document16 pagesUterine Atony 1Dèyanira Jazsmin SilosNo ratings yet
- Module 4F Operative Obstetrics PDFDocument11 pagesModule 4F Operative Obstetrics PDFYori Nicole Martine CuyosNo ratings yet
- Genital Tract InjuriesDocument74 pagesGenital Tract InjuriesDevuchandana RNo ratings yet
- OBSTETRICAL HEMORRHAGE REVISED ScribdDocument34 pagesOBSTETRICAL HEMORRHAGE REVISED Scribdindah.obginuh.jul20No ratings yet
- NCM 102 OB Abnormal 2Document113 pagesNCM 102 OB Abnormal 2Maria Garcia Pimentel Vanguardia IINo ratings yet
- Erpoc CmeDocument20 pagesErpoc CmeSharon J StephenNo ratings yet
- Complications of Post PartumDocument49 pagesComplications of Post PartumakritiNo ratings yet
- Placental Abnormalities Normal Placenta: © Mary Andrea G. Agorilla, Ust-Con 2021 - 1Document3 pagesPlacental Abnormalities Normal Placenta: © Mary Andrea G. Agorilla, Ust-Con 2021 - 1Mary AgorillaNo ratings yet
- Birth Canal Injuries Final LectureDocument63 pagesBirth Canal Injuries Final Lecturepeter njoguNo ratings yet
- 3rd Stage ComplicationsDocument84 pages3rd Stage ComplicationsDream100% (1)
- POSTPARTUM HAEMORRHAGE CME FinalDocument14 pagesPOSTPARTUM HAEMORRHAGE CME FinalAdaha AngelNo ratings yet
- Management of Uterine Inversion: Operative TechniquesDocument4 pagesManagement of Uterine Inversion: Operative TechniquesMuhammad AzkaNo ratings yet
- Obstetrics Cards 19 30 PDFDocument81 pagesObstetrics Cards 19 30 PDFNavid BabluNo ratings yet
- Induction of LabourDocument51 pagesInduction of LabourDuncan Jackson100% (1)
- Complication On Labor and DeliveryDocument5 pagesComplication On Labor and DeliveryMeryville JacildoNo ratings yet
- NFDN 2004 - Unit 4.3 - JLB StudentDocument43 pagesNFDN 2004 - Unit 4.3 - JLB StudentkendrabooboooNo ratings yet
- NRG 204 MidtermDocument80 pagesNRG 204 MidtermKYLA MERCADONo ratings yet
- Ob EmergenciesDocument58 pagesOb Emergenciessanthiyasandy100% (1)
- Post-Partum Hge - @medicine - Way2Document6 pagesPost-Partum Hge - @medicine - Way2saeed hasan saeedNo ratings yet
- Emotional Support in The Immediate Post Partum 1. Taking PhaseDocument3 pagesEmotional Support in The Immediate Post Partum 1. Taking PhaseApRil Anne BalanonNo ratings yet
- Nle - High-Risk PregnancyDocument113 pagesNle - High-Risk Pregnancytachycardia01No ratings yet
- Gestational-Condition 2Document9 pagesGestational-Condition 2Trisha OloresisimoNo ratings yet
- Caesarian Birth - Maternal and Child NursingDocument10 pagesCaesarian Birth - Maternal and Child NursingSofia ResolNo ratings yet
- Early Pregnancy Complications: Ectopic Pregnancy Gestational Trophoblastic Disease Ji Aggasid, JanniecelDocument60 pagesEarly Pregnancy Complications: Ectopic Pregnancy Gestational Trophoblastic Disease Ji Aggasid, JanniecelmedicoNo ratings yet
- Joshi Abhishek F.Y.P.B.B.SC - Nursing Govt College of Nursing JamnagarDocument49 pagesJoshi Abhishek F.Y.P.B.B.SC - Nursing Govt College of Nursing JamnagarPoonam RanaNo ratings yet
- PPT Book ReadingDocument20 pagesPPT Book ReadingOctaria SaputraNo ratings yet
- LacerationsDocument2 pagesLacerationsGoldyNo ratings yet
- Complications of PostpartumDocument10 pagesComplications of PostpartumAlverastine AnNo ratings yet
- ACFrOgB40CYYfaqy K PEr1l2pQYS7J9CKoF1MzNRgUdEeaerp5y-GUUcxhhLpG-m5OUou-0hSVvKydlpjOQw2r0JNNDJa05hIf3kh47Kq6Qb3Lc4EbZZJrZnskvwOSk 94JNpKiPOaPE eXRxjIDocument6 pagesACFrOgB40CYYfaqy K PEr1l2pQYS7J9CKoF1MzNRgUdEeaerp5y-GUUcxhhLpG-m5OUou-0hSVvKydlpjOQw2r0JNNDJa05hIf3kh47Kq6Qb3Lc4EbZZJrZnskvwOSk 94JNpKiPOaPE eXRxjIJomer Levi PortuguezNo ratings yet
- CMCP M1Document312 pagesCMCP M1evangdelacruz1010No ratings yet
- Hypotonic and Hypertonic Contractions and Precipitate LabourDocument3 pagesHypotonic and Hypertonic Contractions and Precipitate LabourRebecca ApeladoNo ratings yet
- NCM 104 Notes PrelimsDocument14 pagesNCM 104 Notes PrelimsAngel MoncadaNo ratings yet
