You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- LRN Speaking Syllabus 2021 b2 c2 January 2021-Unlocked PDFDocument58 pagesLRN Speaking Syllabus 2021 b2 c2 January 2021-Unlocked PDFFotis Syropoulos100% (1)
- Effects of Warm Compresses On Decreased HyperthermiaDocument12 pagesEffects of Warm Compresses On Decreased HyperthermiaNur AiniNo ratings yet
- 2 PBDocument6 pages2 PBArOfaNo ratings yet
- Management of FebrileDocument9 pagesManagement of FebrileNur AiniNo ratings yet
- Comparison of Anti-Inflammatory Effects of IntenseDocument6 pagesComparison of Anti-Inflammatory Effects of IntenseNur AiniNo ratings yet
- Recognition and ManagementDocument7 pagesRecognition and ManagementNur AiniNo ratings yet
- Warm Compress On Among Body TemperatureDocument12 pagesWarm Compress On Among Body TemperatureNur AiniNo ratings yet
- The Pathogenesis of Fever-Induced Febrile SeizuresDocument7 pagesThe Pathogenesis of Fever-Induced Febrile SeizuresNur AiniNo ratings yet
- Effect of Warm Water CompressDocument6 pagesEffect of Warm Water CompressNur AiniNo ratings yet
- Evaluation Patients With Febrile C Risk FactorsDocument7 pagesEvaluation Patients With Febrile C Risk FactorsNur AiniNo ratings yet
- Current Understanding of Febrile Seizures and Their Long-Term OutcomesDocument5 pagesCurrent Understanding of Febrile Seizures and Their Long-Term OutcomesNur AiniNo ratings yet
- MANAGEMENT OF FEBRILE in ChildrenDocument12 pagesMANAGEMENT OF FEBRILE in ChildrenNur AiniNo ratings yet
- IJBMPH - Volume 1 - Issue 1 - Pages 23-29.pdf DoajDocument9 pagesIJBMPH - Volume 1 - Issue 1 - Pages 23-29.pdf DoajNur AiniNo ratings yet
- Concepts DoajDocument21 pagesConcepts DoajNur AiniNo ratings yet
- 3 General Assessment For PatientsDocument19 pages3 General Assessment For PatientsNur AiniNo ratings yet
- Assessment-Of-Causative-Factors-Of-Febrile-Seizure-Related-To-A-Group-Of-Children-In-Iran - PDF PerpusnasDocument5 pagesAssessment-Of-Causative-Factors-Of-Febrile-Seizure-Related-To-A-Group-Of-Children-In-Iran - PDF PerpusnasNur AiniNo ratings yet
- 2 Hospital DirectionsDocument20 pages2 Hospital DirectionssinggihNo ratings yet
- Webinar PI Dan IADDocument23 pagesWebinar PI Dan IADNur AiniNo ratings yet
- Paul 2015Document8 pagesPaul 2015Nur AiniNo ratings yet
- The Pathogenesis of Fever-Induced Febrile SeizuresDocument8 pagesThe Pathogenesis of Fever-Induced Febrile SeizuresNur AiniNo ratings yet
- Evaluation Patients With Febrile C Risk FactorsDocument7 pagesEvaluation Patients With Febrile C Risk FactorsNur AiniNo ratings yet
- 1 Cross Culture - An Australian PerspectiveDocument36 pages1 Cross Culture - An Australian PerspectiveNur AiniNo ratings yet
- 1 Cross Culture - An Australian PerspectiveDocument36 pages1 Cross Culture - An Australian PerspectiveNur AiniNo ratings yet
- Musik SeLIMuTDocument12 pagesMusik SeLIMuTNina PangestutiNo ratings yet
- Jurnal Kejang Demam PDFDocument8 pagesJurnal Kejang Demam PDFsamiraNo ratings yet
- Aloe Vera DoajDocument8 pagesAloe Vera DoajNur AiniNo ratings yet
- 1 - 91-Article Text-516-1-10-20200430-1Document7 pages1 - 91-Article Text-516-1-10-20200430-1Kisna SoniyaNo ratings yet
- The Pathogenesis of Fever-Induced Febrile SeizuresDocument8 pagesThe Pathogenesis of Fever-Induced Febrile SeizuresNur AiniNo ratings yet
- Jurnal Internasional (Kecemasan PraOperasi)Document10 pagesJurnal Internasional (Kecemasan PraOperasi)Nur AiniNo ratings yet
