You might also like
- Living on the Frontline of COVID-19 in MCO And CMCOFrom EverandLiving on the Frontline of COVID-19 in MCO And CMCONo ratings yet
- Novel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited SettingsDocument8 pagesNovel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited Settingsdiah Bayu siswantiNo ratings yet
- COVID-19 and Ophthalmology: A New Chapter in An Old Story: Me H D IDocument3 pagesCOVID-19 and Ophthalmology: A New Chapter in An Old Story: Me H D IasdfNo ratings yet
- Annals of Medicine and Surgery: Muhammad Anis Baskara, Firdian Makrufardi, Ardiana DinisariDocument4 pagesAnnals of Medicine and Surgery: Muhammad Anis Baskara, Firdian Makrufardi, Ardiana Dinisarialfan MaulanaNo ratings yet
- Name: Ikhtiara Fakhrunisa Class: X MIPA 5 Date: Wednesday, 26 Maret 2020 Text Report About InventionDocument2 pagesName: Ikhtiara Fakhrunisa Class: X MIPA 5 Date: Wednesday, 26 Maret 2020 Text Report About InventionIkhtiaraNo ratings yet
- Infection Prevention Strategies For Novel Coronavirus in Pregnant and Puerperal WomenDocument4 pagesInfection Prevention Strategies For Novel Coronavirus in Pregnant and Puerperal WomenEditor IJTSRDNo ratings yet
- Impact of Coronavirus (COVID-19) On Otolaryngologic Surgery: Brief CommentaryDocument8 pagesImpact of Coronavirus (COVID-19) On Otolaryngologic Surgery: Brief CommentaryHesbon MomanyiNo ratings yet
- Managing Covid 19 Patients Nurses Role and ConsiderationsDocument7 pagesManaging Covid 19 Patients Nurses Role and ConsiderationsSimona Marcela ȚibuleacNo ratings yet
- Main 9Document11 pagesMain 9Eltohn JohnNo ratings yet
- Clinical Immunology: Review ArticleDocument9 pagesClinical Immunology: Review ArticleSimon Peter SiansakaNo ratings yet
- Detection of Sars-Cov-2 in The Tears and Conjunctival Secretions of Coronavirus Disease 2019 PatientsDocument5 pagesDetection of Sars-Cov-2 in The Tears and Conjunctival Secretions of Coronavirus Disease 2019 PatientssofiaNo ratings yet
- Simple Economical Solution For Personal Protection Equipment (Face Mask/Shield) For Health Care Staff During COVID 19Document7 pagesSimple Economical Solution For Personal Protection Equipment (Face Mask/Shield) For Health Care Staff During COVID 19Neel PatelNo ratings yet
- Novel CoronavirusDocument7 pagesNovel CoronavirusMustafa KhudhairNo ratings yet
- Guidelines For The Management of COVID-19 in Health FacilitiesDocument35 pagesGuidelines For The Management of COVID-19 in Health FacilitiesherathhmasNo ratings yet
- Informe de La OMS Sobre El CoronavirusDocument3 pagesInforme de La OMS Sobre El CoronavirusTodo NoticiasNo ratings yet
- Impact of Lockdown During COVID-19 Pandemic and Its AdvantagesDocument6 pagesImpact of Lockdown During COVID-19 Pandemic and Its AdvantagesFI WahabNo ratings yet
- Dr. Dian Nurul Al Amini, SP - THTDocument6 pagesDr. Dian Nurul Al Amini, SP - THTRifaniNugrohoNo ratings yet
- COVID-19: A Quick Look at Aspects of Critical CareDocument5 pagesCOVID-19: A Quick Look at Aspects of Critical CareJbarrianNo ratings yet
- Jamaotolaryngology Givi 2020 SC 200001Document6 pagesJamaotolaryngology Givi 2020 SC 200001dina ayu SeptianiNo ratings yet
- Current Situation of Coronavirus Disease Covid19 Review ArticleDocument4 pagesCurrent Situation of Coronavirus Disease Covid19 Review ArticleasuscribdNo ratings yet
- COVID-19 Pathology Accepted PrePrintDocument26 pagesCOVID-19 Pathology Accepted PrePrintamimuNo ratings yet
- Covid 19: Rajni SharmaDocument33 pagesCovid 19: Rajni SharmaJuan CruzNo ratings yet
