You might also like
- Another JurnalDocument4 pagesAnother JurnalReskyAmeliaHRNo ratings yet
- Diagnosis and Management of Microbial Keratitis: AIOS Guidelines ForDocument24 pagesDiagnosis and Management of Microbial Keratitis: AIOS Guidelines ForKukuh Rizwido PrasetyoNo ratings yet
- Choi Eye Emergencies 9.16Document3 pagesChoi Eye Emergencies 9.16pascutaNo ratings yet
- Ma 2021 Uveitis 101Document5 pagesMa 2021 Uveitis 101Jenny MaNo ratings yet
- Disease: Bacterial KeratitisDocument9 pagesDisease: Bacterial KeratitisDwi Ayu PrimadanaNo ratings yet
- mainDocument3 pagesmainomidazadmehr1375No ratings yet
- Dry Eye Disease GuideDocument25 pagesDry Eye Disease Guide215045 zulfa laili aNo ratings yet
- Corneal Atlas 2011Document20 pagesCorneal Atlas 2011Wentao Liu100% (3)
- GP Factsheet - Steroids and The EyeDocument6 pagesGP Factsheet - Steroids and The EyeBima RizkiNo ratings yet
- Ruptur BulbiDocument5 pagesRuptur BulbiseptrealtiNo ratings yet
- Aes 04 9Document6 pagesAes 04 9Ignasius HansNo ratings yet
- Guidelines For The Management of Corneal Ulcer WHODocument36 pagesGuidelines For The Management of Corneal Ulcer WHOichalledhaNo ratings yet
- Vernal Keratoconjunctivitis: Why Is Allergic Eye Disease A Problem For Eye Workers?Document3 pagesVernal Keratoconjunctivitis: Why Is Allergic Eye Disease A Problem For Eye Workers?darendraabimayuNo ratings yet
- Red Eye-Dr S BrodovskyDocument57 pagesRed Eye-Dr S BrodovskyLyndon EdanoNo ratings yet
- Management and Diagnosis of Viral, Bacterial, and Allergic ConjunctivitisDocument30 pagesManagement and Diagnosis of Viral, Bacterial, and Allergic ConjunctivitisAnonymous yyR4FGNo ratings yet
- KeratitisDocument21 pagesKeratitistifano_arian9684No ratings yet
- USMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyRating: 5 out of 5 stars5/5 (2)
- Principles of Eye Management in Stevens-Johnson Syndrome: Mittanamalli S. SridharDocument5 pagesPrinciples of Eye Management in Stevens-Johnson Syndrome: Mittanamalli S. SridharFarah RNo ratings yet
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3No ratings yet
- Herpes Zoster Ophthalmicus: Limits Advanced Journal List Help Journal List West J Emerg Med v.9 (3) 2008 AugDocument7 pagesHerpes Zoster Ophthalmicus: Limits Advanced Journal List Help Journal List West J Emerg Med v.9 (3) 2008 AugGio Vano NaihonamNo ratings yet
- Patient Diagnosis ResearchDocument7 pagesPatient Diagnosis ResearchAaron_Kim_Vela_4636No ratings yet
- Thesis On Corneal UlcerDocument6 pagesThesis On Corneal Ulcertonichristensenaurora100% (2)
- Evaluation of The Painful EyeDocument9 pagesEvaluation of The Painful EyeMuthia Farah AshmaNo ratings yet
- NLM Database Access and DisclaimerDocument5 pagesNLM Database Access and DisclaimerGung NandaNo ratings yet
- Posterior Uveitis HandoutDocument4 pagesPosterior Uveitis Handoutdanny wiryaNo ratings yet
- Complications in Eyelid Surgery 2016Document11 pagesComplications in Eyelid Surgery 2016María Alejandra Rojas MontenegroNo ratings yet
- Posterior UveitisDocument12 pagesPosterior UveitisReinaldoPutraNo ratings yet
- Literature Review On Corneal UlcerDocument7 pagesLiterature Review On Corneal Ulcerc5h4drzj100% (1)
- Management of Glaucoma Medication Induced Dry Eye DiseaseDocument7 pagesManagement of Glaucoma Medication Induced Dry Eye DiseaseMeilin ZulfatinNo ratings yet
- Ocular Myasthenia Gravis With Severe Blepharitis ADocument8 pagesOcular Myasthenia Gravis With Severe Blepharitis AGoran TomićNo ratings yet
- Group 4: Trapago Trebucias Trinidad Umiten Vega Ventura Villalon YabresDocument86 pagesGroup 4: Trapago Trebucias Trinidad Umiten Vega Ventura Villalon YabresHunterDrimsumNo ratings yet
- OpthaDocument5 pagesOpthavarun2k6No ratings yet
