You might also like
- NIIT - Back Ground Verification FormDocument9 pagesNIIT - Back Ground Verification FormLavneetNo ratings yet
- Hotel Marketing PlanDocument29 pagesHotel Marketing PlanAdnan AliNo ratings yet
- P45 Part 1A Details of Employee Leaving WorkDocument3 pagesP45 Part 1A Details of Employee Leaving WorkDan NolanNo ratings yet
- Register of InjuryDocument3 pagesRegister of InjurypenichopsNo ratings yet
- Form Accident ReportDocument4 pagesForm Accident ReportKarthik SNo ratings yet
- 5184 P45 (Online) PDFDocument3 pages5184 P45 (Online) PDFAlejandroe AuditoreNo ratings yet
- Enterprise - Entrepreneurship and Innovation - Concepts, Contexts and Commercialization (PDFDrive)Document572 pagesEnterprise - Entrepreneurship and Innovation - Concepts, Contexts and Commercialization (PDFDrive)hardiyanti pratiwiNo ratings yet
- Copy For Employee: P45 Part 1A Details of Employee Leaving WorkDocument3 pagesCopy For Employee: P45 Part 1A Details of Employee Leaving WorkSteve OrtonNo ratings yet
- P45 68148Document4 pagesP45 68148Эдварт АнтонNo ratings yet
- Employee Vehicle AccidentDocument2 pagesEmployee Vehicle AccidentlintangNo ratings yet
- Bristol Meyers Squibb CompanyDocument20 pagesBristol Meyers Squibb CompanyAkmal Kemal Hadi100% (4)
- HSE Leaving Form - HR106: Section 1. To Be Completed by The EmployeeDocument3 pagesHSE Leaving Form - HR106: Section 1. To Be Completed by The EmployeeLexNo ratings yet
- Copy For Employee: P45 Part 1A Details of Employee Leaving WorkDocument3 pagesCopy For Employee: P45 Part 1A Details of Employee Leaving WorkDenis VitalieviciNo ratings yet
- (MEMO) Daily Timekeeping and Recording GuidelineDocument2 pages(MEMO) Daily Timekeeping and Recording GuidelineCoco MondejarNo ratings yet
- P45 Part 1A Details of Employee Leaving WorkDocument3 pagesP45 Part 1A Details of Employee Leaving WorkCaleb PriceNo ratings yet
- Copy For Employee: Complete Only If Tax Code Is Cumulative. If There Is AnDocument3 pagesCopy For Employee: Complete Only If Tax Code Is Cumulative. If There Is AnZavache DanaNo ratings yet
- Retired Free Supply FormDocument8 pagesRetired Free Supply Formmwmalhr6654No ratings yet
- Cepci 2015Document2 pagesCepci 2015mafechu100% (7)
- Everton Mattos: Direction of Authorization - ClaimsDocument2 pagesEverton Mattos: Direction of Authorization - ClaimsEverton MattosNo ratings yet
- Wsib 012386Document5 pagesWsib 012386rajNo ratings yet
- WSIB Form6Document4 pagesWSIB Form6Ginette BelangerNo ratings yet
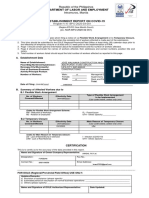
- Return To Work Establishment Report Form v3Document3 pagesReturn To Work Establishment Report Form v3raymond paul adelantarNo ratings yet
- Injury Report Instructions: Worker DetailsDocument5 pagesInjury Report Instructions: Worker DetailsAfzal ImamNo ratings yet
- Pension Rate of Pay Application Form - HR 114: - Section 1. To Be Completed by The EmployeeDocument2 pagesPension Rate of Pay Application Form - HR 114: - Section 1. To Be Completed by The EmployeeLexNo ratings yet
- Reset: Employer's Report of Injury or Occupational DiseaseDocument3 pagesReset: Employer's Report of Injury or Occupational DiseasePSNo ratings yet
- 0008a 08 11 Fs Web RV 09 18-1Document3 pages0008a 08 11 Fs Web RV 09 18-1OvadoseNo ratings yet
- Member Data Change Request Form Form E 4Document5 pagesMember Data Change Request Form Form E 4rachel montanoNo ratings yet
