You might also like
- MCPS Form For Annual Sports Physical Exam - (PPE) 2010 Edition Prepared by Am Academy of Ped, Am. Academy of Family Phys Et Al.Document5 pagesMCPS Form For Annual Sports Physical Exam - (PPE) 2010 Edition Prepared by Am Academy of Ped, Am. Academy of Family Phys Et Al.Concussion_MCPS_MdNo ratings yet
- Psychiatrics McqsDocument20 pagesPsychiatrics McqsHirwaNo ratings yet
- NCLEX Review Cardiovascular QuizDocument17 pagesNCLEX Review Cardiovascular QuizApple Mesina100% (2)
- Emergency Nursing: By: Keverne Jhay P. ColasDocument61 pagesEmergency Nursing: By: Keverne Jhay P. ColasGaras AnnaBerniceNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Effects of COVID-19 On Parkinson Disease Clinical Features - A CMDocument12 pagesEffects of COVID-19 On Parkinson Disease Clinical Features - A CMAntonyNo ratings yet
- Retinal Findings in Patients COVID19Document1 pageRetinal Findings in Patients COVID19María de Lourdes EspejelNo ratings yet
- Movement Disorders in COVID 19 Times Impact On.9Document8 pagesMovement Disorders in COVID 19 Times Impact On.9Putu AfruriNo ratings yet
- Impact of Diabetes On COVID-19-Releated in Hospital MortalityDocument8 pagesImpact of Diabetes On COVID-19-Releated in Hospital MortalityDaniela VelascoNo ratings yet
- Geriatric Medicine and GerontologyDocument7 pagesGeriatric Medicine and GerontologyNoor FadlanNo ratings yet
- Scab 066Document12 pagesScab 066Djfiory YonutzNo ratings yet
- Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, ChinaDocument7 pagesDysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, Chinacika daraNo ratings yet
- Biomarkers of Ageing and Frailty May Predict COVID-19 SeverityDocument13 pagesBiomarkers of Ageing and Frailty May Predict COVID-19 SeverityPPDS Rehab Medik UnhasNo ratings yet
- Bianchetti 2020Document6 pagesBianchetti 2020GembongSatriaMahardhikaNo ratings yet
- JAPI0200 p19-24 CompressedDocument6 pagesJAPI0200 p19-24 Compressedsachin kulkarniNo ratings yet
- FM, Nueva Faceta Post CovidDocument10 pagesFM, Nueva Faceta Post Covidtavo570No ratings yet
- 2020 - Ajslp 20 00147Document12 pages2020 - Ajslp 20 00147Luis.fernando. GarciaNo ratings yet
- Assessment and Characterisation of post-COVID-19 ManifestationsDocument5 pagesAssessment and Characterisation of post-COVID-19 ManifestationsAlexandra IonițăNo ratings yet
- Therapeutic Efficacy of Ivermectin As An Adjuvant in The Treatment of Patients With COVID-19Document5 pagesTherapeutic Efficacy of Ivermectin As An Adjuvant in The Treatment of Patients With COVID-19International Journal of Innovative Science and Research Technology100% (1)
- Funciones y Actividades Plaquetarias Como Posibles Parámetros Hematológicos Relacionados Con La Enfermedad Por CoronavirusDocument7 pagesFunciones y Actividades Plaquetarias Como Posibles Parámetros Hematológicos Relacionados Con La Enfermedad Por CoronavirusEdinson Cortez VasquezNo ratings yet
- Impact of COVID-19 On Primary Care Visits: Lesson Learnt From The Early Pandemic PeriodDocument10 pagesImpact of COVID-19 On Primary Care Visits: Lesson Learnt From The Early Pandemic PeriodRino RinzNo ratings yet
- Dynamic Interleukin-6 Level Changes As A Prognostic Indicator in Patients With COVID-19Document11 pagesDynamic Interleukin-6 Level Changes As A Prognostic Indicator in Patients With COVID-19dariusNo ratings yet