- COVID 19 Lessons in Laboratory MedicineDocument8 pagesCOVID 19 Lessons in Laboratory MedicinegygyNo ratings yet
- Lai2020 Article SteppingUpInfectionControlMeasDocument7 pagesLai2020 Article SteppingUpInfectionControlMeasretnoNo ratings yet
- Print 2Document7 pagesPrint 2ridawahyuni09No ratings yet
- Covid Disease 2019Document1 pageCovid Disease 2019Rolando NABUSNo ratings yet
- 2021 Published Medicina 57 00189Document10 pages2021 Published Medicina 57 00189Healthcare Pro LearningNo ratings yet
- COVID-19 in Pregnancy-Review of Guidelines in Indian Setting From The Point of View of Community HealthDocument6 pagesCOVID-19 in Pregnancy-Review of Guidelines in Indian Setting From The Point of View of Community HealthifaNo ratings yet
- Epidemiology and Clinical Characteristics of COVID-19: MedicineDocument4 pagesEpidemiology and Clinical Characteristics of COVID-19: MedicineAlexRázuriNo ratings yet
- The Role of Masks and Respirator Protection Against Sars-Cov-2Document2 pagesThe Role of Masks and Respirator Protection Against Sars-Cov-2Esther Margaretha YolandaNo ratings yet
- A Review of The Management and Safe Handling of Bodies in Cases Involving COVID-19Document7 pagesA Review of The Management and Safe Handling of Bodies in Cases Involving COVID-19Muhammad RaflirNo ratings yet
- 10 1111@anae 15054 PDFDocument33 pages10 1111@anae 15054 PDFJuliana Rodriguez MariñoNo ratings yet
- PROJETDocument4 pagesPROJETLéon RasolonjatovoNo ratings yet
- COVID-19 Pathology Accepted PrePrint PDFDocument25 pagesCOVID-19 Pathology Accepted PrePrint PDFkambangNo ratings yet
- Rehab and CovidDocument10 pagesRehab and CovidMariana BarrosNo ratings yet
- COVID-19 - Diagnosis - UpToDateDocument34 pagesCOVID-19 - Diagnosis - UpToDateDuy Hùng HoàngNo ratings yet
- Comment: S R e TDocument3 pagesComment: S R e TIvana MayacantikaNo ratings yet
- A Comprehensive Literature Review On The Clinical Presentation, and Management of The Pandemic Coronavirus Disease 2019 (COVID-19)Document18 pagesA Comprehensive Literature Review On The Clinical Presentation, and Management of The Pandemic Coronavirus Disease 2019 (COVID-19)Zihan Zetira100% (1)
- Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease Is SuspectedDocument19 pagesClinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease Is SuspectedgustixNo ratings yet
- Review: Coronavirus Disease 2019 (COVID-19) : Latest Developments in Potential TreatmentsDocument14 pagesReview: Coronavirus Disease 2019 (COVID-19) : Latest Developments in Potential Treatmentsjenny12No ratings yet
- AABIP Statement on Bronchoscopy and COVID-19 Specimen CollectionDocument5 pagesAABIP Statement on Bronchoscopy and COVID-19 Specimen Collectiongarinda almadutaNo ratings yet
- Joim 13091Document15 pagesJoim 13091sarabisimonaNo ratings yet
- COVID 19 An Emerging Coronavirus Infection Advances and Prospects in Designing and Developing Vaccines Immunotherapeutics and TherapeuticsDocument8 pagesCOVID 19 An Emerging Coronavirus Infection Advances and Prospects in Designing and Developing Vaccines Immunotherapeutics and TherapeuticsCertaf MaghnjaNo ratings yet
- Published ArticleDocument5 pagesPublished ArticleJoice RumondangNo ratings yet
- Coronavirus Disease 2019 COVID-19 Latest DevelopmeDocument15 pagesCoronavirus Disease 2019 COVID-19 Latest DevelopmeWarner LlaveNo ratings yet
- Pedoman Standar Perlindungan Dokter - TIM MITIGASI 23 Sep 2020Document57 pagesPedoman Standar Perlindungan Dokter - TIM MITIGASI 23 Sep 2020Melati SatriasNo ratings yet
