You might also like
- Simulink SimulationDocument15 pagesSimulink Simulationpoopoopho100% (1)
- Advanced Manufacturing Processes (ALL SLIDES Gaurav Arora)Document259 pagesAdvanced Manufacturing Processes (ALL SLIDES Gaurav Arora)faizNo ratings yet
- Pupalaikis - S Parameters For Signal IntegrityDocument666 pagesPupalaikis - S Parameters For Signal IntegrityzhangwenNo ratings yet
- Lecture 11 Network DesignDocument132 pagesLecture 11 Network Designjon-jon anchetaNo ratings yet
- IT Companies - in MumbaiDocument22 pagesIT Companies - in MumbaiRicky OrtizNo ratings yet
- Clinical Intervention Using Focused Ultrasound (FUS) Stimulation of The Brain in Diverse Neurological Disorders - Fneur-13-880814Document2 pagesClinical Intervention Using Focused Ultrasound (FUS) Stimulation of The Brain in Diverse Neurological Disorders - Fneur-13-880814Generation GenerationNo ratings yet
- Review DBSDocument8 pagesReview DBSEtonia PangNo ratings yet
- Fneur 13 880814Document18 pagesFneur 13 880814Generation GenerationNo ratings yet
- Stereotactic Implantation of Deep BrainDocument28 pagesStereotactic Implantation of Deep Brainberna chuaNo ratings yet
- Abstracts / Brain Stimulation 10 (2017) 346 E540 396Document1 pageAbstracts / Brain Stimulation 10 (2017) 346 E540 396Aleja ToPaNo ratings yet
- Aspectos MetodológicosDocument8 pagesAspectos MetodológicosDaniela AndreottiNo ratings yet
- Art. L Zrinzo - MRI-guided STN DBS in Parkinson's Disease Without Microelectrode Recording Efficacy and SafetyDocument7 pagesArt. L Zrinzo - MRI-guided STN DBS in Parkinson's Disease Without Microelectrode Recording Efficacy and SafetyEstereotaxia BrasilNo ratings yet
- Kwon World Neurosurgery 2016Document4 pagesKwon World Neurosurgery 2016Churl-Su KwonNo ratings yet
- DOR - FENOL - Chemical Ablation of Genicular Nerve With Phenol For Pain Relief in Patients With Knee Osteoarthritis A Prospective Study - CompressedDocument7 pagesDOR - FENOL - Chemical Ablation of Genicular Nerve With Phenol For Pain Relief in Patients With Knee Osteoarthritis A Prospective Study - CompressedGustavo FredericoNo ratings yet
- Pedunculopontine Nucleus Region Deep Brain Stimulation in Parkinson Disease: Surgical Techniques, Side Effects, and Postoperative ImagingDocument13 pagesPedunculopontine Nucleus Region Deep Brain Stimulation in Parkinson Disease: Surgical Techniques, Side Effects, and Postoperative ImagingEstereotaxia BrasilNo ratings yet
- Art. PA Star - Microelectrode-Guided Implantation of Deep Brain Stimulators Into The Globus Pallidus Internus For Dystonia Techniques, Electrode Locations, and OutcomesDocument14 pagesArt. PA Star - Microelectrode-Guided Implantation of Deep Brain Stimulators Into The Globus Pallidus Internus For Dystonia Techniques, Electrode Locations, and OutcomesPaul RodrigoNo ratings yet
- 10 1016@j Clinph 2019 04 615Document2 pages10 1016@j Clinph 2019 04 615danie.arti01No ratings yet
- 2016 2 jns152485Document11 pages2016 2 jns152485MaríaNo ratings yet
- 2015-Accuracy of Subthalamic Nucleus Targeting by T2, FLAIRDocument8 pages2015-Accuracy of Subthalamic Nucleus Targeting by T2, FLAIRPaul RodrigoNo ratings yet
- 1933 0693 Article p1372Document8 pages1933 0693 Article p1372florin jescuNo ratings yet