- Journal Reading: Update On The Management of Infectious KeratitisDocument35 pagesJournal Reading: Update On The Management of Infectious KeratitisninataniaaaNo ratings yet
- Vitreous Floaters: Publication DetailsDocument6 pagesVitreous Floaters: Publication Detailsmithaa octoviagnesNo ratings yet
- Introduction HzoDocument6 pagesIntroduction Hzoinggrid monicaNo ratings yet
- Guide to Managing Microbial KeratitisDocument30 pagesGuide to Managing Microbial KeratitisTatik Handayani100% (1)
- Blepharitis Disease and Its ManagementDocument7 pagesBlepharitis Disease and Its Managementνικος νικουNo ratings yet
- Corneal Ulcer - StatPearls - NCBI BookshelfDocument5 pagesCorneal Ulcer - StatPearls - NCBI BookshelfAngel LimNo ratings yet
- Staphylococcus Epidermidis End PDFDocument4 pagesStaphylococcus Epidermidis End PDFNisaNo ratings yet
- Bilateral Blindness Due To Pterygium - A Case ReportDocument3 pagesBilateral Blindness Due To Pterygium - A Case ReportDavid Al HavizNo ratings yet
- Comparison of A Preservative Free Nonsteroidal.Document7 pagesComparison of A Preservative Free Nonsteroidal.Danty IndriastutyNo ratings yet
- Confronting Corneal UlcersDocument9 pagesConfronting Corneal UlcersAfdhal MuhammadNo ratings yet
- Congenital Cataracts Causes, Symptoms and TreatmentDocument2 pagesCongenital Cataracts Causes, Symptoms and TreatmentKuchai BaruNo ratings yet
- Jurnal English JhuvanDocument12 pagesJurnal English JhuvanJhuvan FernandoNo ratings yet
- Conjunctivitis As A Manifestation of Wegener 'S GranulomatosisDocument5 pagesConjunctivitis As A Manifestation of Wegener 'S GranulomatosisAsd DsaNo ratings yet
- Orthodontic Lect 2Document16 pagesOrthodontic Lect 2Said SaidNo ratings yet
- Eye Infections PDFDocument10 pagesEye Infections PDFDara Agusti MaulidyaNo ratings yet
- Topical Tacrolimus For Corneal Subepithelial InfiltratesDocument4 pagesTopical Tacrolimus For Corneal Subepithelial InfiltratessrihandayaniakbarNo ratings yet
- HHS Public Access: Advances in Dry Eye Disease TreatmentDocument25 pagesHHS Public Access: Advances in Dry Eye Disease TreatmentjojdoNo ratings yet
- Dry Eye ThesisDocument5 pagesDry Eye ThesisPaperWritingServiceCollegeUK100% (2)
- 38surekha EtalDocument3 pages38surekha EtaleditorijmrhsNo ratings yet
- Amniotic Membrane Transplantation Combined With Antiviral and Steroid Therapy For Herpes Necrotizing Stromal KeratitisDocument7 pagesAmniotic Membrane Transplantation Combined With Antiviral and Steroid Therapy For Herpes Necrotizing Stromal KeratitisnelyNo ratings yet
- Clinical Profile of Patients of Snake Venom Ophthalmia Presenting To The Tertiary Health Care CentreDocument6 pagesClinical Profile of Patients of Snake Venom Ophthalmia Presenting To The Tertiary Health Care CentreIJAR JOURNALNo ratings yet
- Ocular Trauma 4Document22 pagesOcular Trauma 4leena khalidaNo ratings yet
- Cataract in Adults - UpToDateDocument25 pagesCataract in Adults - UpToDateKevin FernandezNo ratings yet
- Gabungan Materi FarmakoterapiDocument235 pagesGabungan Materi FarmakoterapiIndah PrayestiNo ratings yet
- Effects of Diamond Burr in Patients With RecurrentDocument7 pagesEffects of Diamond Burr in Patients With Recurrentsahoshi riveraNo ratings yet
- Causes of Eye DischargeDocument4 pagesCauses of Eye Dischargeabed alawiNo ratings yet
- Cataracts Pathophysiology and Managements: Abdulrahman Zaid AlshamraniDocument4 pagesCataracts Pathophysiology and Managements: Abdulrahman Zaid AlshamraniOcha24 TupamahuNo ratings yet
- Treating and Managing UveitisDocument4 pagesTreating and Managing UveitisMoses Karanja Jr.No ratings yet
- Treatment of Corneal Perforation With Lenticules From Small Incision Lenticule Extraction Surgery: A Preliminary Study of 6 PatientsDocument6 pagesTreatment of Corneal Perforation With Lenticules From Small Incision Lenticule Extraction Surgery: A Preliminary Study of 6 PatientsStephanie AureliaNo ratings yet
