You might also like
- How Social Workers Reflect in Action and When and Why (Europa)Document14 pagesHow Social Workers Reflect in Action and When and Why (Europa)Muzak Para RanasNo ratings yet
- Reshaping Theory in Contemporary Social Work: Toward a Critical Pluralism in Clinical PracticeFrom EverandReshaping Theory in Contemporary Social Work: Toward a Critical Pluralism in Clinical PracticeNo ratings yet
- Unit 2 PDFDocument11 pagesUnit 2 PDFEst 19xxNo ratings yet
- Rethinking Professional Practise Ethics of Care Social ConstructinsmDocument31 pagesRethinking Professional Practise Ethics of Care Social ConstructinsmKiss AnnaNo ratings yet
- Hao Jiao (2011) A Conceptual Model For Social Entrepreneurship Directed Toward Social Impact On SocietyDocument21 pagesHao Jiao (2011) A Conceptual Model For Social Entrepreneurship Directed Toward Social Impact On SocietyCarlos Eduardo VargasNo ratings yet
- Virkkunen and Schaupp 2011 From Change To DevelopmentDocument28 pagesVirkkunen and Schaupp 2011 From Change To DevelopmentAdriane CenciNo ratings yet
- Everyday Ethics in Professional Life: Social Work As Ethics WorkDocument20 pagesEveryday Ethics in Professional Life: Social Work As Ethics WorkMuhammad Danish FahimNo ratings yet
- Participatory Action Research Issues in Theory and Practice (Article Accès Libre)Document26 pagesParticipatory Action Research Issues in Theory and Practice (Article Accès Libre)fleurdhiver13No ratings yet
- Importance of Research in Social Work PR PDFDocument10 pagesImportance of Research in Social Work PR PDFNoor FatasyaNo ratings yet
- Art LIN-HU WorkaholicDocument17 pagesArt LIN-HU Workaholicrosegoncalves27No ratings yet
- Social Loafing: A Meta-Analytic Review and Theoretical IntegrationDocument26 pagesSocial Loafing: A Meta-Analytic Review and Theoretical Integrationjerald james montgomeryNo ratings yet
- Values, Practice and Meaning in Social Work ResearchDocument17 pagesValues, Practice and Meaning in Social Work ResearchNurjehan A. DimacangunNo ratings yet
- BR J Soc Work 2006 Taylor 189 206Document18 pagesBR J Soc Work 2006 Taylor 189 206jerri00009No ratings yet
- Coghlan, D. (Annals, 2011) - Action Research Exploring Perspectives On A Philosophy of Practical KnowingDocument36 pagesCoghlan, D. (Annals, 2011) - Action Research Exploring Perspectives On A Philosophy of Practical KnowingMurat Karabulut100% (1)
- Burns SimilaritiesDifferencesCasework 1963Document14 pagesBurns SimilaritiesDifferencesCasework 1963voltronid06No ratings yet
- Atkinson 1982Document33 pagesAtkinson 1982Aditi GhoshNo ratings yet
- Social Work With Individuals: Social Diagnosis and Treatment of Psycho-Social ProblemsDocument11 pagesSocial Work With Individuals: Social Diagnosis and Treatment of Psycho-Social ProblemsMohd ShakilNo ratings yet
- Cambio SocialDocument15 pagesCambio SocialJesseniaNo ratings yet
- Disrupting Hegemony in Social Work Doctoral Education and ResearchDocument17 pagesDisrupting Hegemony in Social Work Doctoral Education and ResearchKaterine Henriquez CamposNo ratings yet
- Boltanski in SSI 1983Document26 pagesBoltanski in SSI 1983Sebastián MuñozNo ratings yet
- Group Work With Children Youth PDFDocument11 pagesGroup Work With Children Youth PDFPUNZALAN, Philip Julian L.No ratings yet
- Importance of Research in Social Work Pr-pages-DeletedDocument8 pagesImportance of Research in Social Work Pr-pages-DeletedAnirban GoswamiNo ratings yet
- Participatory Action Research Issues in Theory and PracticeDocument26 pagesParticipatory Action Research Issues in Theory and PracticeEdgar VesgaNo ratings yet
