You might also like
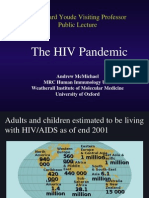
- The HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureDocument50 pagesThe HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureSanthosh SubramanianNo ratings yet
- Opportunistic InfectionsDocument88 pagesOpportunistic InfectionszamadulaNo ratings yet
- AIDS Project (Bios 328)Document36 pagesAIDS Project (Bios 328)tammdocNo ratings yet
- HivDocument29 pagesHivSUTHAN100% (2)
- Fusion Inhibitor and Immunomodulator AbDocument18 pagesFusion Inhibitor and Immunomodulator AbMutiaraa Sarii DewiiNo ratings yet
- HIV Replicação e PatogeneseDocument33 pagesHIV Replicação e Patogenesejose ribamar borges mendesNo ratings yet
- Serology Chapter 24 WorksheetDocument3 pagesSerology Chapter 24 WorksheetRikkiNo ratings yet
- HIV. ASCP. Note YAWDocument80 pagesHIV. ASCP. Note YAWDaroo D.TNo ratings yet
- HIV InfectionDocument47 pagesHIV InfectionMarwanNo ratings yet
- HIV and Related InfectionsDocument50 pagesHIV and Related InfectionsHassan.shehriNo ratings yet
- Chapter X HivDocument52 pagesChapter X HivD PharmaNo ratings yet
- HivDocument49 pagesHivPriyanka GuptaNo ratings yet
- HIV DISEASE - Physiotherapy ClassDocument32 pagesHIV DISEASE - Physiotherapy ClassPraveen RajNo ratings yet
- HIV and AIDS Myths, Facts, and The FutureDocument6 pagesHIV and AIDS Myths, Facts, and The FuturehendoramuNo ratings yet
- Acquired Immuno-Deficiency Syndrome (AIDS) : Savitha R S JSSCP, MysoreDocument41 pagesAcquired Immuno-Deficiency Syndrome (AIDS) : Savitha R S JSSCP, MysorerathanNo ratings yet
- Presentation - AIDSDocument14 pagesPresentation - AIDSPuguNo ratings yet
- Hiv/Aids Seminar: September, 2011Document45 pagesHiv/Aids Seminar: September, 2011Diress MollaNo ratings yet
- FinalDocument42 pagesFinalVizhiNo ratings yet
- HIV&HepatitisDocument100 pagesHIV&HepatitisRaja RuzannaNo ratings yet
- Hiv Vaccines: Presenter: Natasha SawhneyDocument37 pagesHiv Vaccines: Presenter: Natasha SawhneyDR VARSHA A SINGHNo ratings yet
- Chapter 6 - Immune Diseases (Part II) (Robbins and Cotran Pathologic Basis of Disease)Document3 pagesChapter 6 - Immune Diseases (Part II) (Robbins and Cotran Pathologic Basis of Disease)Ernie G. Bautista II, RN, MD100% (5)
- Hivss2019 Paredes R. Intro To Pathophysiology of HivDocument65 pagesHivss2019 Paredes R. Intro To Pathophysiology of Hivjhonny12321No ratings yet
- Lec 6Document32 pagesLec 6Ghadi AbdalazizNo ratings yet
- Human Immunodeficiency VirusDocument15 pagesHuman Immunodeficiency VirusSarah PavuNo ratings yet
- Is HivDocument50 pagesIs HivRodriguez, Jhe-ann M.No ratings yet
- Presented By: DR - Biswajeeta Saha (1 Yr PG) Moderator: Dr. N. Sahu, Dept of Pathology, Kims, BBSRDocument43 pagesPresented By: DR - Biswajeeta Saha (1 Yr PG) Moderator: Dr. N. Sahu, Dept of Pathology, Kims, BBSRBiswajeeta SahaNo ratings yet
- 7-Human Immunodeficiency Virus (HIV)Document6 pages7-Human Immunodeficiency Virus (HIV)TᕼE FᗩᗪEᗪ ᔕOᑌᒪNo ratings yet
