You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Insufficienze Valvolari ESCDocument34 pagesInsufficienze Valvolari ESCAFA.BLSNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Controlling: Cardiac ChaosDocument6 pagesControlling: Cardiac ChaosAFA.BLSNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- HTN e AF Verdecchia-Angeli.117.311402Document17 pagesHTN e AF Verdecchia-Angeli.117.311402AFA.BLSNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Tep EscDocument48 pagesTep EscAFA.BLSNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Goette AtrialcardiomyopatiesDocument36 pagesGoette AtrialcardiomyopatiesAFA.BLSNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- How To Mend A Broken Heart - An Approach To The Failing RV - American College of CardiologyDocument14 pagesHow To Mend A Broken Heart - An Approach To The Failing RV - American College of CardiologyAFA.BLSNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- HTN and Arrh AfzalDocument8 pagesHTN and Arrh AfzalAFA.BLSNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- American Thoracic Society DocumentsDocument29 pagesAmerican Thoracic Society DocumentsAFA.BLSNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- GL Valvole CardiacheDocument49 pagesGL Valvole CardiacheAFA.BLSNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Yellow and Orange in Cutaneous Lesions: Clinical and Dermoscopic DataDocument9 pagesYellow and Orange in Cutaneous Lesions: Clinical and Dermoscopic DataAFA.BLSNo ratings yet
- Management of Acute Exacerbations of Asthma in Adults - UpToDateDocument23 pagesManagement of Acute Exacerbations of Asthma in Adults - UpToDateAFA.BLSNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Basic Life Support (BLS) in Adults - UpToDateDocument11 pagesBasic Life Support (BLS) in Adults - UpToDateAFA.BLSNo ratings yet
- Use of Diuretics in Patients With Heart Failure - UpToDateDocument11 pagesUse of Diuretics in Patients With Heart Failure - UpToDateAFA.BLSNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Glucocorticoid Withdrawal - UpToDateDocument11 pagesGlucocorticoid Withdrawal - UpToDateAFA.BLSNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Copia Di Drugs That Cause or Prolong Delirium - UpToDateDocument2 pagesCopia Di Drugs That Cause or Prolong Delirium - UpToDateAFA.BLSNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Diagnostik Dan Tatalaksana Stable CAD - CCSDocument38 pagesDiagnostik Dan Tatalaksana Stable CAD - CCSIno HajrinNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- 1 s2.0 S2213177917304183 MainDocument9 pages1 s2.0 S2213177917304183 MainAndré DiasNo ratings yet
- ACS DR Rini PramestiDocument52 pagesACS DR Rini PramestiJackSaripantungNo ratings yet
- Left Ventricular Remodeling in Heart FailureDocument11 pagesLeft Ventricular Remodeling in Heart FailureSabrinaAyuPutriNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Pharma - Updated Topical Past Papers 2007-23Document53 pagesPharma - Updated Topical Past Papers 2007-23Tayyab AfzalNo ratings yet
- Medical Surgical Nursing Review 1Document422 pagesMedical Surgical Nursing Review 1jeshemaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
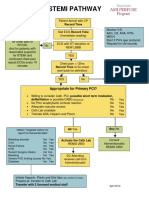
- Stemi Pathway: Record TimeDocument2 pagesStemi Pathway: Record TimeOlga Jadha CasmiraNo ratings yet
- Plab 1 NotesDocument141 pagesPlab 1 Notesthiri sakura100% (3)
- Susan G. Salvo - Mosby's Pathology For Massage Therapists-Mosby (2013)Document557 pagesSusan G. Salvo - Mosby's Pathology For Massage Therapists-Mosby (2013)7ty42yr2v4No ratings yet
- Pharmacotherapeutics - PharmD II YearDocument5 pagesPharmacotherapeutics - PharmD II YearSuresh Thanneru100% (2)
- ExamDocument2 pagesExamcheem_porkeezNo ratings yet
- Examination, Diagnosis and Treatment Planning For Complete Denture TherapyDocument7 pagesExamination, Diagnosis and Treatment Planning For Complete Denture TherapyAmar Bimavarapu100% (1)
- 2541 FullDocument100 pages2541 FullIrina Luciana DumitriuNo ratings yet
- EMT NotesDocument58 pagesEMT NotesJosue PasillasNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Combined Impact of Surgical Team Education and Chlorhexidine 2% Alcohol On The Reduction of Surgical Site Infection Following Cardiac SurgeryDocument7 pagesThe Combined Impact of Surgical Team Education and Chlorhexidine 2% Alcohol On The Reduction of Surgical Site Infection Following Cardiac SurgeryShandaPrimaDewiNo ratings yet
- The Abdominojugular Reflux Sign: Jeff Wiese, MDDocument3 pagesThe Abdominojugular Reflux Sign: Jeff Wiese, MDRed RubyNo ratings yet
- GP Emergency Manual PDFDocument72 pagesGP Emergency Manual PDFRumana Ali100% (2)
- Thesis On Coronary Heart DiseaseDocument7 pagesThesis On Coronary Heart Diseasetracyclarkwarren100% (1)
- Med-Surg Lecture 4th Year 1st Sem (Incomplete)Document70 pagesMed-Surg Lecture 4th Year 1st Sem (Incomplete)Raezhell Dianne RachoNo ratings yet
- Biology - MYP 3 - 31st AugustDocument6 pagesBiology - MYP 3 - 31st Augustarchit.kulkarni7756No ratings yet
- Medical TerminologyDocument107 pagesMedical TerminologyonmcvNo ratings yet
- Copia de EuroSCOREorgPDocument6 pagesCopia de EuroSCOREorgPDiego Andrés Rojas TejadaNo ratings yet
- MetoprololDocument15 pagesMetoprololMahavir SinghNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 50 Nursing Mnemonics and Acronyms You Need To Know NowDocument29 pages50 Nursing Mnemonics and Acronyms You Need To Know Nowtandz100% (19)
- CVD PreventionDocument31 pagesCVD PreventionAhmad AnzariNo ratings yet
- Slaber Jaga Kamis 31 Agustus 2023Document21 pagesSlaber Jaga Kamis 31 Agustus 2023Amil budi JadiNo ratings yet
- Krok2 - Medicine - 2010Document27 pagesKrok2 - Medicine - 2010Badriya YussufNo ratings yet
- MnemonicsDocument9 pagesMnemonicsJhey MalanyaonNo ratings yet
- Prognosis and Outcomes Following Sudden Cardiac Arrest in AdultsDocument24 pagesPrognosis and Outcomes Following Sudden Cardiac Arrest in AdultsAnca StanNo ratings yet
- Discharge PlanningDocument3 pagesDischarge PlanningMaye ArugayNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (5)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (39)