- JurnalkuDocument5 pagesJurnalkuAgis CliquersNo ratings yet
- Ene 14885Document12 pagesEne 14885mikeNo ratings yet
- Nikken MX2R Device, Pulsed Magnetic Field Therapy in Refractory CarpalDocument6 pagesNikken MX2R Device, Pulsed Magnetic Field Therapy in Refractory CarpalgstrohlNo ratings yet
- Brain EdemaDocument15 pagesBrain EdemaDian Nita Eka SaptariniNo ratings yet
- Dowd 2017 Basal GangliaDocument9 pagesDowd 2017 Basal Gangliasingle_ladyNo ratings yet
- Awake CraniotomyDocument28 pagesAwake CraniotomyBeba EchevarriaNo ratings yet
- Margret Jensdottir Learning Curve Analysis and AdverseDocument9 pagesMargret Jensdottir Learning Curve Analysis and AdverseJesus PerezNo ratings yet
- Pi Is 1094715921064345Document7 pagesPi Is 1094715921064345syarifaNo ratings yet
- Awake Neurosurgery An UpdateDocument5 pagesAwake Neurosurgery An UpdatevictoriaefernandezNo ratings yet
- Superiority of Continuous Over Intermittent Intraoperative Nerve Monitoring in Preventing Vocal Cord PalsyDocument9 pagesSuperiority of Continuous Over Intermittent Intraoperative Nerve Monitoring in Preventing Vocal Cord PalsyazharbattooNo ratings yet
- Fenoy 2017Document7 pagesFenoy 2017syarifaNo ratings yet
- Deep Brain Stimulation of Posterior Hypothalamic Area For Cluster Headache: A Retrospective Case SeriesDocument5 pagesDeep Brain Stimulation of Posterior Hypothalamic Area For Cluster Headache: A Retrospective Case SeriesegyzellahsNo ratings yet
- Oup Accepted Manuscript 2020Document8 pagesOup Accepted Manuscript 2020renianggrainiNo ratings yet
- % Dextrose Water As The Primary: Stanley K. H. Lam, Kenneth Dean Reeves, and An-Lin ChengDocument18 pages% Dextrose Water As The Primary: Stanley K. H. Lam, Kenneth Dean Reeves, and An-Lin ChengFloyd. BNo ratings yet
- Baru 2Document12 pagesBaru 2Bianca CaterinalisendraNo ratings yet
- MedicinaDocument8 pagesMedicinaLetíciaNo ratings yet
- The Very Long-Term Outcome of Radiosurgery For Classical Trigeminal NeuralgiaDocument9 pagesThe Very Long-Term Outcome of Radiosurgery For Classical Trigeminal NeuralgiaJose Damian Lemus IbacacheNo ratings yet
- Intraoperative Radiotherapy During Awake Craniotomies - Preliminary Results of A Single-Center Case SeriesDocument7 pagesIntraoperative Radiotherapy During Awake Craniotomies - Preliminary Results of A Single-Center Case Seriesuyenminh2802No ratings yet
- Biomedicines: Peripheral Nerve Stimulation: The Evolution in Pain MedicineDocument4 pagesBiomedicines: Peripheral Nerve Stimulation: The Evolution in Pain MedicineGiancarlo Gardella MartínezNo ratings yet
- Martins 2008Document8 pagesMartins 2008Sebastian GiovanniniNo ratings yet
- Eeg UsDocument6 pagesEeg UsnetoNo ratings yet
- Scalp 2011 (169401)Document10 pagesScalp 2011 (169401)Naufal BinseffNo ratings yet
- Peripheral Nerve Stimulation For Painful Mononeuropathy Secondary To Leprosy: A 12-Month Follow-Up StudyDocument6 pagesPeripheral Nerve Stimulation For Painful Mononeuropathy Secondary To Leprosy: A 12-Month Follow-Up StudySartika Ayu NingsihNo ratings yet
- Treatment of Medically Intractable Cluster Headache by Occipital Nerve Stimulation: Long-Term Follow-Up of Eight PatientsDocument8 pagesTreatment of Medically Intractable Cluster Headache by Occipital Nerve Stimulation: Long-Term Follow-Up of Eight PatientsareteusNo ratings yet