- P45 94142 (1) BunDocument4 pagesP45 94142 (1) BunCosty DutaNo ratings yet
- ACostE Application FormDocument7 pagesACostE Application FormJithin FrancizNo ratings yet
- Full Employee ReportDocument3 pagesFull Employee ReportXYZNo ratings yet
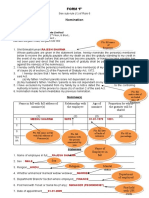
- Form 7 Report FORMATDocument2 pagesForm 7 Report FORMATedgie.soquiasNo ratings yet
- Form F - GuidlineDocument2 pagesForm F - GuidlineVAMSI KRISHNA BOMMISETTYNo ratings yet
- P45 (Online) - LJDocument3 pagesP45 (Online) - LJGreat EmmanuelNo ratings yet
- Temporary Rehabilitation Remuneration Form-HR114: Section 1. To Be Completed by The EmployeeDocument3 pagesTemporary Rehabilitation Remuneration Form-HR114: Section 1. To Be Completed by The EmployeeLexNo ratings yet
- Department of Labor and Employment: Republic of The Philippines Intramuros, ManilaDocument2 pagesDepartment of Labor and Employment: Republic of The Philippines Intramuros, ManilaElaine Fiona VillafuerteNo ratings yet
- 475 1257L SR460976A MR 2: P45 Part 1A Details of Employee Leaving WorkDocument3 pages475 1257L SR460976A MR 2: P45 Part 1A Details of Employee Leaving WorkAlexandru cosminNo ratings yet
- ds158 enDocument2 pagesds158 enDivineThotNo ratings yet
- Background Verification FormDocument4 pagesBackground Verification FormAnitha Ajay Pal SinghNo ratings yet
- Syntel Employment ApplicationDocument2 pagesSyntel Employment ApplicationrusofranklinNo ratings yet
- Wwp-Catch Up Plan-Feb 1-5Document7 pagesWwp-Catch Up Plan-Feb 1-5DocRoms Andres PilongoNo ratings yet
- Retirement & Pension Plan For NYCDCC Employees 2006Document13 pagesRetirement & Pension Plan For NYCDCC Employees 2006Latisha WalkerNo ratings yet
- Workers United Complaint To NLRB Regarding TeslaDocument2 pagesWorkers United Complaint To NLRB Regarding TeslaCNBC.comNo ratings yet
- Vetting of Pay Fixation of SchoolsDocument5 pagesVetting of Pay Fixation of Schoolspinappu0% (1)
- For Printing - A4Document5 pagesFor Printing - A4Andie GalangNo ratings yet
- Department of Labor and Employment: Republic of The Philippines Intramuros, ManilaDocument2 pagesDepartment of Labor and Employment: Republic of The Philippines Intramuros, ManilaKathNo ratings yet
- PCO Accreditation Application Form (Renewal)Document3 pagesPCO Accreditation Application Form (Renewal)car3laNo ratings yet
- Application For Undergraduate Re-Admission / Faculty TransferDocument1 pageApplication For Undergraduate Re-Admission / Faculty TransferGabrielNo ratings yet
- PFF053 Member'SContributionRemittanceForm V03Document12 pagesPFF053 Member'SContributionRemittanceForm V03CA RosarioNo ratings yet
- Work Order Template 07Document1 pageWork Order Template 075 E Hernández Gómez Osmar UlisesNo ratings yet
- Department of Labor and Employment: Republic of The Philippines Intramuros, ManilaDocument2 pagesDepartment of Labor and Employment: Republic of The Philippines Intramuros, ManilaLeowell John RapaconNo ratings yet
- NLRB Charge Student Transp. Am. (Filed Feb. 4, 2011)Document2 pagesNLRB Charge Student Transp. Am. (Filed Feb. 4, 2011)Molly DiBiancaNo ratings yet
- BGV Form (BVF) R1Document2 pagesBGV Form (BVF) R1MK BALANo ratings yet
- Monica Caballero Ortiz - Monica OrtizDocument10 pagesMonica Caballero Ortiz - Monica OrtizLJ Avila LayronNo ratings yet