- v73 Supp 2 2018Document92 pagesv73 Supp 2 2018Stephanie AureliaNo ratings yet
- 2017 Understanding-Nystagmus v04Document48 pages2017 Understanding-Nystagmus v04Stephanie AureliaNo ratings yet
- 2020 Evaluation of Coronavirus in Tears and Conjunctival Secretions Xia - Et - Al COVID-19 PDFDocument6 pages2020 Evaluation of Coronavirus in Tears and Conjunctival Secretions Xia - Et - Al COVID-19 PDFvaleria giraldoNo ratings yet
- Clinical Management of Ocular Surface Squamous Neoplasia: A Review of The Current EvidenceDocument16 pagesClinical Management of Ocular Surface Squamous Neoplasia: A Review of The Current EvidenceStephanie AureliaNo ratings yet
- Conjunctivitis As Sole Symptom of COVID-19: A Case Report and Review of LiteratureDocument6 pagesConjunctivitis As Sole Symptom of COVID-19: A Case Report and Review of LiteratureMuhamad ZenNo ratings yet
- Stromal Lenticule Management of Corneal Perforations Oneyear Results 2155 9570 1000614Document4 pagesStromal Lenticule Management of Corneal Perforations Oneyear Results 2155 9570 1000614Stephanie AureliaNo ratings yet
- Conjunctivitis in COVID-19 PatientsDocument7 pagesConjunctivitis in COVID-19 PatientsStephanie AureliaNo ratings yet
- Blindness and Visual Impairment Profile of Rapid Assessment of Avoidable Blindness in Indonesia - Mia Rachmawati NDocument15 pagesBlindness and Visual Impairment Profile of Rapid Assessment of Avoidable Blindness in Indonesia - Mia Rachmawati NStephanie AureliaNo ratings yet
- Vision Academy of Subfoveal HemorrhageDocument2 pagesVision Academy of Subfoveal HemorrhageStephanie AureliaNo ratings yet
- Lacrimal Gland and Its Role On Dry Eyes PDFDocument12 pagesLacrimal Gland and Its Role On Dry Eyes PDFStephanie AureliaNo ratings yet
- Thyroid TumorDocument4 pagesThyroid TumorStephanie AureliaNo ratings yet
- Jamaophthalmology Wu 2020 BR 200003Document4 pagesJamaophthalmology Wu 2020 BR 200003andres felipe pulido ladinoNo ratings yet
- Modern Approach To The Treatment of Dry Eye, A Complex Multifactorial Disease: A P.I.C.A.S.S.O. Board ReviewDocument8 pagesModern Approach To The Treatment of Dry Eye, A Complex Multifactorial Disease: A P.I.C.A.S.S.O. Board ReviewStephanie AureliaNo ratings yet
- Raised ICP GuideDocument6 pagesRaised ICP GuideBeny RiliantoNo ratings yet
- Chek List JurnalDocument4 pagesChek List JurnalYid BajangNo ratings yet
- Shoulder DislocationDocument10 pagesShoulder DislocationStephanie AureliaNo ratings yet
- ADA Diabetic Neuropathy 2005Document7 pagesADA Diabetic Neuropathy 2005Penpun TocharoenkitNo ratings yet
- Diabetic Foot Ulcer ReviewDocument7 pagesDiabetic Foot Ulcer Reviewintan_ekleNo ratings yet
- Patogenesis Neuropatik DiabetikDocument8 pagesPatogenesis Neuropatik DiabetikStephanie AureliaNo ratings yet
- Guillain Barre SyndromeDocument8 pagesGuillain Barre SyndromeStephanie AureliaNo ratings yet
- Diabetic Foot PDFDocument9 pagesDiabetic Foot PDFStephanie AureliaNo ratings yet
- Bedah SarafDocument11 pagesBedah SarafStephanie AureliaNo ratings yet
- Acute Apendicitis LancetDocument10 pagesAcute Apendicitis LancetJeisson Castillo ChauxNo ratings yet
- 457 Full PDFDocument10 pages457 Full PDFStephanie AureliaNo ratings yet
- Nyeri NeuropatikDocument7 pagesNyeri NeuropatikStephanie AureliaNo ratings yet
- Nyeri NeuropatikDocument7 pagesNyeri NeuropatikStephanie AureliaNo ratings yet
- A Glimpse Into The Pathophysiology, Mechanisms, and Management of Neuropathic PainDocument7 pagesA Glimpse Into The Pathophysiology, Mechanisms, and Management of Neuropathic PainStephanie AureliaNo ratings yet
- Group 2 - Chapter 3 4Document7 pagesGroup 2 - Chapter 3 4Mira AurumtinNo ratings yet
- Customer Preferences For Restaurant Technology InnovationsDocument22 pagesCustomer Preferences For Restaurant Technology InnovationsDeepankar SinghNo ratings yet