- Advancesinanesthesia Monitoring: Yi Deng,, Jovany Cruz Navarro,, Sandeep MarkanDocument9 pagesAdvancesinanesthesia Monitoring: Yi Deng,, Jovany Cruz Navarro,, Sandeep MarkanUmer HussainNo ratings yet
- Article in Press: Surgical Management of Persistent Post-Traumatic Trans-Tentorial Brain HerniaDocument8 pagesArticle in Press: Surgical Management of Persistent Post-Traumatic Trans-Tentorial Brain HerniaGatoNo ratings yet
- Neurosurgeons' Armamentarium For The Management of Refractory Postherpetic Neuralgia: A Systematic Literature ReviewDocument11 pagesNeurosurgeons' Armamentarium For The Management of Refractory Postherpetic Neuralgia: A Systematic Literature ReviewJaime XavierNo ratings yet
- Dorsal RhizotomyDocument13 pagesDorsal RhizotomyAiman MaidanNo ratings yet
- Awake Glioma Surgery: Technical Evolution and NuancesDocument32 pagesAwake Glioma Surgery: Technical Evolution and NuancesVito MasagusNo ratings yet
- Coene N 2011Document7 pagesCoene N 2011Estereotaxia BrasilNo ratings yet
- Resection of Gliomas With and Without Neuropsychological Support During Awake Craniotomy-Effects On Surgery and Clinical OutcomeDocument8 pagesResection of Gliomas With and Without Neuropsychological Support During Awake Craniotomy-Effects On Surgery and Clinical OutcomeHellen SantosNo ratings yet
- Occipital NeuralgiaDocument12 pagesOccipital NeuralgiaStudentNo ratings yet
- John D. Heiss Et Al - Local Distribution and Toxicity of Prolonged Hippocampal Infusion of MuscimolDocument11 pagesJohn D. Heiss Et Al - Local Distribution and Toxicity of Prolonged Hippocampal Infusion of MuscimolCortate15gNo ratings yet
- Personalised, Image-Guided, Noninvasive Brain Stimulation in Gliomas - Rationale, Challenges & OpportunitiesDocument12 pagesPersonalised, Image-Guided, Noninvasive Brain Stimulation in Gliomas - Rationale, Challenges & OpportunitiesshylajaNo ratings yet
- JNS Role of Electrophysiology in Guiding Near Total Resection For Preservation of Facial Nerve Function in The Surgical Treatment of Large Vestibular SchwannomasDocument8 pagesJNS Role of Electrophysiology in Guiding Near Total Resection For Preservation of Facial Nerve Function in The Surgical Treatment of Large Vestibular SchwannomasAlejandro CheritNo ratings yet
- Motor Cortex Stimulation For Neuropathic Facial Pain: Nikolai G. Rainov and Volkmar HeideckeDocument5 pagesMotor Cortex Stimulation For Neuropathic Facial Pain: Nikolai G. Rainov and Volkmar HeideckemoiNo ratings yet
- Peripheral Nerve Block (PNB)Document1 pagePeripheral Nerve Block (PNB)ridhoadityaNo ratings yet
- Endarterectomia 2Document12 pagesEndarterectomia 2Andrea RangelNo ratings yet
- Current Concept in Adult Peripheral Nerve and Brachial Plexus SurgeryDocument8 pagesCurrent Concept in Adult Peripheral Nerve and Brachial Plexus SurgeryJhon Fredy Castañeda LopezNo ratings yet
- Dexmedetomidine Vs Propofol-Remifentanil Conscious Sedation For Awake Craniotomy: A Prospective Randomized Controlled TrialDocument59 pagesDexmedetomidine Vs Propofol-Remifentanil Conscious Sedation For Awake Craniotomy: A Prospective Randomized Controlled TrialRashid MurtazaNo ratings yet
