You might also like
- Rizal JournalDocument2 pagesRizal Journallindzy.amurao01No ratings yet
- 10 1111@anae 15054 PDFDocument33 pages10 1111@anae 15054 PDFJuliana Rodriguez MariñoNo ratings yet
- Jama Murthy 2020 It 200008Document2 pagesJama Murthy 2020 It 200008jorgeNo ratings yet
- Dr. Hendri - Early Warning System & PPEDocument106 pagesDr. Hendri - Early Warning System & PPEViniFortunataNo ratings yet
- Care For Critically Ill Patients With COVID-19: Clinical UpdateDocument2 pagesCare For Critically Ill Patients With COVID-19: Clinical UpdateNicole BatistaNo ratings yet
- Consensus Statement: Safe Airway Society Principles of Airway Management and Tracheal Intubation Specific To The COVID-19 Adult Patient GroupDocument10 pagesConsensus Statement: Safe Airway Society Principles of Airway Management and Tracheal Intubation Specific To The COVID-19 Adult Patient GroupMeska AmeliaNo ratings yet
- Mja2 50598Document10 pagesMja2 50598Andi Astrid AmaliaNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - Anesthetic Concerns, Including Airway Management and Infection ControlDocument32 pagesCoronavirus Disease 2019 (COVID-19) - Anesthetic Concerns, Including Airway Management and Infection ControlT GalenNo ratings yet
- COVID-19: A Quick Look at Aspects of Critical CareDocument5 pagesCOVID-19: A Quick Look at Aspects of Critical CareJbarrianNo ratings yet
- N 5 RFTKV BGYTs 6 N Vyd 7 GMC 3 CDocument18 pagesN 5 RFTKV BGYTs 6 N Vyd 7 GMC 3 CGeysel SuarezNo ratings yet
- Jurnal Deskriptif IngDocument6 pagesJurnal Deskriptif IngAulin putri damayantiNo ratings yet
- Respiratory Support For Adult Patients With COVID-19Document7 pagesRespiratory Support For Adult Patients With COVID-19SekarNo ratings yet
- Pneumomediastinum and Subcutaneous Emphysema in COVID-19: Barotrauma or Lung Frailty?Document7 pagesPneumomediastinum and Subcutaneous Emphysema in COVID-19: Barotrauma or Lung Frailty?Prayudo Mahendra PutraNo ratings yet
- Tracheostomy in The COVID 19 PandemicDocument3 pagesTracheostomy in The COVID 19 PandemicKenjiNo ratings yet
- Novel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited SettingsDocument8 pagesNovel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited Settingsdiah Bayu siswantiNo ratings yet
- Jurnal 2Document8 pagesJurnal 2DelisQurrotaA'yunNo ratings yet
- Anesthetics and AnesthesiologyDocument5 pagesAnesthetics and AnesthesiologykhairaniNo ratings yet
- Jurding KLP A Anes 3Document18 pagesJurding KLP A Anes 3mreza26No ratings yet
- Jamaotolaryngology Givi 2020 SC 200001Document6 pagesJamaotolaryngology Givi 2020 SC 200001dina ayu SeptianiNo ratings yet
- Helmet CPAP To Treat Acute Hypoxemic Respiratory Failure in Patients With COVID-19: A Management Strategy ProposalDocument8 pagesHelmet CPAP To Treat Acute Hypoxemic Respiratory Failure in Patients With COVID-19: A Management Strategy Proposaladliah zahiraNo ratings yet
- Pemiihan Anestesi Pada Pasien C-19Document10 pagesPemiihan Anestesi Pada Pasien C-19Nabilah PutiNo ratings yet
- Document Can Be Found At:: /hcp/non-Us-Settings/overview/index - HTMLDocument25 pagesDocument Can Be Found At:: /hcp/non-Us-Settings/overview/index - HTMLMaqbool AlizaiNo ratings yet
- Recommendations For Prehospital Airway Management in Patients With Suspected COVID-19 InfectionDocument5 pagesRecommendations For Prehospital Airway Management in Patients With Suspected COVID-19 InfectionConnor StephensonNo ratings yet