- Sociology of Labour and Human Resource Management: An Interdisciplinary ApproachDocument9 pagesSociology of Labour and Human Resource Management: An Interdisciplinary Approachking bestNo ratings yet
- Social Innovation: Intuition, Precept, Concept, Theory and PracticeDocument13 pagesSocial Innovation: Intuition, Precept, Concept, Theory and PracticeJonatan BautistaNo ratings yet
- 6 - 2019 - Theory-Social Work Methods-Participation - LubDocument17 pages6 - 2019 - Theory-Social Work Methods-Participation - LubMaria Camila Lopez CastellanosNo ratings yet
- Group Work Practice to Advance Social Competence: A Specialized Methodology for Social WorkFrom EverandGroup Work Practice to Advance Social Competence: A Specialized Methodology for Social WorkNo ratings yet
- 13 Roscoe Carson Madoc-Jones Narrative Social Work. Conversations Between Theory and Practice PDFDocument17 pages13 Roscoe Carson Madoc-Jones Narrative Social Work. Conversations Between Theory and Practice PDFMateo MateitoNo ratings yet
- Ijiset V4 I10 02Document11 pagesIjiset V4 I10 02Nikhil DwivediNo ratings yet
- CH 28092 Social Teater PDFDocument25 pagesCH 28092 Social Teater PDFFarhanNo ratings yet
- Perspectives on Social Group Work PracticeFrom EverandPerspectives on Social Group Work PracticeRating: 5 out of 5 stars5/5 (1)
- BradburyDocument21 pagesBradburyadambayNo ratings yet
- Briggs - ArticleDocument11 pagesBriggs - ArticleJade IsmailNo ratings yet
- Analysing The Temporal Organization of Daily LifeDocument21 pagesAnalysing The Temporal Organization of Daily LifesilvapaNo ratings yet
- A Historical Perspective On The FutureDocument4 pagesA Historical Perspective On The FutureGina GiNo ratings yet
- Reissner Pagan 2013 PreproofDocument38 pagesReissner Pagan 2013 PreproofNasrullah Khan AbidNo ratings yet
- Goldspink & Kay, 2007 PDFDocument15 pagesGoldspink & Kay, 2007 PDFPantelis TsavalasNo ratings yet
- Evidence-based Practice – Modernising the Knowledge Base of Social Work?From EverandEvidence-based Practice – Modernising the Knowledge Base of Social Work?No ratings yet
- Social Work As ScienceDocument11 pagesSocial Work As Sciencerosemariegalindo70No ratings yet
- Epistemology and Social Work: Enhancing The Integration of Theory, Practice and Research Through Philosophical PragmatismDocument12 pagesEpistemology and Social Work: Enhancing The Integration of Theory, Practice and Research Through Philosophical PragmatismMuhammad zahirNo ratings yet
- Research MaterialsDocument31 pagesResearch MaterialsJe CoNo ratings yet
- Wilfred Carr - Critical Action Research TodayDocument13 pagesWilfred Carr - Critical Action Research TodayNádia MartinsNo ratings yet
- Careers in BusinessDocument6 pagesCareers in BusinessHounaida JlassiNo ratings yet
- Villacanas de Castro Banegas ORE 2020 Philosophical Tenets of Action ResearchDocument53 pagesVillacanas de Castro Banegas ORE 2020 Philosophical Tenets of Action ResearchHa YatNo ratings yet
- Paper-4 Social Work Research and Statistics: UNIT-1Document292 pagesPaper-4 Social Work Research and Statistics: UNIT-1Rajesh RoyalsNo ratings yet
- Diagrammatic Assessment of Family RelationshipsDocument12 pagesDiagrammatic Assessment of Family RelationshipsNicholas BoonNo ratings yet
- Sociomaterial Practices: Exploring Technology at Work: EssaiDocument14 pagesSociomaterial Practices: Exploring Technology at Work: Essaiyz2104382No ratings yet
- Demonstrations of The Activity Theory Framework For Research in Information SystemsDocument21 pagesDemonstrations of The Activity Theory Framework For Research in Information SystemsClaudia ElenaNo ratings yet
- Theory & Model-Building in Social Work, A Course SyllabusDocument17 pagesTheory & Model-Building in Social Work, A Course SyllabusJane Gilgun100% (3)