- Aids With CMVDocument8 pagesAids With CMVIchunx MelissaNo ratings yet
- Molecular Virology of HIV-1 and Current Antiviral StrategiesDocument7 pagesMolecular Virology of HIV-1 and Current Antiviral StrategiesDitha FadhilaNo ratings yet
- Disusun Oleh: Dr. H. Deddy HartantoDocument63 pagesDisusun Oleh: Dr. H. Deddy HartantoAnonymous UbA0ZHCKeNo ratings yet
- PREP ICU 2013 Answers and Critiques - 1 - Jan & FebDocument47 pagesPREP ICU 2013 Answers and Critiques - 1 - Jan & FebNicholasHuffNo ratings yet
- AIDSDocument32 pagesAIDSJuwairia tariqNo ratings yet
- Retrovirus: Medical Virology Dr. Saif AL-MayahDocument11 pagesRetrovirus: Medical Virology Dr. Saif AL-MayahAtheer AlabdyNo ratings yet
- GVHDDocument35 pagesGVHDSaad KhanNo ratings yet
- Aids and Immunodeficiencies: - Kiruthika ManivannanDocument35 pagesAids and Immunodeficiencies: - Kiruthika ManivannanrevaishNo ratings yet
- GVHDDocument35 pagesGVHDSaad KhanNo ratings yet
- Immunology 8Document37 pagesImmunology 8ukashazam19No ratings yet
- Sem1P1 (41-60)Document19 pagesSem1P1 (41-60)Thom TimkangNo ratings yet
- Clinical Tract: Module OnDocument12 pagesClinical Tract: Module Onpschileshe9472100% (1)
- (17b) RetroviridaeDocument50 pages(17b) RetroviridaeFarrah BenoitNo ratings yet
- Immunodeficiency DisordersDocument8 pagesImmunodeficiency Disordersbpt2No ratings yet
- Immune Response To HIVDocument9 pagesImmune Response To HIVTugas HeinzNo ratings yet
- Nomenclature of Virus ProteinsDocument11 pagesNomenclature of Virus ProteinslkokodkodNo ratings yet
- Biomarkers in SepsisDocument33 pagesBiomarkers in SepsisAnjana KsNo ratings yet
- Virology of Human Immunodeficiency VirusDocument13 pagesVirology of Human Immunodeficiency Virusemmanuelnwa943No ratings yet
- Human Immuno Deficiency VirusDocument15 pagesHuman Immuno Deficiency VirusDayana PrasanthNo ratings yet
- Meyer 2015Document5 pagesMeyer 2015Nasrin Akther ShopnaNo ratings yet
- Epstein-Barr Virus Super FinalDocument6 pagesEpstein-Barr Virus Super FinalStill DollNo ratings yet
- Lymphopenia in COVIDDocument6 pagesLymphopenia in COVIDcitra dewiNo ratings yet
- Google 5Document35 pagesGoogle 5VizhiNo ratings yet
- Coreb Anrs Mie 19042021 Clinic PathophysiolDocument52 pagesCoreb Anrs Mie 19042021 Clinic PathophysiolstephNo ratings yet
- DR - Dr.efrida Warganegara, M.Kes., SP - MKDocument30 pagesDR - Dr.efrida Warganegara, M.Kes., SP - MKDedy SantosoNo ratings yet
- 1 s2.0 S0749070421000981 MainDocument11 pages1 s2.0 S0749070421000981 MainEliseu AmaralNo ratings yet
- MISC - Multisystem Inflammatory Syndrome in in Children (An Unfortunate COVID 19 Aftermath in Children) - DR Akshay P Jadhav MD Pediatrics Fellow PED ICU Fellow Ped EmergencyDocument62 pagesMISC - Multisystem Inflammatory Syndrome in in Children (An Unfortunate COVID 19 Aftermath in Children) - DR Akshay P Jadhav MD Pediatrics Fellow PED ICU Fellow Ped EmergencyDr Akshay P JadhavNo ratings yet
- HIV Life Cycle: Scott M. Hammer, M.DDocument7 pagesHIV Life Cycle: Scott M. Hammer, M.DMohammad SalemyNo ratings yet