- Conjunctivitis and COVID 19: A Meta Analysis: LettertotheeditorDocument2 pagesConjunctivitis and COVID 19: A Meta Analysis: LettertotheeditorAngel LimNo ratings yet
- Long COVID Guidelines Need To Reflect Lived Experience: CommentDocument3 pagesLong COVID Guidelines Need To Reflect Lived Experience: CommentAlexandra PimentaNo ratings yet
- Kidney Disease Is Associated With In-Hospital Death of Patients With COVID-19Document10 pagesKidney Disease Is Associated With In-Hospital Death of Patients With COVID-19Kevin OwenNo ratings yet
- Fisiopatologia, Presentación y Abordaje Del Delirium en Covid 19Document16 pagesFisiopatologia, Presentación y Abordaje Del Delirium en Covid 19paola coralNo ratings yet
- Contactless In-Home Monitoring of The Long-Term Respiratory and Behavioral Phenotypes in Older Adults With COVID-19Document8 pagesContactless In-Home Monitoring of The Long-Term Respiratory and Behavioral Phenotypes in Older Adults With COVID-19Sarah Nauman GhaziNo ratings yet
- ECI 9999 E13314Document6 pagesECI 9999 E13314WilsonR.CorzoNiñoNo ratings yet
- Modeling The Onset Syntoms of CovidDocument14 pagesModeling The Onset Syntoms of CovidMiguel R MoNo ratings yet
- Montelukast in COVID-4Document6 pagesMontelukast in COVID-4Golam JILANI Mahbubay AlamNo ratings yet
- Presidential Memorandum On Long-Term Effects of COVID-19Document2 pagesPresidential Memorandum On Long-Term Effects of COVID-19rodriguezdiazNo ratings yet
- COVID-19 Infection and Seropositivity in Multiple Sclerosis Patients in Guilan in 2021Document11 pagesCOVID-19 Infection and Seropositivity in Multiple Sclerosis Patients in Guilan in 2021samaneh shirkouhiNo ratings yet
- COVID-19 Incidence and Mortality in Non-Dialysis Chronic Kidney Disease PatientsDocument11 pagesCOVID-19 Incidence and Mortality in Non-Dialysis Chronic Kidney Disease Patientsblume diaNo ratings yet
- Covid-19-Linked Loss of Smell and Taste - Case Study and DiscussionDocument5 pagesCovid-19-Linked Loss of Smell and Taste - Case Study and DiscussionGalletNo ratings yet
- Jennings Et Al (Dic-2021)Document15 pagesJennings Et Al (Dic-2021)Sergio GarcíaNo ratings yet
- COVID-19 and Smoking: What Evidence Needs Our Attention?Document9 pagesCOVID-19 and Smoking: What Evidence Needs Our Attention?elguyoNo ratings yet
- Fimmu 13 857573Document11 pagesFimmu 13 857573Bruno QueirozNo ratings yet
- COVID-19 and Guillain-Barré Syndrome, A Single-Center Prospective Case Series With A 1-Year Follow-UpDocument8 pagesCOVID-19 and Guillain-Barré Syndrome, A Single-Center Prospective Case Series With A 1-Year Follow-UpLuciano RuizNo ratings yet
- Long Term Neuropsychiatric Consequences in COVID-19 Survivors Cognitive Impairment and Inflammatory Underpinnings Fifteen Months After DischargeDocument8 pagesLong Term Neuropsychiatric Consequences in COVID-19 Survivors Cognitive Impairment and Inflammatory Underpinnings Fifteen Months After DischargeLaura PulidoNo ratings yet
- 2299-Article Text-26374-3-10-20220428Document6 pages2299-Article Text-26374-3-10-20220428anne claire feudoNo ratings yet
- Knowledge and Practice On Covid-19 Among General PublicDocument4 pagesKnowledge and Practice On Covid-19 Among General PublicInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Quadmester-Wise Comparison of Disease Transmission Dynamics of COVID-19 Among Health Care Workers in Kannur District, KeralaDocument7 pagesQuadmester-Wise Comparison of Disease Transmission Dynamics of COVID-19 Among Health Care Workers in Kannur District, KeraladrdeepudentNo ratings yet