- Katz Busy Bodies 2000Document18 pagesKatz Busy Bodies 2000Alexei70No ratings yet
- Grounded Theory Research MethodsDocument13 pagesGrounded Theory Research MethodsArturo CostaNo ratings yet
- Course: Chapter 1, Lesson 1Document51 pagesCourse: Chapter 1, Lesson 1Carmz PeraltaNo ratings yet
- Smeeton o Connor 2019 Embodied Social Work Practice Within Risk SocietyDocument19 pagesSmeeton o Connor 2019 Embodied Social Work Practice Within Risk SocietyWildan Habibi'98No ratings yet
- Reflexivity LitreviewDocument19 pagesReflexivity LitreviewSarithNo ratings yet
- Affilia: Incorporating Spirituality in Feminist Social Work PerspectivesDocument20 pagesAffilia: Incorporating Spirituality in Feminist Social Work Perspectivesklau0dee0deeNo ratings yet
- Carey - Social Work IdeologieDocument20 pagesCarey - Social Work IdeologieWladimir Mauricio Luque ToroNo ratings yet
- Social Psychology: Student's NameDocument8 pagesSocial Psychology: Student's NameHaseeb AshrafNo ratings yet
- DES221 Social Change PowerPointDocument69 pagesDES221 Social Change PowerPointPastor-Oshatoba Femi Jedidiah0% (1)
- Inscaping: Exploring The Connection Between Experiential Surfacing and Social InnovationDocument11 pagesInscaping: Exploring The Connection Between Experiential Surfacing and Social InnovationNesta100% (1)
- Content ServerDocument15 pagesContent ServerBarbara muñozNo ratings yet
- Diagnoгaă Iăinterven Iaăstructural Ă Înăcaгulăfamiliilor Temporar DezintegrateDocument9 pagesDiagnoгaă Iăinterven Iaăstructural Ă Înăcaгulăfamiliilor Temporar DezintegrateAnna MaryaNo ratings yet
- Linearity vs. Circularity? On Some Common Misconceptions On The Differences in The Research Process in Qualitative and Quantitative ResearchDocument15 pagesLinearity vs. Circularity? On Some Common Misconceptions On The Differences in The Research Process in Qualitative and Quantitative ResearchAnna MaryaNo ratings yet
- Murray - Effects of Parental Imprisonment On Child Antisocial Behaviour and Mental Health A Systematic Review - CSRDocument106 pagesMurray - Effects of Parental Imprisonment On Child Antisocial Behaviour and Mental Health A Systematic Review - CSRAnna MaryaNo ratings yet
- Cover Sheet: Campbell Collaboration Review ProtocolDocument13 pagesCover Sheet: Campbell Collaboration Review ProtocolAnna MaryaNo ratings yet
- Mann Alapter Bertolote Et Al - Suicide Prevention Strategies-Systematic ReviewDocument12 pagesMann Alapter Bertolote Et Al - Suicide Prevention Strategies-Systematic ReviewAnna MaryaNo ratings yet
- Wilson - Dropout - Protocol - CSRDocument35 pagesWilson - Dropout - Protocol - CSRAnna MaryaNo ratings yet
- Littell - Multisystemic Therapy For Social, Emotional, and Behavioral Problems in Youth Aged 10-17 - CSRDocument63 pagesLittell - Multisystemic Therapy For Social, Emotional, and Behavioral Problems in Youth Aged 10-17 - CSRAnna MaryaNo ratings yet
- Work Programmes For Welfare Recipients (Protocol)Document13 pagesWork Programmes For Welfare Recipients (Protocol)Anna MaryaNo ratings yet
- Lucas - Financial Benefits For Child Health and Well-Being in Low Income or Socially Disadvantaged Families in Developed World Countries - CSRDocument96 pagesLucas - Financial Benefits For Child Health and Well-Being in Low Income or Socially Disadvantaged Families in Developed World Countries - CSRAnna MaryaNo ratings yet
- Garrido - Serious (Violent or Chronic) Juvenile Offenders A Systematic Review of Treatment Effectiveness in Secure Corrections - CSRDocument49 pagesGarrido - Serious (Violent or Chronic) Juvenile Offenders A Systematic Review of Treatment Effectiveness in Secure Corrections - CSRAnna MaryaNo ratings yet