- 1 s2.0 S1479666X20301888 MainDocument5 pages1 s2.0 S1479666X20301888 MainTécnicos CredineNo ratings yet
- Dr. Dian Nurul Al Amini, SP - THTDocument6 pagesDr. Dian Nurul Al Amini, SP - THTRifaniNugrohoNo ratings yet
- High-Flow, Noninvasive Ventilation and Awake (Nonintubation) Proning in Patients With Coronavirus Disease 2019 With Respiratory FailureDocument11 pagesHigh-Flow, Noninvasive Ventilation and Awake (Nonintubation) Proning in Patients With Coronavirus Disease 2019 With Respiratory FailureCamila Fernanda Rivera ArayaNo ratings yet
- COVID19-Overview PresentationDocument25 pagesCOVID19-Overview PresentationAmany AymanNo ratings yet
- Novel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited SettingsDocument9 pagesNovel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited SettingsHanni HarahapNo ratings yet
- Anaesthesia ACTUAL GuidelineDocument16 pagesAnaesthesia ACTUAL Guidelinetam meiNo ratings yet
- Severe Covid-19: Clinical PracticeDocument10 pagesSevere Covid-19: Clinical Practicemarcelocarvalhoteacher2373No ratings yet
- Guidance For Otolaryngology Health Care Workers Performing Aerosol Generating Medical Procedures During The COVID-19 PandemicDocument8 pagesGuidance For Otolaryngology Health Care Workers Performing Aerosol Generating Medical Procedures During The COVID-19 PandemicUsuario CyVNo ratings yet
- NEJM Severe COVIDDocument10 pagesNEJM Severe COVIDErick Roa GandicaNo ratings yet
- A Protocol of Infection Control For Mechanical Thrombectomy in Possible COVID-19 Patients: Tokai University COVID-19 ManualDocument5 pagesA Protocol of Infection Control For Mechanical Thrombectomy in Possible COVID-19 Patients: Tokai University COVID-19 ManualMartha OktaviaNo ratings yet
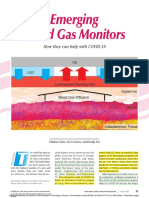
- 2020 Emerging Blood Gas MonitorsDocument15 pages2020 Emerging Blood Gas MonitorsSHANU KUMARNo ratings yet
- Airway Management Guidance For The Endemic Phase of COVID-19Document10 pagesAirway Management Guidance For The Endemic Phase of COVID-19Kamar Operasi Hermina BogorNo ratings yet
- An Intermediate Respiratory Care Unit in Every - 2023 - Archivos de BronconeumoDocument3 pagesAn Intermediate Respiratory Care Unit in Every - 2023 - Archivos de BronconeumoJuan Manuel Claros BustosNo ratings yet
- 2 Epitaxis Covid19Document3 pages2 Epitaxis Covid19andinNo ratings yet
- CCJM 87a ccc033 FullDocument4 pagesCCJM 87a ccc033 FullKamar Operasi Hermina BogorNo ratings yet
- Covid-19: Negative Pressure Rooms: Anmf Evidence BriefDocument5 pagesCovid-19: Negative Pressure Rooms: Anmf Evidence BriefninesuNo ratings yet
- Severe Covid-19Document10 pagesSevere Covid-19Gabriela ArvelaezNo ratings yet
- COVID-19 Disease Invasive VentilationDocument8 pagesCOVID-19 Disease Invasive VentilationfikriafisNo ratings yet
- Supporting The Health Care Workforce During The COVID-19 Global EpidemicDocument2 pagesSupporting The Health Care Workforce During The COVID-19 Global EpidemicDema AlsouqiNo ratings yet
- Lemme Rs 2020Document19 pagesLemme Rs 2020LirajvNo ratings yet
- Clinical Recommendations For in Hospital Airway Mana - 2021 - Best Practice - ReDocument17 pagesClinical Recommendations For in Hospital Airway Mana - 2021 - Best Practice - ReAbdulaziz AlghamdiNo ratings yet