- COVID-19 Diagnosis and Management ReviewDocument15 pagesCOVID-19 Diagnosis and Management ReviewOscar Oswaldo SCNo ratings yet
- COVID-19 Patient Friendly EbookDocument55 pagesCOVID-19 Patient Friendly EbookYarmand WaqarNo ratings yet
- The Journal of Pharmaceutical Sciences and Medicinal ResearchDocument20 pagesThe Journal of Pharmaceutical Sciences and Medicinal Researchjaypharma111No ratings yet
- Infectious Pneumonia in The Immunocompetent Host: What The Radiologist Should KnowDocument10 pagesInfectious Pneumonia in The Immunocompetent Host: What The Radiologist Should KnowAgung AbdurrahmanNo ratings yet
- COVID 19 Guideline To Resume Paediatric Dental Services in MalaysiaDocument29 pagesCOVID 19 Guideline To Resume Paediatric Dental Services in MalaysiaEnrita DianNo ratings yet
- COVID 19PartI IP2020Document12 pagesCOVID 19PartI IP2020hanady shehataNo ratings yet
- Covid-19 by Md. Masum BillalDocument7 pagesCovid-19 by Md. Masum BillalMd. Masum BillalNo ratings yet
- JObstetAnaesthCritCare10269-2682971 072709 PDFDocument6 pagesJObstetAnaesthCritCare10269-2682971 072709 PDFMuhammad RenaldiNo ratings yet
- Letter To The Editor: Neonatal Coronavirus Disease-2019: Presentation and ManagementDocument3 pagesLetter To The Editor: Neonatal Coronavirus Disease-2019: Presentation and ManagementadeNo ratings yet
- Resolution of Coronavirus Disease 2019 COVID 19Document12 pagesResolution of Coronavirus Disease 2019 COVID 19Job GonzagaNo ratings yet
- Coronavirus Disease 2019 COVID-19 Latest DevelopmeDocument15 pagesCoronavirus Disease 2019 COVID-19 Latest DevelopmeNHÂN LÊNo ratings yet
- Vol 28 2 2020 10Document14 pagesVol 28 2 2020 10Nanang SupriyantoNo ratings yet
- Management of COVID-19 From The Pulmonologist's Perspective: A Narrative ReviewDocument18 pagesManagement of COVID-19 From The Pulmonologist's Perspective: A Narrative ReviewLOLOLONo ratings yet
- Influenza Virus 2021Document6 pagesInfluenza Virus 2021cdsaludNo ratings yet
- #Helmet and NoninvasiveDocument14 pages#Helmet and NoninvasiveHanni HarahapNo ratings yet
- Antonelli2019 Article NIVThroughTheHelmetCanBeUsedAsDocument3 pagesAntonelli2019 Article NIVThroughTheHelmetCanBeUsedAsHanni HarahapNo ratings yet
- Mechanical Ventilation Learning Package: Sharon-Ann Shunker, CNC, Liverpool ICU SWSLHD 2/3/2016Document75 pagesMechanical Ventilation Learning Package: Sharon-Ann Shunker, CNC, Liverpool ICU SWSLHD 2/3/2016Hanni HarahapNo ratings yet
- (Rev. 3) Positive Ending Expiratory Pressure ValveDocument9 pages(Rev. 3) Positive Ending Expiratory Pressure ValveHanni HarahapNo ratings yet
- Experimental Techniques PDFDocument31 pagesExperimental Techniques PDFHanni HarahapNo ratings yet
- S5 - Noise MeasurementsDocument41 pagesS5 - Noise MeasurementsHanni HarahapNo ratings yet
- Pud Case StudyDocument6 pagesPud Case Studyapi-302326926100% (1)
- Clinical Laboratory Biosafety: Tapeshwar Yadav (Lecturer)Document26 pagesClinical Laboratory Biosafety: Tapeshwar Yadav (Lecturer)Tapeshwar YadavNo ratings yet
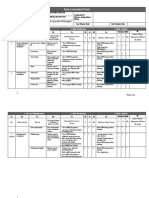
- Lim Meng Heck (SR - Operation Manager) : ISK Ssessment ORMDocument2 pagesLim Meng Heck (SR - Operation Manager) : ISK Ssessment ORMVaradaraju ThirunavukkarasanNo ratings yet
- National Children's Science Congress: NCSC 2022 and 2023 Focal Theme and Sub-ThemesDocument11 pagesNational Children's Science Congress: NCSC 2022 and 2023 Focal Theme and Sub-ThemesnkhiangteNo ratings yet
- OET Nursing Case Notes: Introducing Maeve GreersonDocument2 pagesOET Nursing Case Notes: Introducing Maeve GreersonLigy GeorgeNo ratings yet