- Koziarz 2019Document11 pagesKoziarz 2019Thiago DiasNo ratings yet
- Research Article: Stanley K. H. Lam, Kenneth Dean Reeves, and An-Lin ChengDocument18 pagesResearch Article: Stanley K. H. Lam, Kenneth Dean Reeves, and An-Lin ChengSebastiano SerraNo ratings yet
- J Neurol Neurosurg Psychiatry 2005 Mallik Ii23 31Document10 pagesJ Neurol Neurosurg Psychiatry 2005 Mallik Ii23 31أحمد عطيةNo ratings yet
- EMG Response of Facial Nerve Stimulation Under Different LevelsDocument9 pagesEMG Response of Facial Nerve Stimulation Under Different LevelsAlejandro CheritNo ratings yet
- Echography and Doppler of the BrainFrom EverandEchography and Doppler of the BrainChiara RobbaNo ratings yet
- Database of Functional Neurosurgery TargetsDocument8 pagesDatabase of Functional Neurosurgery TargetsEstereotaxia BrasilNo ratings yet
- Anatomia STN Clement HamaniDocument17 pagesAnatomia STN Clement HamaniEstereotaxia BrasilNo ratings yet
- Art. CC McIntyre - Electric Field and Stimulating Influence Generated by Deep Brain Stimulation of The Subthalamic NucleusDocument7 pagesArt. CC McIntyre - Electric Field and Stimulating Influence Generated by Deep Brain Stimulation of The Subthalamic NucleusEstereotaxia BrasilNo ratings yet
- 10 0000@m Neurology Org@m@85@23@2075Document3 pages10 0000@m Neurology Org@m@85@23@2075Estereotaxia BrasilNo ratings yet
- Kerrigan 2004Document9 pagesKerrigan 2004Estereotaxia BrasilNo ratings yet
- 907 FullDocument10 pages907 FullHugo Whysk LeonardoNo ratings yet
- The Current State of Deep Brain Stimulation For Chronic Pain and Its Context in Other Forms of NeuromodulationDocument19 pagesThe Current State of Deep Brain Stimulation For Chronic Pain and Its Context in Other Forms of NeuromodulationEstereotaxia BrasilNo ratings yet
- 10 0000@m Neurology Org@m@66@10@1490Document6 pages10 0000@m Neurology Org@m@66@10@1490Estereotaxia BrasilNo ratings yet
- Pedunculopontine Nucleus Region Deep Brain Stimulation in Parkinson Disease: Surgical Techniques, Side Effects, and Postoperative ImagingDocument13 pagesPedunculopontine Nucleus Region Deep Brain Stimulation in Parkinson Disease: Surgical Techniques, Side Effects, and Postoperative ImagingEstereotaxia BrasilNo ratings yet
- Art. L Zrinzo - Intra-Operative Recordings of Local Field Potentials Can Help Localize The Subthalamic Nucleus in Parkinson's Disease SurgeryDocument8 pagesArt. L Zrinzo - Intra-Operative Recordings of Local Field Potentials Can Help Localize The Subthalamic Nucleus in Parkinson's Disease SurgeryEstereotaxia BrasilNo ratings yet
- Art. AL Benabid - Deep Brain Stimulation For Parkinson's DiseaseDocument11 pagesArt. AL Benabid - Deep Brain Stimulation For Parkinson's DiseaseEstereotaxia BrasilNo ratings yet
- Deep Brain Stimulation For Essential Tremor: Targeting The Dentato-Rubro-Thalamic Tract?Document9 pagesDeep Brain Stimulation For Essential Tremor: Targeting The Dentato-Rubro-Thalamic Tract?Estereotaxia BrasilNo ratings yet
- Fisher 2010Document10 pagesFisher 2010Estereotaxia BrasilNo ratings yet
- Art. PA Star - Implantation of Deep Brain Stimulators Into The Subthalamic Nucleus Technical Approach and RM Imaging-Verified Lead LocationsDocument18 pagesArt. PA Star - Implantation of Deep Brain Stimulators Into The Subthalamic Nucleus Technical Approach and RM Imaging-Verified Lead LocationsEstereotaxia BrasilNo ratings yet