- ISBN Register of Injuries Template Return To Work Toolkit 2011 07Document3 pagesISBN Register of Injuries Template Return To Work Toolkit 2011 07Rakesh KaushikNo ratings yet
- John Thomas ApplicationDocument7 pagesJohn Thomas ApplicationkevinhfdNo ratings yet
- Recruitment q1 2023Document47 pagesRecruitment q1 2023Ferby RamosNo ratings yet
- Background Verification Form (BVF) : Personal InformationDocument2 pagesBackground Verification Form (BVF) : Personal InformationMarshall0% (1)
- Workplace Injury/ Illness Report FormDocument2 pagesWorkplace Injury/ Illness Report FormDimpho MasetediNo ratings yet
- FM Embrvi CPD Awps Wpu 03Document3 pagesFM Embrvi CPD Awps Wpu 03DMALL MANG INASALNo ratings yet
- Guidance For Completion of The Application For Employment FormDocument9 pagesGuidance For Completion of The Application For Employment FormterryfediwNo ratings yet
- Anssi Profil PP 2015 01à06Document215 pagesAnssi Profil PP 2015 01à06Vaibhav DafaleNo ratings yet
- Chapter I PsychologyDocument8 pagesChapter I PsychologyVaibhav DafaleNo ratings yet
- Common Summary Assessment ReportDocument4 pagesCommon Summary Assessment ReportVaibhav DafaleNo ratings yet
- How To Build Csars: For OpentoscaDocument25 pagesHow To Build Csars: For OpentoscaVaibhav DafaleNo ratings yet
- CsarDocument56 pagesCsarVaibhav DafaleNo ratings yet
- An Introduction To The CSAR Package: Jose M Muino May 19, 2021Document5 pagesAn Introduction To The CSAR Package: Jose M Muino May 19, 2021Vaibhav DafaleNo ratings yet
- Gs Nfv-Sol004v020501pDocument21 pagesGs Nfv-Sol004v020501pVaibhav DafaleNo ratings yet
- Personal Information (Popi) Act: Protection ofDocument2 pagesPersonal Information (Popi) Act: Protection ofVaibhav DafaleNo ratings yet
- Joju Charging Emergency Services BrochureDocument8 pagesJoju Charging Emergency Services BrochureVaibhav DafaleNo ratings yet
- CSARGuidance DocumentDocument11 pagesCSARGuidance DocumentVaibhav DafaleNo ratings yet
- Banking Technology and Service Quality: Evidence From Private Sector Banks in KeralaDocument6 pagesBanking Technology and Service Quality: Evidence From Private Sector Banks in KeralaVaibhav DafaleNo ratings yet
- Functional Abilities FormDocument2 pagesFunctional Abilities FormVaibhav DafaleNo ratings yet
- Hydrogeological Report: Atal Bhujal Yojana (Atal Jal)Document16 pagesHydrogeological Report: Atal Bhujal Yojana (Atal Jal)Vaibhav DafaleNo ratings yet
- Hydrogeological Report: Atal Bhujal Yojana (Ataljal)Document15 pagesHydrogeological Report: Atal Bhujal Yojana (Ataljal)Vaibhav DafaleNo ratings yet
- Guidelines For Attorneys On The Protection of Personal Information ActDocument31 pagesGuidelines For Attorneys On The Protection of Personal Information ActVaibhav DafaleNo ratings yet
- Talukawise GWA2008-09Document166 pagesTalukawise GWA2008-09Vaibhav DafaleNo ratings yet
- Hydrogeological Report: Atal Bhujal Yojana (Ataljal)Document17 pagesHydrogeological Report: Atal Bhujal Yojana (Ataljal)Vaibhav DafaleNo ratings yet
- 297 Authors: Institution: Department of Urology, Eulji University, College of Medicine TitleDocument1 page297 Authors: Institution: Department of Urology, Eulji University, College of Medicine TitleVaibhav DafaleNo ratings yet
- 2102 13225Document19 pages2102 13225Vaibhav DafaleNo ratings yet
- Em 602Document23 pagesEm 602Vaibhav DafaleNo ratings yet