- Complication & Minor Ailments of PuerperiumDocument61 pagesComplication & Minor Ailments of PuerperiumMohammed AbdNo ratings yet
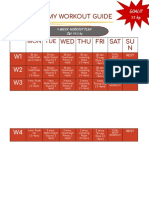
- My Workout GuideDocument2 pagesMy Workout GuideHanna AligatoNo ratings yet
- My Workout GuideDocument2 pagesMy Workout GuideHanna AligatoNo ratings yet
- High Risk NewbornDocument4 pagesHigh Risk NewbornHanna AligatoNo ratings yet
- Physical or Developmental ChallengeDocument7 pagesPhysical or Developmental ChallengeHanna AligatoNo ratings yet
- Uterine MYOMADocument5 pagesUterine MYOMARoss Manalang100% (2)
- 28099453C Case Study 3Document27 pages28099453C Case Study 3Alice HuiiNo ratings yet
- An Ayurvedic Review of Uterine FibroidsDocument5 pagesAn Ayurvedic Review of Uterine FibroidsIJAR JOURNALNo ratings yet
- Abdominal HysterectomyDocument23 pagesAbdominal Hysterectomytata marethaNo ratings yet
- Maleand Female Reproductive System @muhammad Usama BilalDocument4 pagesMaleand Female Reproductive System @muhammad Usama BilalumerkhanNo ratings yet
- Reproductive - Systems - in - Vertebrates ss2Document12 pagesReproductive - Systems - in - Vertebrates ss2Ezeh PrincessNo ratings yet
- m4 MCN - m4Document140 pagesm4 MCN - m4Kristine KimNo ratings yet
- Sexuality Today 11th Edition Kelly Solution ManualDocument16 pagesSexuality Today 11th Edition Kelly Solution Manualjacob100% (24)
- 10 Science Notes 08 How Do Organisms Reproduce 1Document10 pages10 Science Notes 08 How Do Organisms Reproduce 1All Rounder HindustanNo ratings yet
- Uterine Prolapse in Cattle - 2Document11 pagesUterine Prolapse in Cattle - 2frankyNo ratings yet
- TOG Vaginal HysterectomyDocument6 pagesTOG Vaginal HysterectomyYasmin AlkhatibNo ratings yet
- Female Reproductive System: Sexual Health UnitDocument47 pagesFemale Reproductive System: Sexual Health UnitСухоставець Наталія ПетрівнаNo ratings yet
- Lesson Plan On ANTE NATAL CARE FINALDocument33 pagesLesson Plan On ANTE NATAL CARE FINALrenu100% (1)
- Vacuum Delivery Case StudyDocument40 pagesVacuum Delivery Case StudyMoni Mbumba Meleke60% (5)
- Cases in ObgDocument41 pagesCases in ObgShriyansh Chahar0% (1)
- Cesarean BirthDocument35 pagesCesarean BirthJhonny Paul RamosNo ratings yet
- Rat DissectionDocument9 pagesRat Dissectionapi-296981910No ratings yet
- Displacement of The Uterus: DR Sahar Anwar RizkDocument32 pagesDisplacement of The Uterus: DR Sahar Anwar RizkWida Ratna SariNo ratings yet
- INTRO, Physiological Changes IN PUERPERIUM-UTERUSDocument26 pagesINTRO, Physiological Changes IN PUERPERIUM-UTERUSrachael annorNo ratings yet
- The Phases of Menstrual CycleDocument5 pagesThe Phases of Menstrual CycleKristine AlejandroNo ratings yet
- Total and Acute Uterine Inversion After Delivery A Case Report PDFDocument4 pagesTotal and Acute Uterine Inversion After Delivery A Case Report PDFatika sgrtNo ratings yet
- 2 - Anatomy and Histology of Female Genital TractDocument26 pages2 - Anatomy and Histology of Female Genital TractHervis FantiniNo ratings yet
- Adenomyosis A Sonographic DiagnosisDocument14 pagesAdenomyosis A Sonographic DiagnosisHelioNo ratings yet
- High Risk Labor and DeliveryDocument5 pagesHigh Risk Labor and DeliveryCarl John ManaloNo ratings yet
- Vet Obst Lecture 10 Cesarean in Domestic Farm and Pet AnimalsDocument41 pagesVet Obst Lecture 10 Cesarean in Domestic Farm and Pet Animalsgnpobs100% (1)
- Placenta Previa - MedscapeDocument5 pagesPlacenta Previa - MedscapeAnonymous jh87ryNo ratings yet
- Energetics in Acupuncture Pages 3Document98 pagesEnergetics in Acupuncture Pages 3Geeta SajjanNo ratings yet
- Spontaneous MiscarriageDocument14 pagesSpontaneous MiscarriageGomez VanessaNo ratings yet
- Student'S Gynaecology Notes: For Students, by StudentsDocument45 pagesStudent'S Gynaecology Notes: For Students, by StudentsAdli IsmailNo ratings yet
- Obstructed Labour (OL)Document34 pagesObstructed Labour (OL)ruhulcoc1No ratings yet