- HIV-AIDS NewDocument30 pagesHIV-AIDS NewTri UmianaNo ratings yet
- Kendall A Smith: To Cure Chronic HIV Infection, A New Therapeutic Strategy Is NeededDocument8 pagesKendall A Smith: To Cure Chronic HIV Infection, A New Therapeutic Strategy Is NeededFrontiersNo ratings yet
- Acquired Immunodeficiency Syndrome (AIDS)Document48 pagesAcquired Immunodeficiency Syndrome (AIDS)Muhammad RidwanNo ratings yet
- Hiv AidsDocument52 pagesHiv AidsRivera CharmaineNo ratings yet
- Section 2 Aerobic Gram Positive Bacilli: Susceptibility Manual MB 0810.08Document29 pagesSection 2 Aerobic Gram Positive Bacilli: Susceptibility Manual MB 0810.08Ahmed Goma'aNo ratings yet
- Gram Negative Bacilli Non FermentiveDocument62 pagesGram Negative Bacilli Non FermentiveAhmed Goma'aNo ratings yet
- Section 6 Anaerobes: IH MicrobiologyDocument27 pagesSection 6 Anaerobes: IH MicrobiologyAhmed Goma'aNo ratings yet
- Section 5 Fastidious/Miscellaneous Gram Negative Bacilli/Cocci/CoccobacilliDocument36 pagesSection 5 Fastidious/Miscellaneous Gram Negative Bacilli/Cocci/CoccobacilliAhmed Goma'aNo ratings yet
- Gram Negative BacilliDocument92 pagesGram Negative BacilliAhmed Goma'aNo ratings yet
- Ab Ag RX (Agglut&Precipit)Document16 pagesAb Ag RX (Agglut&Precipit)Ahmed Goma'aNo ratings yet
- HIV Testing in England 2017 ReportDocument57 pagesHIV Testing in England 2017 ReportAhmed Goma'aNo ratings yet
- Tumor Immunology: Teaching ObjectivesDocument5 pagesTumor Immunology: Teaching ObjectivesAhmed Goma'aNo ratings yet
- 07cytokines and ImmunoregulationDocument6 pages07cytokines and ImmunoregulationAhmed Goma'aNo ratings yet
- ApoptosisDocument41 pagesApoptosisZeshan Haider KazmiNo ratings yet
- 07cell Cell InteractionsDocument9 pages07cell Cell InteractionsAhmed Goma'aNo ratings yet
- Quality Assurance in Bacteriology and Immunology 2002Document203 pagesQuality Assurance in Bacteriology and Immunology 2002Ahmed Goma'aNo ratings yet
- ART Threaded Fastener Design and AnalysisDocument40 pagesART Threaded Fastener Design and AnalysisAarón Escorza MistránNo ratings yet
- Tutorial 2 EtherchannelDocument3 pagesTutorial 2 EtherchannelOng CHNo ratings yet
- The Positive and Negative Impact of Inclusive LeadershipDocument9 pagesThe Positive and Negative Impact of Inclusive LeadershipAmbreen ZainebNo ratings yet
- Alternative Refrigerants Manny A PresentationDocument29 pagesAlternative Refrigerants Manny A PresentationEmmanuel Zr Dela CruzNo ratings yet
- Final Year Project Edi IrawanDocument75 pagesFinal Year Project Edi IrawanEdi IrawanNo ratings yet
- EPB2.4 + V3f20 Installation - Start-Up ProcDocument30 pagesEPB2.4 + V3f20 Installation - Start-Up ProcBeltran Héctor75% (4)
- National Institute of Industrial Engineering: Part - B (10 Marks) : Answer All The QuestionsDocument4 pagesNational Institute of Industrial Engineering: Part - B (10 Marks) : Answer All The QuestionsTulasi PatleNo ratings yet