- Association of COVID 19 With Diabetes: A Systematic Review and Meta AnalysisDocument8 pagesAssociation of COVID 19 With Diabetes: A Systematic Review and Meta AnalysisAgatha GeraldyneNo ratings yet
- Association of Procalcitonin Levels With The Progression and Prognosis of Hospitalized Patients With COVID-19Document9 pagesAssociation of Procalcitonin Levels With The Progression and Prognosis of Hospitalized Patients With COVID-19Dian Putri NingsihNo ratings yet
- Coronavirus Disease 2019 (COVID-19) : A Perspective From ChinaDocument11 pagesCoronavirus Disease 2019 (COVID-19) : A Perspective From Chinasri karuniaNo ratings yet
- E696 FullDocument10 pagesE696 FullotakualafugaNo ratings yet
- Does Amantadine Have A Protective Effect Against CDocument3 pagesDoes Amantadine Have A Protective Effect Against CAleksandra MarciniakNo ratings yet
- Diabetes and COVID-19 Testing, Positivity, and MortalityDocument6 pagesDiabetes and COVID-19 Testing, Positivity, and MortalityDiana MontoyaNo ratings yet
- International Journal of Infectious Diseases: SciencedirectDocument8 pagesInternational Journal of Infectious Diseases: SciencedirectAntonio Barrios PerezNo ratings yet
- Review: Li Jiang, Kun Tang, Mike Levin, Omar Irfan, Shaun K Morris, Karen Wilson, Jonathan D Klein, Zulfiqar A BhuttaDocument13 pagesReview: Li Jiang, Kun Tang, Mike Levin, Omar Irfan, Shaun K Morris, Karen Wilson, Jonathan D Klein, Zulfiqar A BhuttaMaria Carolina FallaNo ratings yet
- IJGMP - Format-Association Thyroid Function To Prognosis of COVID 19Document8 pagesIJGMP - Format-Association Thyroid Function To Prognosis of COVID 19iaset123No ratings yet
- Neuropsychiatric Symptoms Inelderly With Dementia DuringCOVID-19 PandemicDocument9 pagesNeuropsychiatric Symptoms Inelderly With Dementia DuringCOVID-19 Pandemicmadalena limaNo ratings yet
- Procalcitonin and Secondary Bacterial InfectionsDocument6 pagesProcalcitonin and Secondary Bacterial Infectionsadrifen adriNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument5 pagesDiabetes & Metabolic Syndrome: Clinical Research & ReviewsRea AuliaNo ratings yet
- Bencivenga 2020Document4 pagesBencivenga 2020GembongSatriaMahardhikaNo ratings yet
- 1 s2.0 S0022510X22003495 MainDocument11 pages1 s2.0 S0022510X22003495 MainoscarNo ratings yet
- Predictors of COVID-19 Severity: A Literature ReviewDocument10 pagesPredictors of COVID-19 Severity: A Literature ReviewRafiqua Sifat JahanNo ratings yet
- 2020 - Ajslp 20 00147Document12 pages2020 - Ajslp 20 00147Maha KhanNo ratings yet
- Pengumuman THT-KL 2022Document10 pagesPengumuman THT-KL 2022Citra LyadhaNo ratings yet
- Covid 19 Review PaperDocument25 pagesCovid 19 Review PaperLeena MuniandyNo ratings yet
- The Study of Clinical Profile of Acute Kidney Injury in COVID-19 PatientsDocument6 pagesThe Study of Clinical Profile of Acute Kidney Injury in COVID-19 PatientsbijgimNo ratings yet
- 1 s2.0 S1473309921007039 MainDocument6 pages1 s2.0 S1473309921007039 MainCamilo Andrés CastroNo ratings yet
- METHAMEDICINDocument21 pagesMETHAMEDICINRobert ManriqueNo ratings yet
- Current Prevalence, Characteristics, and Comorbidities of Patients With COVID-19 in IndonesiaDocument8 pagesCurrent Prevalence, Characteristics, and Comorbidities of Patients With COVID-19 in IndonesiaAkreditasi InternaNo ratings yet