- Course Reader For Chapter IiiDocument33 pagesCourse Reader For Chapter Iiipau baniagaNo ratings yet
- Iso 3675 en PDFDocument6 pagesIso 3675 en PDFGery Arturo Perez AltamarNo ratings yet
- Asphaltene Eng2020Document4 pagesAsphaltene Eng2020Elprince MidoNo ratings yet
- Why Facts Don't Change Our MindsDocument13 pagesWhy Facts Don't Change Our MindsNadia Sei LaNo ratings yet
- 8th Chemical Effects of Electric Current Solved QuestionsDocument3 pages8th Chemical Effects of Electric Current Solved QuestionsGururaj KulkarniNo ratings yet
- 4.0 Air Separators 4.1Document31 pages4.0 Air Separators 4.1Dilnesa Ejigu100% (1)
- Technical DescriptionDocument6 pagesTechnical DescriptionJigar MehtaNo ratings yet
- Earth and Life Science LAS UpdatedDocument7 pagesEarth and Life Science LAS UpdatedAnthony HawNo ratings yet
- Tanner EDA Tools v16.3 Release NotesDocument60 pagesTanner EDA Tools v16.3 Release NotesMohiuddin Mohammad100% (1)
- Hi Fi Audio Tone Control Circuit Using Low Noise TransistorsDocument8 pagesHi Fi Audio Tone Control Circuit Using Low Noise TransistorsMuhammad YousafNo ratings yet
- HOSTILE - Colony Module Schematics (Updated)Document18 pagesHOSTILE - Colony Module Schematics (Updated)Oleksandr TrifanNo ratings yet
- Goal SeekDocument7 pagesGoal SeekdNo ratings yet
- British Cost Accounting 1887-1952 PreviewDocument27 pagesBritish Cost Accounting 1887-1952 PreviewJessica JessNo ratings yet
- Display VFD48-1202FN Analog Style - Arduino Project HubDocument27 pagesDisplay VFD48-1202FN Analog Style - Arduino Project HubPhops FrealNo ratings yet
- Punjab Medical Faculty Registration Form: Personal DetailsDocument2 pagesPunjab Medical Faculty Registration Form: Personal DetailsAamir Khan PtiNo ratings yet
- Ampd Data Sheet Vacuum Casting Resin 8263Document2 pagesAmpd Data Sheet Vacuum Casting Resin 8263Lorenzo Guida0% (1)
- Literature & MedicineDocument14 pagesLiterature & MedicineJoyce LeungNo ratings yet
- Term SymbolDocument20 pagesTerm SymbolRirin Zarlina100% (1)
- ECE - 1551 Digital Logic Lecture 15: Combinational Circuits: Assistant Prof. Fareena SaqibDocument19 pagesECE - 1551 Digital Logic Lecture 15: Combinational Circuits: Assistant Prof. Fareena SaqibAll aboutNo ratings yet
- Crushing and Screening Equipment Handbook (Low Res)Document46 pagesCrushing and Screening Equipment Handbook (Low Res)Jayesh NairNo ratings yet
- How To Disassemble Dell Inspiron 17R N7110 - Inside My LaptopDocument17 pagesHow To Disassemble Dell Inspiron 17R N7110 - Inside My LaptopAleksandar AntonijevicNo ratings yet
- 15 TribonDocument10 pages15 Tribonlequanghung98No ratings yet
- Prasna Marga Part I, NotesDocument8 pagesPrasna Marga Part I, NotesSaurav ChakrabortyNo ratings yet
- The Differences Between OHS Management System StandardsDocument27 pagesThe Differences Between OHS Management System StandardsRommel100% (2)
- Middle East Product Booklet 5078 NOV18Document56 pagesMiddle East Product Booklet 5078 NOV18Mohamed987No ratings yet
- A User Guide For FORTRAN 90-95-0Document19 pagesA User Guide For FORTRAN 90-95-0Anonymous IF3H0X2vBeNo ratings yet
- The Awakening Study Guide AnswersDocument24 pagesThe Awakening Study Guide AnswersAli RidhaNo ratings yet
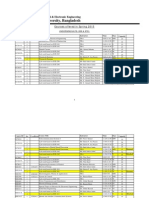
- Courses Offered in Spring 2015Document3 pagesCourses Offered in Spring 2015Mohammed Afzal AsifNo ratings yet
- The Future of Humanity ProjectDocument8 pagesThe Future of Humanity Projectapi-563597519No ratings yet
- Aras Jung Curriculum IndividualDocument72 pagesAras Jung Curriculum IndividualdianavaleriaalvarezNo ratings yet