- Concepts DoajDocument21 pagesConcepts DoajNur AiniNo ratings yet
- Qualitative ResearchDocument6 pagesQualitative Researchtoshiro lazarteNo ratings yet
- Easa Management System Assessment ToolDocument40 pagesEasa Management System Assessment ToolAdam Tudor-danielNo ratings yet
- Laboratory ManagementDocument6 pagesLaboratory ManagementJamille CarayuganNo ratings yet
- Unit 7Document12 pagesUnit 7ALEXANDRA VACANo ratings yet
- Risk List TemplateDocument3 pagesRisk List Templatemanjunathaug3No ratings yet
- Weekly-Home-Learning-Plan Q1 Week 1Document2 pagesWeekly-Home-Learning-Plan Q1 Week 1Cla RisaNo ratings yet
- Treatment of Insomnia Through The Use of ElectrosleepDocument13 pagesTreatment of Insomnia Through The Use of ElectrosleepEnricoNo ratings yet
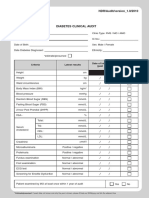
- Borang Diabetes Clinical AuditDocument2 pagesBorang Diabetes Clinical AuditHafizzah Mohd FirdausNo ratings yet
- Midline Diastema Correction Utilizing Clinical Application of M-Spring A Case ReportDocument3 pagesMidline Diastema Correction Utilizing Clinical Application of M-Spring A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Teaching P.E. and Health in The Elementary GradesDocument20 pagesTeaching P.E. and Health in The Elementary GradesTech VlogsNo ratings yet
- 5.1 EnglDocument3 pages5.1 Englmarie vegaNo ratings yet
- Superficial Parotidectomy TRZDocument20 pagesSuperficial Parotidectomy TRZdokteraan100% (3)
- Text Information and MediaDocument41 pagesText Information and MediaRegine GuavezNo ratings yet
- LF2F Parental Consent and Waiver FormDocument6 pagesLF2F Parental Consent and Waiver FormDreSznNo ratings yet
- lastCleanException 20221129215815Document2 pageslastCleanException 20221129215815poisoxnedNo ratings yet
- Set1 (Answer? English) std10Document10 pagesSet1 (Answer? English) std10Saiyam JainNo ratings yet
- Erikson's Psycho-Social Theory of DevelopmentDocument10 pagesErikson's Psycho-Social Theory of DevelopmentCielo DasalNo ratings yet
- The Last PsychDocument381 pagesThe Last PsychBen BeasleyNo ratings yet
- Psychotherapeutic Interventions (Management Therapy)Document5 pagesPsychotherapeutic Interventions (Management Therapy)Jenny Juniora AjocNo ratings yet
- NCM 105 Nutrition and Diet Therapy Legal MandatesDocument47 pagesNCM 105 Nutrition and Diet Therapy Legal MandatesLea Angel Dominique MacamNo ratings yet
- Cosmed MetabolicDocument175 pagesCosmed MetabolicAsrullahNo ratings yet
- Introduction To Chemguard PDFDocument2 pagesIntroduction To Chemguard PDFjoana ramirezNo ratings yet
- Clinical Hypnosis For The Alleviation of TinnitusDocument4 pagesClinical Hypnosis For The Alleviation of TinnitusIsabelNo ratings yet
- Depression in Older Adults (Problem Tree Analysis)Document8 pagesDepression in Older Adults (Problem Tree Analysis)Ishie De LeonNo ratings yet
- Isotretinoin Oral Uses, Side Effects, Interactions, Pictures, Warnings & Dosing - WebMDDocument1 pageIsotretinoin Oral Uses, Side Effects, Interactions, Pictures, Warnings & Dosing - WebMDLynn Abou TayehNo ratings yet
- NUR153 IG Session6Document9 pagesNUR153 IG Session6ira GenelazoNo ratings yet
- Incident Reporting Process VisioDocument1 pageIncident Reporting Process Visiopjtx100No ratings yet
- Session Plan Lo2Document4 pagesSession Plan Lo2abegail capistranoNo ratings yet
- Preparation and Modification of High Dietary Fiber FlourDocument12 pagesPreparation and Modification of High Dietary Fiber FlourHuỳnh Như Đặng ThụyNo ratings yet