- Approaches To The Management of Patients in Oral and Maxillofacial Surgery During COVID-19 PandemicDocument21 pagesApproaches To The Management of Patients in Oral and Maxillofacial Surgery During COVID-19 PandemicYahul MazfarNo ratings yet
- Pneumothorax and Pneumomediastinum Among COVID-19 Patients With Mechanical Ventilation: A Case SeriesDocument8 pagesPneumothorax and Pneumomediastinum Among COVID-19 Patients With Mechanical Ventilation: A Case SeriesIJPHSNo ratings yet
- Guiding Airway Management and Personal Protective Equipment For COVID-19 Intubation TeamsDocument2 pagesGuiding Airway Management and Personal Protective Equipment For COVID-19 Intubation TeamsahmdamnnNo ratings yet
- Coronavirus Disease 2019: Epidemiological Factors During Aerosol-Generating Medical ProceduresDocument4 pagesCoronavirus Disease 2019: Epidemiological Factors During Aerosol-Generating Medical ProceduresAbrar Hendri PutraNo ratings yet
- Covid - BLS - I - Évf. Oh - English - 2021Document7 pagesCovid - BLS - I - Évf. Oh - English - 2021bnvjNo ratings yet
- Evolution of Acute Respiratory Distress Syndrome IDocument14 pagesEvolution of Acute Respiratory Distress Syndrome InalgatronNo ratings yet
- Mechanical Ventilation Management in COVID-19 PatientsDocument6 pagesMechanical Ventilation Management in COVID-19 PatientsPuskesmas BaboNo ratings yet
- Rational Use of Personal Protective Equipment (PPE) For Coronavirus Disease (COVID-19)Document9 pagesRational Use of Personal Protective Equipment (PPE) For Coronavirus Disease (COVID-19)Karthick AnbuNo ratings yet
- Precautions For Intubating Patients With COVID-19: To The EditorDocument3 pagesPrecautions For Intubating Patients With COVID-19: To The EditorIvan MoralesNo ratings yet
- Manejo de Ventilacion Covid 19Document16 pagesManejo de Ventilacion Covid 19FRANZ DE ARMASNo ratings yet
- 1 5177078803217777108 PDFDocument26 pages1 5177078803217777108 PDFLais Win AndradeNo ratings yet
- Impact of Coronavirus (COVID-19) On Otolaryngologic Surgery: Brief CommentaryDocument8 pagesImpact of Coronavirus (COVID-19) On Otolaryngologic Surgery: Brief CommentaryHesbon MomanyiNo ratings yet
- Current Problems in Diagnostic Radiology 50 (2021) 284 287Document4 pagesCurrent Problems in Diagnostic Radiology 50 (2021) 284 287Leonard AcsinteNo ratings yet
- Aha RCP CovidDocument3 pagesAha RCP Covidalex zuluagaNo ratings yet
- Covid-19 Airway Management and Ventilation Strategy for Critically Ill Older PatientsFrom EverandCovid-19 Airway Management and Ventilation Strategy for Critically Ill Older PatientsNicola VargasNo ratings yet
- COVID-19’s Consequences on the Cardiovascular System: Immediate, Intermediate, and Long-Term ComplicationsFrom EverandCOVID-19’s Consequences on the Cardiovascular System: Immediate, Intermediate, and Long-Term ComplicationsFabian Sanchis-GomarNo ratings yet
- Basic Training Logbook HKCCCNDocument19 pagesBasic Training Logbook HKCCCNSANTOSH KUMAR BHASKARNo ratings yet
- Metaanalisis AfricaDocument14 pagesMetaanalisis AfricaRosy AlcayagaNo ratings yet
- Pogona Vitticeps) Nannizziopsis GuarroiDocument8 pagesPogona Vitticeps) Nannizziopsis GuarroiAkın SeverNo ratings yet
- Erata Ghid PDFDocument2 pagesErata Ghid PDFAna-Maria MihalceaNo ratings yet