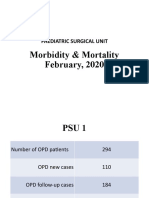
- Morbidity & Mortality (February, 2020)Document14 pagesMorbidity & Mortality (February, 2020)Wai GyiNo ratings yet
- Jake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersDocument8 pagesJake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersJake Yvan DizonNo ratings yet
- Viral Skin InfectionsDocument28 pagesViral Skin Infectionstolesadereje73No ratings yet
- Case Files® EnterococcusDocument4 pagesCase Files® EnterococcusAHMAD ADE SAPUTRANo ratings yet
- Bugnao v. Ubag, GR No. 4445, 18 September 1909Document2 pagesBugnao v. Ubag, GR No. 4445, 18 September 1909Judel MatiasNo ratings yet
- Diseases: July 2021Document246 pagesDiseases: July 2021Mkaruka BrellaNo ratings yet
- Keamanan Pangan Hasil PerikananDocument42 pagesKeamanan Pangan Hasil PerikananBhatara Ayi MeataNo ratings yet
- I. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationDocument3 pagesI. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationCherubim Lei DC FloresNo ratings yet
- Legalizing Marijuana FinalDocument18 pagesLegalizing Marijuana FinalTeresa EvripidouNo ratings yet
- Ann-Charlotte Granholm, David Bachman, Jacobo Mintzer, Kumar SambamurtiDocument2 pagesAnn-Charlotte Granholm, David Bachman, Jacobo Mintzer, Kumar SambamurtiAlexandru TanaseNo ratings yet
- Edu 259 p1 Prof Ed Edu 259 p1 Prof EdDocument92 pagesEdu 259 p1 Prof Ed Edu 259 p1 Prof EdkriztheiaaveriennenievesNo ratings yet
- Medical Emergencies in Oral and Maxillofacial Surgery KHADIJA-5Document81 pagesMedical Emergencies in Oral and Maxillofacial Surgery KHADIJA-5Khadija VasiNo ratings yet
- Bayes' Theorem in Paleopathological Diagnosis PDFDocument9 pagesBayes' Theorem in Paleopathological Diagnosis PDFjessyramirez07No ratings yet
- Lab Final Exam ReviewDocument59 pagesLab Final Exam ReviewManju ShreeNo ratings yet
- Health Facts 2020Document19 pagesHealth Facts 2020haikal11No ratings yet
- J. Dizon vs. Naess Shipping Phils., Inc. G.R. No. 201834 DawisanDocument2 pagesJ. Dizon vs. Naess Shipping Phils., Inc. G.R. No. 201834 DawisanMae Clare BendoNo ratings yet
- Notes On UtiDocument15 pagesNotes On UtiSaleh Mohammad ShoaibNo ratings yet
- Volume 23 Chapter 4 - Supard Race's VillageDocument21 pagesVolume 23 Chapter 4 - Supard Race's VillageCastro CarlosNo ratings yet
- Current Application of Cannabidiol (CBD) in The Management and Treatment of Neurological DisordersDocument14 pagesCurrent Application of Cannabidiol (CBD) in The Management and Treatment of Neurological Disorderssara laadamiNo ratings yet
- Soy2020 Article CytokineStormInCOVID-19PathogeDocument10 pagesSoy2020 Article CytokineStormInCOVID-19PathogeGumoNo ratings yet
- UlcerDocument3 pagesUlcerMd Ahsanuzzaman PinkuNo ratings yet
- Final Project IdeaDocument2 pagesFinal Project IdeaAniqa waheedNo ratings yet
- EDITED 02chapter 1 Aratiles OintmentDocument9 pagesEDITED 02chapter 1 Aratiles OintmentMikhaela Andree MarianoNo ratings yet
- 13463-Article Text-25834-1-10-20210103Document3 pages13463-Article Text-25834-1-10-20210103Melly SyafridaNo ratings yet
- Evolution of MicrobiologyDocument48 pagesEvolution of MicrobiologyArielleNo ratings yet
- Radiological Anatomy of Stomach and Duodenum With Clinical SignificanceDocument9 pagesRadiological Anatomy of Stomach and Duodenum With Clinical SignificancepouchkineNo ratings yet