- Art. L Zrinzo - Basal Ganglia Local Field Potential Activity Character and Functional Significance in The HumanDocument10 pagesArt. L Zrinzo - Basal Ganglia Local Field Potential Activity Character and Functional Significance in The HumanEstereotaxia BrasilNo ratings yet
- Art. L Zrinzo - Deep Brain Stimulation Between 1947 and 1987 The Untold StoryDocument10 pagesArt. L Zrinzo - Deep Brain Stimulation Between 1947 and 1987 The Untold StoryEstereotaxia BrasilNo ratings yet
- Coene N 2011Document7 pagesCoene N 2011Estereotaxia BrasilNo ratings yet
- Art. L Zrinzo - Intra-Operative STN DBS Attenuates The Prominent Beta Rhythm in The STN in Parkinson's DiseaseDocument8 pagesArt. L Zrinzo - Intra-Operative STN DBS Attenuates The Prominent Beta Rhythm in The STN in Parkinson's DiseaseEstereotaxia BrasilNo ratings yet
- Art. L Zrinzo - Effect of Electrode Contact Location On Clinical Efficacy of Pallidal Deep Brain Stimulation in Primary Generalised DystoniaDocument6 pagesArt. L Zrinzo - Effect of Electrode Contact Location On Clinical Efficacy of Pallidal Deep Brain Stimulation in Primary Generalised DystoniaEstereotaxia BrasilNo ratings yet
- Art. L Zrinzo - Bilateral Globus Pallidus Stimulation For Severe Tourette'sDocument11 pagesArt. L Zrinzo - Bilateral Globus Pallidus Stimulation For Severe Tourette'sEstereotaxia BrasilNo ratings yet
- Double Target DBS For Essential TremorDocument4 pagesDouble Target DBS For Essential TremorEstereotaxia BrasilNo ratings yet
- Starr PA. Placement of Deep Brain Stimulators Into The STN and GPI - Planning TechniquesDocument28 pagesStarr PA. Placement of Deep Brain Stimulators Into The STN and GPI - Planning TechniquesEstereotaxia BrasilNo ratings yet
- Art. L Zrinzo - Adaptive Deep Brain Stimulation in Advanced Parkinson DiseaseDocument9 pagesArt. L Zrinzo - Adaptive Deep Brain Stimulation in Advanced Parkinson DiseaseEstereotaxia BrasilNo ratings yet
- Art. L Zrinzo - Intra-Operative Recordings of Local Field Potentials Can Help Localize The Subthalamic Nucleus in Parkinson's Disease SurgeryDocument8 pagesArt. L Zrinzo - Intra-Operative Recordings of Local Field Potentials Can Help Localize The Subthalamic Nucleus in Parkinson's Disease SurgeryEstereotaxia BrasilNo ratings yet
- The Current State of Deep Brain Stimulation For Chronic Pain and Its Context in Other Forms of NeuromodulationDocument19 pagesThe Current State of Deep Brain Stimulation For Chronic Pain and Its Context in Other Forms of NeuromodulationEstereotaxia BrasilNo ratings yet
- Art. L Zrinzo - Basal Ganglia Local Field Potential Activity Character and Functional Significance in The HumanDocument10 pagesArt. L Zrinzo - Basal Ganglia Local Field Potential Activity Character and Functional Significance in The HumanEstereotaxia BrasilNo ratings yet
- Art. PA Star - Implantation of Deep Brain Stimulators Into The Subthalamic Nucleus Technical Approach and RM Imaging-Verified Lead LocationsDocument18 pagesArt. PA Star - Implantation of Deep Brain Stimulators Into The Subthalamic Nucleus Technical Approach and RM Imaging-Verified Lead LocationsEstereotaxia BrasilNo ratings yet