- BIS Working Papers: The Dollar, Bank Leverage and Real Economic Activity: An Evolving RelationshipDocument18 pagesBIS Working Papers: The Dollar, Bank Leverage and Real Economic Activity: An Evolving RelationshipVaibhav DafaleNo ratings yet
- Hemani Neil SNR Thesis WebDocument89 pagesHemani Neil SNR Thesis WebVaibhav DafaleNo ratings yet
- Dec 2016Document72 pagesDec 2016Vaibhav DafaleNo ratings yet
- Mie L1 AbDocument38 pagesMie L1 AbSakshi MNo ratings yet
- Rentmycar: - A P2P Car Rental Service in IndonesiaDocument23 pagesRentmycar: - A P2P Car Rental Service in IndonesiaRitika SharmaNo ratings yet
- 2022 Deloitte Global Cxo Sustainability ReportDocument23 pages2022 Deloitte Global Cxo Sustainability ReportVenkata SaiNo ratings yet
- ESSAY1Document9 pagesESSAY1Dang Le Phuong Nhi (FGW DN)No ratings yet
- Procurement and Human Resources Business ProcessDocument33 pagesProcurement and Human Resources Business ProcessSurya Patra AbdilahNo ratings yet
- DSB Q3Document8 pagesDSB Q3William HarrisNo ratings yet
- Strategic Management and Project Management: PurposeDocument10 pagesStrategic Management and Project Management: PurposesurapolNo ratings yet
- Brand Manual v2 May 2020Document30 pagesBrand Manual v2 May 2020Pian SopianNo ratings yet
- Personal Luxury in Indonesia - Datagraphics: Country Report - Jan 2020Document4 pagesPersonal Luxury in Indonesia - Datagraphics: Country Report - Jan 2020Elle ANo ratings yet
- NewGen IEDCDocument19 pagesNewGen IEDCpkk thampiNo ratings yet
- MarketsandMarkets - Corporate CapabilitiesDocument32 pagesMarketsandMarkets - Corporate CapabilitiesKaranvir singhNo ratings yet
- System AnalysisDocument7 pagesSystem AnalysisNNADI EMMANUELNo ratings yet
- Financial Ratio AnalysisDocument32 pagesFinancial Ratio AnalysisTriechia LaudNo ratings yet
- Rocket ReachDocument4 pagesRocket Reachbhaskar ghoshNo ratings yet
- Otus - Malik Gold - Klein WatchesDocument1 pageOtus - Malik Gold - Klein Watchesabdulbasit.omar1997No ratings yet
- BLD 2332 - English Marekting-: Name of Lecturer:Nur Azlin Fatesah BT AzaddinDocument6 pagesBLD 2332 - English Marekting-: Name of Lecturer:Nur Azlin Fatesah BT AzaddinIntan SalwaniNo ratings yet
- Unit 1 (D)Document18 pagesUnit 1 (D)priya dharshiniNo ratings yet
- Type of Branding Umbrella and Multi BrandingDocument14 pagesType of Branding Umbrella and Multi BrandingEAGANBABU SMNo ratings yet
- MKT 337 Chapter 10Document23 pagesMKT 337 Chapter 10Ahsan AnikNo ratings yet
- Manaksia Company PresentationDocument21 pagesManaksia Company Presentationparth sarthyNo ratings yet
- Reconstructions - Amalgamation, Mergers, TakeoversDocument5 pagesReconstructions - Amalgamation, Mergers, Takeoversmasiga mauriceNo ratings yet
- Organizational Change Management ConceptsDocument10 pagesOrganizational Change Management ConceptsRonald MulleyNo ratings yet
- Travel Agent New Application Guide (He-Ae) Ngiss - PakistanDocument8 pagesTravel Agent New Application Guide (He-Ae) Ngiss - PakistanFaisal ImtiazNo ratings yet
- PASS OutstandingDocument3 pagesPASS Outstandingtvsufi.comNo ratings yet
- (Company Name) (Month) (Emd-Mcr) 2 (6 Below Chemical Count)Document1 page(Company Name) (Month) (Emd-Mcr) 2 (6 Below Chemical Count)Allan ResmaNo ratings yet
- Commercial MouDocument4 pagesCommercial MouALOKE GANGULY100% (1)