- Advantages and Disadvantages of Aphakics Correction, Types of Aphakic Correction, Problems of Newly Corrected AphakicsDocument78 pagesAdvantages and Disadvantages of Aphakics Correction, Types of Aphakic Correction, Problems of Newly Corrected AphakicsTika100% (1)
- Pedia 102 MIDTERM EXAMSDocument15 pagesPedia 102 MIDTERM EXAMSquidditch07No ratings yet
- Introduction Clinical Pharmacology 9th Visovsky Test BankDocument6 pagesIntroduction Clinical Pharmacology 9th Visovsky Test BanksonyaaaqNo ratings yet
- Review Utbk 2019 KE-5: Bahasa InggrisDocument1 pageReview Utbk 2019 KE-5: Bahasa InggrisRyanGonzalesNo ratings yet
- Visual Diagnosis and Traditional Chinese Medicine: Face Reading - What Your Face SaysDocument8 pagesVisual Diagnosis and Traditional Chinese Medicine: Face Reading - What Your Face SaysTaniaNo ratings yet
- Learning Medicine - 1.0Document206 pagesLearning Medicine - 1.0Henry Leroy Lewis BatresNo ratings yet
- SHO Paper 2Document9 pagesSHO Paper 2Kenny Low100% (1)
- MCQ Internal MedicineDocument16 pagesMCQ Internal Medicinemohamed mowafey100% (2)
- SFL Joining KitDocument11 pagesSFL Joining Kitdharam singhNo ratings yet
- Food Poisoning N AMOEBIASIS - LECTUREDocument60 pagesFood Poisoning N AMOEBIASIS - LECTUREpriyanka100% (1)
- Tropical Veterinary Science: Ready Today For TomorrowDocument8 pagesTropical Veterinary Science: Ready Today For TomorrowEsdinawan Carakantara SatrijaNo ratings yet
- What Is The Difference Between Perception and PerspectiveDocument4 pagesWhat Is The Difference Between Perception and Perspectivebday23100% (1)
- Sweet DeathDocument5 pagesSweet DeathJBNo ratings yet
- Savage Worlds - Unofficial New HindrancesDocument3 pagesSavage Worlds - Unofficial New HindrancesLeandro MandoNo ratings yet
- "Sex The Gift in Body Languge That Sells". Janessa Jordan-RowellDocument46 pages"Sex The Gift in Body Languge That Sells". Janessa Jordan-RowellSenderoNo ratings yet
- Disfunctional Vascular Endothelium As A Driver of Atherosclerosis - Emergind Insights Into Pathogenesis and Treatment 2021Document18 pagesDisfunctional Vascular Endothelium As A Driver of Atherosclerosis - Emergind Insights Into Pathogenesis and Treatment 2021Camila VidigalNo ratings yet
- Biostat 2020 62 QDocument270 pagesBiostat 2020 62 Q'محمد علي' محمد لافيNo ratings yet
- Nursing Care Plan HyperthyroidismDocument2 pagesNursing Care Plan Hyperthyroidismderic76% (17)
- Inborn Errors of MetabolismDocument12 pagesInborn Errors of Metabolismmichelle octavianiNo ratings yet
- Congenital Adrenal Hyperplasia - Peds - PresentationDocument24 pagesCongenital Adrenal Hyperplasia - Peds - PresentationAditya ChhabraNo ratings yet
- Role of A Nurse in COVID-19 PandemicDocument6 pagesRole of A Nurse in COVID-19 PandemicMARYAM AL-KADHIM100% (3)
- CB Insights - Digital Health 150 2020Document15 pagesCB Insights - Digital Health 150 2020nikhil karthikeyanNo ratings yet
- Cloze Test: Complete The Text Wtih The Correct WordsDocument2 pagesCloze Test: Complete The Text Wtih The Correct WordsSo ToysNo ratings yet
- Treatment Program Special PDLDocument43 pagesTreatment Program Special PDLCriminegrology TvNo ratings yet
- Certificate Course in Meditation and Yoga Sciences: Subject CodeDocument3 pagesCertificate Course in Meditation and Yoga Sciences: Subject CodeGaurav PrakashNo ratings yet
- Head TraumaDocument22 pagesHead TraumaEllsay AliceNo ratings yet