- Learning ObjectivesDocument6 pagesLearning Objectivesangot123No ratings yet
- Tujuan DietDocument3 pagesTujuan DietKecengNo ratings yet
- Daconil 720 SC: Safety Data SheetDocument9 pagesDaconil 720 SC: Safety Data SheetAngelicaNo ratings yet
- Upw WorkbookDocument109 pagesUpw WorkbookAdriana SuruNo ratings yet
- How to Get a Good Night's Sleep: Tips for Managing InsomniaDocument24 pagesHow to Get a Good Night's Sleep: Tips for Managing InsomniaUm ArNo ratings yet
- Qol SonDocument3 pagesQol Sonpermana0adityaNo ratings yet
- Birth asphyxia causes and neonatal resuscitationDocument20 pagesBirth asphyxia causes and neonatal resuscitationinne_fNo ratings yet
- Mental Health EssayDocument2 pagesMental Health EssayROHITNo ratings yet
- Case Write Up - Dengue FeverDocument22 pagesCase Write Up - Dengue FevervijayaNo ratings yet
- Complication of Hemodialysis and Their ManagementDocument52 pagesComplication of Hemodialysis and Their ManagementRetno SumaraNo ratings yet
- Diabetes Type 2 BasicsDocument44 pagesDiabetes Type 2 BasicsMasunji EmanuelNo ratings yet
- Đề Thi Thử Thptqg Môn Tiếng AnhDocument8 pagesĐề Thi Thử Thptqg Môn Tiếng AnhHổCápNo ratings yet
- Gastroesophageal Reflux Disease (GERD) : Patient Population: Objective: Key PointsDocument12 pagesGastroesophageal Reflux Disease (GERD) : Patient Population: Objective: Key PointsRavindraNo ratings yet
- Boore, CarolineDocument287 pagesBoore, CarolineAmarshanaNo ratings yet
- Steps To Prevent Drug AddictionDocument9 pagesSteps To Prevent Drug AddictionLuna DizonNo ratings yet
- The Family Doctor - Prof. Henry S Taylor, M.D., 1860Document324 pagesThe Family Doctor - Prof. Henry S Taylor, M.D., 1860IreneRainsNo ratings yet
- I. Essay Questions: (2 X 20 40) : M.D. (Homeopathy) Degree Examination - October 2013Document2 pagesI. Essay Questions: (2 X 20 40) : M.D. (Homeopathy) Degree Examination - October 2013amareshscribdNo ratings yet
- Gym PlanDocument56 pagesGym PlanAlize Ch0% (1)
- A Single-Arm Study To Evaluate The Transfer of Drospirenone To Breast Milk After Reaching Steady State, Following Oral Administration of 4 MG Drospirenone in Healthy Lactating Female VolunteersDocument7 pagesA Single-Arm Study To Evaluate The Transfer of Drospirenone To Breast Milk After Reaching Steady State, Following Oral Administration of 4 MG Drospirenone in Healthy Lactating Female VolunteersfadhilNo ratings yet
- Advance Endoscopy Assessment FormDocument2 pagesAdvance Endoscopy Assessment FormRomelia CampuzanoNo ratings yet
- Diabetes Care in Nigeria - 2015 - Annals of Global Health PDFDocument9 pagesDiabetes Care in Nigeria - 2015 - Annals of Global Health PDFarmanNo ratings yet
- Abnormal Psychology Beidel 3rd Edition Test BankDocument4 pagesAbnormal Psychology Beidel 3rd Edition Test BankChuck Simmons100% (25)
- Early Childhood CariesDocument13 pagesEarly Childhood Cariesrahul sharmaNo ratings yet
- Research Made EasyDocument74 pagesResearch Made EasygloriacunananNo ratings yet
- Dragon BoatDocument7 pagesDragon BoatandrewadrianNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (16)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- CBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerFrom EverandCBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- How To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeFrom EverandHow To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Inmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedFrom EverandInmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)