- Academic Writing in English: Carolyn Brimley Norris, Ph.D. Language Services University of Helsinki 2015Document86 pagesAcademic Writing in English: Carolyn Brimley Norris, Ph.D. Language Services University of Helsinki 2015nasralaNo ratings yet
- Brown Creative Vintage Rustic Motivational Quote PosterDocument1 pageBrown Creative Vintage Rustic Motivational Quote PosterRafunzel Pe BandoquilloNo ratings yet
- Transforming Enterprises Through Diversity and Inclusion - ILODocument124 pagesTransforming Enterprises Through Diversity and Inclusion - ILODaniela GalvisNo ratings yet
- Transcript All Without NumberingDocument35 pagesTranscript All Without NumberingJohn Carl AparicioNo ratings yet
- Iep2014 15Document22 pagesIep2014 15api-245317729No ratings yet
- Tee Cube Collections Catalogue With Google Photos Link PDFDocument4 pagesTee Cube Collections Catalogue With Google Photos Link PDFKirat SinghNo ratings yet
- Calculus For EngineersDocument268 pagesCalculus For EngineersSr_Tabosa100% (1)
- The Nazi Master PlanDocument28 pagesThe Nazi Master PlanFolad109No ratings yet
- Level of Awareness on Anti-Violence LawDocument16 pagesLevel of Awareness on Anti-Violence LawWilliam VincentNo ratings yet
- United States Patent (19) : (52) U.S. C.260/583 KDocument5 pagesUnited States Patent (19) : (52) U.S. C.260/583 KkurniawanNo ratings yet
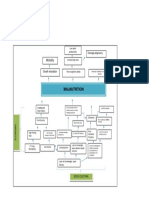
- Problem Tree Analysis MalnutritionDocument1 pageProblem Tree Analysis MalnutritionMho Dsb50% (6)
- Patient ProfileDocument9 pagesPatient ProfileValarmathiNo ratings yet
- CMTS SetupDocument68 pagesCMTS Setup'Jean CarlosNo ratings yet
- Revit For Presentations Graphics That Pop - Class HandoutDocument15 pagesRevit For Presentations Graphics That Pop - Class HandoutAutodesk University100% (1)
- Historic Struggle For Pakistan 1857 - 1947Document32 pagesHistoric Struggle For Pakistan 1857 - 1947The CSS Point82% (79)
- Md. Touhidul Islam: Professional ProfileDocument4 pagesMd. Touhidul Islam: Professional ProfileYaseen Fida HossainNo ratings yet
- The Role of Social Media On Leisure Preferences - A Research On The Participants of Outdoor Recreation Activities (#263492) - 230009Document10 pagesThe Role of Social Media On Leisure Preferences - A Research On The Participants of Outdoor Recreation Activities (#263492) - 230009Stella PadillaNo ratings yet
- Tawassulan Fik TjakrabuanaDocument6 pagesTawassulan Fik TjakrabuanafikditasresNo ratings yet
- Reflective Paper On Narcissism and LeadershipDocument6 pagesReflective Paper On Narcissism and Leadershipsema sharmaNo ratings yet
- A2 AQA History Britain NotesDocument7 pagesA2 AQA History Britain Notesjazzybob0% (1)
- Miniscrew-Assisted Mandibular Molar Protraction: A Case ReportDocument6 pagesMiniscrew-Assisted Mandibular Molar Protraction: A Case ReportAdvanced Research PublicationsNo ratings yet
- List of Intel Core I3 MicroprocessorsDocument3 pagesList of Intel Core I3 MicroprocessorsKing 79100% (1)
- Ambien Withdrawal TreatmentDocument6 pagesAmbien Withdrawal TreatmentSurvival SabariNo ratings yet
- Racionalidad Acotada 1Document4 pagesRacionalidad Acotada 1Hector J. RubiniNo ratings yet
- Effectiveness of Workplace Counseling On Employee Performance. A Case of Mumias Sugar Company Limited, KenyaDocument10 pagesEffectiveness of Workplace Counseling On Employee Performance. A Case of Mumias Sugar Company Limited, KenyainventionjournalsNo ratings yet
- Selection of Hazard Evaluation Techniques PDFDocument16 pagesSelection of Hazard Evaluation Techniques PDFdediodedNo ratings yet
- Competition Commission of India Economics Study Material Amp NotesDocument3 pagesCompetition Commission of India Economics Study Material Amp NotesRaghav DhillonNo ratings yet