You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Quiz 11 Unit .3 Patricia E. Benner Introduction of Nursing Theory & ModelDocument3 pagesQuiz 11 Unit .3 Patricia E. Benner Introduction of Nursing Theory & ModelZhedriex EspirituNo ratings yet
- Acanthosis Nigricans An Extensive ReviewDocument16 pagesAcanthosis Nigricans An Extensive ReviewFebri Dwi HaryonoNo ratings yet
- Paraneoplastic Syndromes in Small Cell Lung CancerDocument11 pagesParaneoplastic Syndromes in Small Cell Lung CancerFebri Dwi HaryonoNo ratings yet
- 4 EctDocument9 pages4 EctFebri Dwi HaryonoNo ratings yet
- Siadh!!!Document10 pagesSiadh!!!Febri Dwi HaryonoNo ratings yet
- Common Invasive Fungal Diseases An Overview of Invasive Candidiasis, Aspergillosis, Cryptococcosis, and Pneumocystis PneumoniaDocument12 pagesCommon Invasive Fungal Diseases An Overview of Invasive Candidiasis, Aspergillosis, Cryptococcosis, and Pneumocystis PneumoniaFebri Dwi HaryonoNo ratings yet
- Cryptococcal Lung MycosesDocument14 pagesCryptococcal Lung MycosesFebri Dwi HaryonoNo ratings yet
- Clinical Manifestations and Treatment of BlastomycosisDocument15 pagesClinical Manifestations and Treatment of BlastomycosisFebri Dwi HaryonoNo ratings yet
- Hybrid Deep Learning For Detecting Lung Diseases From X-Ray ImagesDocument14 pagesHybrid Deep Learning For Detecting Lung Diseases From X-Ray ImagesMurshedul ArifeenNo ratings yet
- Fimmu 12 606860Document18 pagesFimmu 12 606860Aditya Yudha PratamaNo ratings yet
- Sensorium.: NiirDocument6 pagesSensorium.: NiirSundar RajanNo ratings yet
- Hypertensive Disorders in Pregnancy: Abdallah Al-MawazrehDocument36 pagesHypertensive Disorders in Pregnancy: Abdallah Al-MawazrehAbdallahMousaNo ratings yet
- Effect of Nateglinide On The Incidence of DiabetesDocument31 pagesEffect of Nateglinide On The Incidence of Diabetesfred opinionNo ratings yet
- 1-3 Day 1 - Community As People Community Health NursingDocument11 pages1-3 Day 1 - Community As People Community Health NursingBea Dela CenaNo ratings yet
- School Form 8 SF8 Learner Basic Health and Nutrition ReportDocument10 pagesSchool Form 8 SF8 Learner Basic Health and Nutrition ReportRey Moca100% (1)
- Myelomeningocele: A New Functional Classification: PerspectiveDocument5 pagesMyelomeningocele: A New Functional Classification: PerspectiveLema Ulloa ZoraidaNo ratings yet
- Rescue and Carry Methods Power PointDocument75 pagesRescue and Carry Methods Power PointJean Minette Prado88% (8)
- Novita Tirodatu - 19704001 - Kelas A - Tugas Epidemiologi Kawasan PesisirDocument8 pagesNovita Tirodatu - 19704001 - Kelas A - Tugas Epidemiologi Kawasan PesisirNovita Tirodatu11No ratings yet
- Baloon Tamponade of Gastroesophageal VaricesDocument8 pagesBaloon Tamponade of Gastroesophageal VaricesCecilio MartínNo ratings yet
- Renal 20nutrition 20web 1Document57 pagesRenal 20nutrition 20web 1Qurat ul Ain Arif Sethi Pharmacy PracticeNo ratings yet
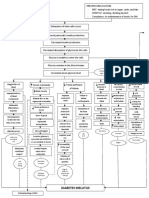
- Diabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)Document3 pagesDiabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)John Henry ValenciaNo ratings yet
- Epilepsy SyndromesDocument13 pagesEpilepsy SyndromestoyyibNo ratings yet
- Bracing ArmageddonDocument224 pagesBracing ArmageddonH AckNo ratings yet
- Neha ShahDocument448 pagesNeha ShahAshima GautamNo ratings yet
- np4 TestDocument8 pagesnp4 TestMargie BalunesNo ratings yet
- Primary Psoas Abscess: Alexandru Crisan, Emilia Nicoara, Karina Bota, Doru BordosDocument3 pagesPrimary Psoas Abscess: Alexandru Crisan, Emilia Nicoara, Karina Bota, Doru BordosNataliaMaedyNo ratings yet
- Spirometry: How To Do The TestDocument4 pagesSpirometry: How To Do The TestMarc AbellaNo ratings yet
- Glaucoma Case StudyDocument5 pagesGlaucoma Case StudyEdgel QuidolesNo ratings yet
- 100 Item MEDICAL SURGICAL Nursing Examination Correct Answers and RationalesDocument27 pages100 Item MEDICAL SURGICAL Nursing Examination Correct Answers and RationaleshezekiahNo ratings yet
- Boone 19e c04 PPTDocument40 pagesBoone 19e c04 PPTJohn RitssNo ratings yet
- Jama Ference 2020 It 200013Document2 pagesJama Ference 2020 It 200013miguelalmenarezNo ratings yet
- Set A: NP1 Nursing Board Exam December 2006 Answer Key 'Foundation of Professional Nursing PracticeDocument14 pagesSet A: NP1 Nursing Board Exam December 2006 Answer Key 'Foundation of Professional Nursing PracticeRaLph C. LopezNo ratings yet
- Health Law BibliographyDocument11 pagesHealth Law BibliographyIeien MuthmainnahNo ratings yet
- Eyelids Slides PDFDocument72 pagesEyelids Slides PDFMariam QaisNo ratings yet
- Running Shoes, Orthotics, and Injuries: D.C. Mckenzie, D.B. Clement J.E. TauntonDocument14 pagesRunning Shoes, Orthotics, and Injuries: D.C. Mckenzie, D.B. Clement J.E. TauntonAriene RibeiroNo ratings yet
- Microbiology - Bio LibretextDocument782 pagesMicrobiology - Bio LibretextJomsEve Ison100% (2)
- Clinical Nursing Skills and Techniques 6th Edition Perry Test BankDocument11 pagesClinical Nursing Skills and Techniques 6th Edition Perry Test BankAnnetteOliverrbwcx100% (12)