You might also like
- Topic 2 COPD and AsthmaDocument18 pagesTopic 2 COPD and AsthmaCaitlynNo ratings yet
- NCM 114 Topic 4 Comprehensive Geriatric AssessmentDocument16 pagesNCM 114 Topic 4 Comprehensive Geriatric AssessmentCaitlynNo ratings yet
- I and I Module Infectious DisordersDocument23 pagesI and I Module Infectious DisordersCaitlynNo ratings yet
- Tracheostomy Care: Module DescriptionDocument13 pagesTracheostomy Care: Module DescriptionCaitlynNo ratings yet
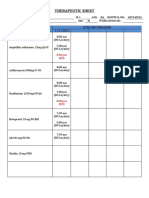
- Therapeutic SheetDocument2 pagesTherapeutic SheetCaitlynNo ratings yet
- Module 2 Ethico-Legal Considerations in Nurisng ResearchDocument6 pagesModule 2 Ethico-Legal Considerations in Nurisng ResearchCaitlynNo ratings yet
- Module 3 Responsibilities of A Beginning Nurse ResearcherDocument9 pagesModule 3 Responsibilities of A Beginning Nurse ResearcherCaitlynNo ratings yet
- Kardex: Mental Status - Conscious Activities Diet Tubes Special InfoDocument6 pagesKardex: Mental Status - Conscious Activities Diet Tubes Special InfoCaitlynNo ratings yet
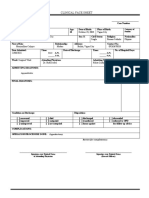
- Clinical Face Sheet: October 23, 2003 Vigan City Single Roman Catholic FilipinoDocument15 pagesClinical Face Sheet: October 23, 2003 Vigan City Single Roman Catholic FilipinoCaitlynNo ratings yet
- Nurses NotesDocument2 pagesNurses NotesCaitlyn100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Family Health Nursing PlanDocument2 pagesFamily Health Nursing PlanGuezil Joy R. DelfinNo ratings yet
- Doctors N Chemist ListDocument19 pagesDoctors N Chemist ListJaggu TigerNo ratings yet
- Healthmedicinet I 2016 5Document282 pagesHealthmedicinet I 2016 5tuni santeNo ratings yet
- Mortality Morbidity and Health Selection Among Met PDFDocument81 pagesMortality Morbidity and Health Selection Among Met PDFLuis EcheverriNo ratings yet
- Test Bank For Lemone and Burkes Medical Surgical Nursing 7th by BauldoffDocument5 pagesTest Bank For Lemone and Burkes Medical Surgical Nursing 7th by Bauldoffcosimalocu68xb1No ratings yet
- Active Fluid De-Resuscitacion in Crtiticalli III Patients Whitj ShockDocument8 pagesActive Fluid De-Resuscitacion in Crtiticalli III Patients Whitj ShockMartha Isabel BurgosNo ratings yet
- Microbiology SyllabusDocument2 pagesMicrobiology Syllabusapi-3704804No ratings yet
- Perioperative Nursing 1Document2 pagesPerioperative Nursing 1Rosie Cuasito100% (2)
- WS 1Q - PHYSICAL EDUCATION With PagesDocument14 pagesWS 1Q - PHYSICAL EDUCATION With PagesJellie Delos ReyesNo ratings yet
- Natasha's Resume WordpressDocument1 pageNatasha's Resume WordpressNatasha Maria CabigonNo ratings yet
- 6 Minute Walk Test ATS GuidelinesDocument7 pages6 Minute Walk Test ATS GuidelinescpradheepNo ratings yet
- NCP PretermDocument5 pagesNCP PretermJamine Joyce Ortega-AlvarezNo ratings yet
- Ankle-Brachial Index-3 PDFDocument9 pagesAnkle-Brachial Index-3 PDFSarah HalanNo ratings yet
- ADA 2020: T2DM Glycemic Goals & Glucose-Lowering GuidelinesDocument10 pagesADA 2020: T2DM Glycemic Goals & Glucose-Lowering GuidelinesLuckybeauty storeNo ratings yet
- Apical Patency - ARTICULO 2Document4 pagesApical Patency - ARTICULO 2Karina Delgado MejíaNo ratings yet
- J. A. D. Anderson - Self-Medication (1979)Document121 pagesJ. A. D. Anderson - Self-Medication (1979)Scoala SolomonaraNo ratings yet
- Reporting in Nursing: By: ImavikeDocument16 pagesReporting in Nursing: By: ImavikererenrahmawatiNo ratings yet
- Bluetongue, Romania: Print CloseDocument2 pagesBluetongue, Romania: Print CloseAnna Maria MurariuNo ratings yet
- Who BG PDFDocument21 pagesWho BG PDFAastha AroraNo ratings yet
- High Risk Newborn2Document15 pagesHigh Risk Newborn2Catherine Villanueva Sta Monica100% (1)
- NN.19.10 Umbilical Cord CareDocument2 pagesNN.19.10 Umbilical Cord CareRohit DwivediNo ratings yet
- Diabetic FootDocument18 pagesDiabetic FootFAMED RESIDENTS CESMEDNo ratings yet
- PROCEDURE On AmniocentesisDocument2 pagesPROCEDURE On AmniocentesisMansiNo ratings yet
- Principles of Continuous Renal Replacement Therapy For AkiDocument43 pagesPrinciples of Continuous Renal Replacement Therapy For AkiFelicia Risca RyandiniNo ratings yet
- Pharmacy Technicians Entry-to-Practice Competency Standards: With Implementation Guide For Competency AssessmentDocument66 pagesPharmacy Technicians Entry-to-Practice Competency Standards: With Implementation Guide For Competency Assessmentokoye geraldNo ratings yet
- Voice Therapy Telepractice, Voice Care For The 21st Century, Towey, 2017Document8 pagesVoice Therapy Telepractice, Voice Care For The 21st Century, Towey, 2017marcela riqueroNo ratings yet
- Medicalization: History and Theory HSSC 532 /HIST 534/SOCI 513Document4 pagesMedicalization: History and Theory HSSC 532 /HIST 534/SOCI 513sofroniscoNo ratings yet
- High-Risk Non-Small Cell Lung Cancer Treated With Active Scanning Proton Beam Radiation Therapy and ImmunotherapyDocument9 pagesHigh-Risk Non-Small Cell Lung Cancer Treated With Active Scanning Proton Beam Radiation Therapy and ImmunotherapyRaul Matute MartinNo ratings yet
- The Future of Imaging in Vet Oncology - Learning From Human MedicineDocument13 pagesThe Future of Imaging in Vet Oncology - Learning From Human MedicineAndra Elena PricopNo ratings yet
- NCP Hyperthermia Related To Underlying InfectionDocument2 pagesNCP Hyperthermia Related To Underlying InfectionNIKKI CARYL ZAFRANo ratings yet