- Benabid Long Term StimDocument12 pagesBenabid Long Term StimEstereotaxia BrasilNo ratings yet
- Art. L Zrinzo - Deep Brain Stimulation Between 1947 and 1987 The Untold StoryDocument10 pagesArt. L Zrinzo - Deep Brain Stimulation Between 1947 and 1987 The Untold StoryEstereotaxia BrasilNo ratings yet
- AT2 ERT Installation GuideDocument3 pagesAT2 ERT Installation GuideYordan Silva GomezNo ratings yet
- Introduction To DSADocument11 pagesIntroduction To DSAdhiraj1223353No ratings yet
- Math 1712Document11 pagesMath 1712fake emailNo ratings yet
- Science 8-Quarter 2-Lesson 3Document16 pagesScience 8-Quarter 2-Lesson 3Ms. Rhonabelle Llerin PagudNo ratings yet
- AC PPTDocument28 pagesAC PPTPrajwal BirwadkarNo ratings yet
- Semi-Finished Products: For Extreme Applications Pe, PP, PVDF, Ectfe, Fep, PfaDocument16 pagesSemi-Finished Products: For Extreme Applications Pe, PP, PVDF, Ectfe, Fep, PfaLuciano CortisNo ratings yet
- Chenmko Enterprise Co.,Ltd: CHN202UPT Surface MountDocument3 pagesChenmko Enterprise Co.,Ltd: CHN202UPT Surface MountAlberto CardenasNo ratings yet
- Climaveneta CVM 20 ManualDocument20 pagesClimaveneta CVM 20 ManualisaNo ratings yet
- Harmonic EspritDocument9 pagesHarmonic EspritNizar TayemNo ratings yet
- A Map of The Interconnection Between Keys: Fractal Key of That NoteDocument1 pageA Map of The Interconnection Between Keys: Fractal Key of That NoteJohn Arturo Talavera MendozaNo ratings yet
- User Manual Quality Espresso MachinesDocument56 pagesUser Manual Quality Espresso MachinesEdward GarzónNo ratings yet
- s67 Rosen Thermo - Hi.pvc Iz 2018 enDocument34 pagess67 Rosen Thermo - Hi.pvc Iz 2018 enSomea NoneaNo ratings yet
- Che Vol1Document139 pagesChe Vol1abiramanNo ratings yet
- E220-400M30S UserManual EN v1.0-1Document14 pagesE220-400M30S UserManual EN v1.0-1Predrag VisnjicNo ratings yet
- IINNO Catalogue2012 01 SMART 021112 B PDFDocument25 pagesIINNO Catalogue2012 01 SMART 021112 B PDFmiraijewelsNo ratings yet
- Verb Morphological Generator For TeluguDocument11 pagesVerb Morphological Generator For TeluguSasi Raja Sekhar DokkaraNo ratings yet
- 001-03 - Hydraulic Charge Pressure Switch Shorted To High SourceDocument6 pages001-03 - Hydraulic Charge Pressure Switch Shorted To High Sourceكؤمپيوته رى ديارىNo ratings yet
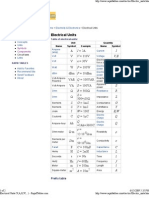
- Electrical UnitsDocument2 pagesElectrical Unitsevtoma100% (1)
- Executive Summary by Dr. Eugene Brigham and Dr. Joel HoustonDocument12 pagesExecutive Summary by Dr. Eugene Brigham and Dr. Joel HoustonCharisseMaeM.CarreonNo ratings yet
- Ees ManualDocument191 pagesEes ManualMohd Jamal Mohd MoktarNo ratings yet
- Risk and Return-1Document57 pagesRisk and Return-1Marri Denyel CordetaNo ratings yet
- Sunshape Thesis - Wilbert - DLRDocument177 pagesSunshape Thesis - Wilbert - DLRAhmed AlshehrriNo ratings yet
- Frequent Itemset MiningDocument58 pagesFrequent Itemset MiningMesut ErkekliNo ratings yet
- Green Synthesis of Copper Nanoparticles and Its CharacterizationDocument5 pagesGreen Synthesis of Copper Nanoparticles and Its CharacterizationNicolas MolinaNo ratings yet
- Timeline of The IT ERADocument23 pagesTimeline of The IT ERAJohn Gil Talangan PadieNo ratings yet