You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Mental Satus ExaminationDocument5 pagesMental Satus ExaminationP BNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
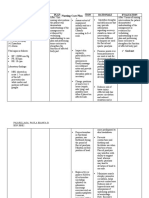
- Nursing Care Plan: Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: IndependentDocument3 pagesNursing Care Plan: Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: IndependentP BNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Ards DSDocument11 pagesArds DSP BNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Penetrating Abdominal Trauma (Stab Wound)Document1 pagePenetrating Abdominal Trauma (Stab Wound)P BNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- DRUG STUDY ClonazepamDocument2 pagesDRUG STUDY ClonazepamP BNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- DRUG STUDY LamotrigineDocument1 pageDRUG STUDY LamotrigineP B0% (2)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Drug StudyDocument3 pagesDrug StudyP BNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Drug StudyDocument7 pagesDrug StudyP BNo ratings yet
- Russian Revolution Revise-TestsDocument7 pagesRussian Revolution Revise-TestsMarga Bendicho Bernal50% (2)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- DR RadhakrishnaDocument74 pagesDR RadhakrishnaChandra ReddyNo ratings yet
- Rekap Pasien Graha INCOVIT Minggu, 08 Agustus 2021Document25 pagesRekap Pasien Graha INCOVIT Minggu, 08 Agustus 2021Muhammad BilalNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Business Proposal FormatDocument15 pagesBusiness Proposal Formatroger policarpioNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- BCT 2019 2020Document356 pagesBCT 2019 2020alam123456No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Hamlet Revision NotesDocument21 pagesHamlet Revision NotesCherrie JohnstnNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Poe Llamanzares Vs Comelec Case DigestDocument4 pagesPoe Llamanzares Vs Comelec Case DigestCess Lamsin100% (3)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Module 12 - Regulatory Bodies For Banks and Non - Bank Financial InstitutionsDocument5 pagesModule 12 - Regulatory Bodies For Banks and Non - Bank Financial InstitutionsMarjon DimafilisNo ratings yet
- Ricalde vs. PeopleDocument14 pagesRicalde vs. PeopleRomy Ian LimNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Pakistan Studies - Affairs - Most Important MCQs (Set III) For CSS, PMS, PCS, NTSDocument9 pagesPakistan Studies - Affairs - Most Important MCQs (Set III) For CSS, PMS, PCS, NTSJatoi AkhtarNo ratings yet
- Zoomcar Tncs 04 03 22Document7 pagesZoomcar Tncs 04 03 22Watch WebseriesNo ratings yet
- Defining A Partnership - The Traditional Approach Versus An InnovaDocument43 pagesDefining A Partnership - The Traditional Approach Versus An Innovajjaye5500No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- EIL AC UPS SpecificaitonDocument465 pagesEIL AC UPS SpecificaitonRitaban R. BanerjeeNo ratings yet
- Model / Modello: WL432Document2 pagesModel / Modello: WL432Wilson HerreraNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- 5.missing File CIC - DS - A - 2013 - 001788-SA - M - 138483Document9 pages5.missing File CIC - DS - A - 2013 - 001788-SA - M - 138483callcenjobsNo ratings yet
- Critical ReasoningDocument3 pagesCritical ReasoningVenkat KrishnaNo ratings yet
- Hagiography and The Cult of Saints in The Diocese of Liège, C. 700-980Document276 pagesHagiography and The Cult of Saints in The Diocese of Liège, C. 700-980Gerardo LarghiNo ratings yet
- 626960PUB0v20B0iesClimateChangeVol2 PDFDocument845 pages626960PUB0v20B0iesClimateChangeVol2 PDFEvelyn MachadoNo ratings yet
- Angels Hadith - Full PaperDocument25 pagesAngels Hadith - Full PaperSouad El MouqtassirNo ratings yet
- Artificial Intelligence Human Flourishing and The Rule of LawDocument6 pagesArtificial Intelligence Human Flourishing and The Rule of LawAinaa KhaleesyaNo ratings yet
- Mabo Study NotesDocument10 pagesMabo Study NotesAaronNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Executive Summary Garden Vista E-VersionDocument1 pageExecutive Summary Garden Vista E-VersionNdank SutrisnoNo ratings yet
- F7-2015-Past Exam - June 2015Document15 pagesF7-2015-Past Exam - June 2015Yulia Melentii0% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Alexandra L. FlottoDocument3 pagesAlexandra L. FlottoAlexandra FlottoNo ratings yet
- Why Do Youth Join Gangs?Document9 pagesWhy Do Youth Join Gangs?Alexandra KeresztesNo ratings yet
- Rizal'S Life, Works & Writings - First Homecoming, 1887-88Document22 pagesRizal'S Life, Works & Writings - First Homecoming, 1887-88Julius de la CruzNo ratings yet
- Raad M. Hassan 305347Document4 pagesRaad M. Hassan 305347Texas WatchdogNo ratings yet
- Asian Filipino Moral Character and Values UpdatedDocument32 pagesAsian Filipino Moral Character and Values UpdatedJames CancinoNo ratings yet
- Getting Started With Bug Bounty PDFDocument15 pagesGetting Started With Bug Bounty PDFmojoxeNo ratings yet
- Sandia Remote Sensing E-MagazineDocument7 pagesSandia Remote Sensing E-Magazinesandia_docsNo ratings yet