- Dokumen - Tips Dm3220-Servicemanual PDFDocument62 pagesDokumen - Tips Dm3220-Servicemanual PDFwalidsayed1No ratings yet
- 978-0393617542 Research MethodsDocument18 pages978-0393617542 Research MethodsReccebacaNo ratings yet
- Mum LatecityDocument14 pagesMum LatecityGkiniNo ratings yet
- Ictracker Summary of Stocks With Outlook 'Strong Buy' in United StatesDocument12 pagesIctracker Summary of Stocks With Outlook 'Strong Buy' in United StatesBosZ AndersonNo ratings yet
- Mens and Actus ReusDocument3 pagesMens and Actus ReusBrian Okuku OwinohNo ratings yet
- Richard Feynman - The Hierarchy of ComplexityDocument3 pagesRichard Feynman - The Hierarchy of ComplexityjacquesyvescaruanaNo ratings yet
- Pricelist LV Siemens 2019 PDFDocument96 pagesPricelist LV Siemens 2019 PDFBerlianiNo ratings yet
- Stat and Prob Q4 M2 DigitizedDocument38 pagesStat and Prob Q4 M2 Digitizedsecret secretNo ratings yet
- Spsi 622 Page Quattlebaum-Severecommunicationdisorders W Ecolog Inventory ExDocument25 pagesSpsi 622 Page Quattlebaum-Severecommunicationdisorders W Ecolog Inventory Exapi-270949898No ratings yet
- James Bruce, One of Russian Tsar Peter The Great's Key Advisors (1669-1735)Document2 pagesJames Bruce, One of Russian Tsar Peter The Great's Key Advisors (1669-1735)Johanna Granville100% (1)
- معالجات ستاذ يزنDocument11 pagesمعالجات ستاذ يزنammerNo ratings yet
- Organizational Behavior Exam 2 Practice QuestionsDocument1 pageOrganizational Behavior Exam 2 Practice QuestionsSydney EverettNo ratings yet
- The DAMA Guide To The Data Management Body of Knowledge - First EditionDocument430 pagesThe DAMA Guide To The Data Management Body of Knowledge - First Editionkakarotodesu100% (10)
- Kuka Interbus InterfaceDocument11 pagesKuka Interbus InterfaceAnonymous Zh6p3ENo ratings yet
- Tahmina Ferdousy Jhumu: HND Btec Unit 15 Psychology For Health and Social CareDocument29 pagesTahmina Ferdousy Jhumu: HND Btec Unit 15 Psychology For Health and Social CareNabi BoxNo ratings yet
- Om06 JulyaugDocument44 pagesOm06 JulyaugengineeringyusufNo ratings yet
- Securing Your Organization From Modern Ransomware: Ransomware Attacks Are Now A Team EffortDocument11 pagesSecuring Your Organization From Modern Ransomware: Ransomware Attacks Are Now A Team EfforttiagouebemoraisNo ratings yet
- Christina Lauren - The Soulmate EquationDocument4 pagesChristina Lauren - The Soulmate EquationLakshmi SubramanianNo ratings yet
- Music and Yoga Are Complementary To Each OtherDocument9 pagesMusic and Yoga Are Complementary To Each OthersatishNo ratings yet
- UNIABROAD PitchdeckDocument21 pagesUNIABROAD PitchdeckVikas MurulidharaNo ratings yet
- Teacher Survey - Outdoor Classroom Feedback: Please Circle All That ApplyDocument3 pagesTeacher Survey - Outdoor Classroom Feedback: Please Circle All That ApplyBrooke Doran RoeNo ratings yet
- Chemistry Bridging Course Lecture NotesDocument3 pagesChemistry Bridging Course Lecture NotesNNo ratings yet
- ParaklesisDocument23 pagesParaklesisDiana ObeidNo ratings yet