You might also like
- 325 FullDocument20 pages325 FullDessyadoeNo ratings yet
- 10096_2018_Article_3216Document7 pages10096_2018_Article_3216Betty YayaNo ratings yet
- Blood Culture Booklet - PRN 16 0097a 00 MK Approved13jul161Document36 pagesBlood Culture Booklet - PRN 16 0097a 00 MK Approved13jul161Thiody Hope LimosneroNo ratings yet
- tmpD1AB TMPDocument9 pagestmpD1AB TMPFrontiersNo ratings yet
- Blood Culture Key Investigations BookletDocument36 pagesBlood Culture Key Investigations BooklettahirinicoledNo ratings yet
- J. Clin. Microbiol.-2003-Weinstein-2275-8 - Blood Culture Contamination Persisting Problems and Partial Progress PDFDocument4 pagesJ. Clin. Microbiol.-2003-Weinstein-2275-8 - Blood Culture Contamination Persisting Problems and Partial Progress PDFmela renNo ratings yet
- Diagnosis of Blood and Bone Marrow DisordersFrom EverandDiagnosis of Blood and Bone Marrow DisordersSa A. WangNo ratings yet
- Actualización-Endocarditis-bacteriana AmJMed 2020Document6 pagesActualización-Endocarditis-bacteriana AmJMed 2020msq.cv5919No ratings yet
- J. Clin. Microbiol. 2011 Weinstein S26 9Document4 pagesJ. Clin. Microbiol. 2011 Weinstein S26 9Prakarsa Adi Daya NusantaraNo ratings yet
- Hyponatremia in Tuberculous MeningitisDocument11 pagesHyponatremia in Tuberculous MeningitisBelinda Putri agustiaNo ratings yet
- Lectura 3seminario Micosis ProfundaDocument8 pagesLectura 3seminario Micosis ProfundaSebastian CastroNo ratings yet
- Journal of Clinical Microbiology-2011-Wolk-S62.fullDocument6 pagesJournal of Clinical Microbiology-2011-Wolk-S62.fullAli AhmedNo ratings yet
- Cell-Based Therapy To Reduce Mortality From COVID-19Document16 pagesCell-Based Therapy To Reduce Mortality From COVID-19Chelsea Shannen Marie CarreonNo ratings yet
- Empiric Antimicrobial Therapy For BacteremiaDocument4 pagesEmpiric Antimicrobial Therapy For BacteremiamadengNo ratings yet
- JVECC Consensus Antithrombotics Main DocumentDocument25 pagesJVECC Consensus Antithrombotics Main DocumentTzu YinNo ratings yet
- Spondt (Spondylodiscitis Diagnosis and Treatment) : Spondylodiscitis Scoring SystemDocument8 pagesSpondt (Spondylodiscitis Diagnosis and Treatment) : Spondylodiscitis Scoring SystemZak harNo ratings yet
- 10 1016@j Jaad 2019 05 096Document8 pages10 1016@j Jaad 2019 05 096JohnNo ratings yet
- TBC y Shock SepticoDocument9 pagesTBC y Shock Septicogiseladelarosa2006No ratings yet
- 1 s2.0 S0002934322007227 MainDocument8 pages1 s2.0 S0002934322007227 MainMaryatiNo ratings yet
- Sepsis Therapies: Learning From 30 Years of Failure of Translational Research To Propose New LeadsDocument24 pagesSepsis Therapies: Learning From 30 Years of Failure of Translational Research To Propose New LeadsMark TomNo ratings yet
- Cryptococcal Infection in Plhiv: Series of 12 Cases at The Laboratory of Mohammed Vi University Hospital of MarrakechDocument6 pagesCryptococcal Infection in Plhiv: Series of 12 Cases at The Laboratory of Mohammed Vi University Hospital of MarrakechIJAR JOURNALNo ratings yet
- CREMJHIDDocument9 pagesCREMJHIDAnggy de RinconNo ratings yet
- Clinico-Microbiological Spectrum of Hemodialysis Catheter-Related Blood Stream Infections: A Concise ReviewDocument7 pagesClinico-Microbiological Spectrum of Hemodialysis Catheter-Related Blood Stream Infections: A Concise ReviewIJAR JOURNALNo ratings yet
- Jama Neal 2023 Ed 230070 1696973944.14124Document2 pagesJama Neal 2023 Ed 230070 1696973944.14124Luz Elena ValderramaNo ratings yet
- Jurnal PilihanDocument7 pagesJurnal PilihanNovia khasanahNo ratings yet
- Respiratory and Pulmonary Medicine: ClinmedDocument3 pagesRespiratory and Pulmonary Medicine: ClinmedGrace Yuni Soesanti MhNo ratings yet
- Urosepsis PDFDocument14 pagesUrosepsis PDFYudi SiswantoNo ratings yet
- Diagnose of BSIDocument12 pagesDiagnose of BSIWong Chun ShengNo ratings yet
- 803 FullDocument8 pages803 FullYud yaoNo ratings yet
- AAFP SepsisDocument13 pagesAAFP SepsisANISA RACHMITA ARIANTI 2020No ratings yet
- PIIS1201971218345090Document9 pagesPIIS1201971218345090favorendaNo ratings yet
- Culture Negative IsDocument29 pagesCulture Negative IsvinobapsNo ratings yet
- Celebrating 70 Years of the Hungarian Society of Laboratory MedicineDocument9 pagesCelebrating 70 Years of the Hungarian Society of Laboratory MedicineRiski Nur RamadhaniNo ratings yet
- De PrintatDocument24 pagesDe PrintatDJ ATBNo ratings yet
- Review On Blood Culture: Anup R Warrier, Mathew ThomasDocument3 pagesReview On Blood Culture: Anup R Warrier, Mathew Thomaspurnima4uonlyNo ratings yet
- Espondilodiscitis Infecciosa Por Patógenos Poco ComunesDocument5 pagesEspondilodiscitis Infecciosa Por Patógenos Poco ComunesOthoniel RamirezNo ratings yet
- Antimicrob. Agents Chemother.-2017-GrossmanDocument12 pagesAntimicrob. Agents Chemother.-2017-GrossmanGUSTAVO FREITASNo ratings yet
- Chaves 2005 PDFDocument5 pagesChaves 2005 PDFWa Nur Arlin RahmadhantyNo ratings yet
- SMW 09797 PDFDocument9 pagesSMW 09797 PDFEJ AguilarNo ratings yet
- Diagnostic Approach for PancytopeniaDocument7 pagesDiagnostic Approach for PancytopeniaDani BelloNo ratings yet
- Guizzetti - 2016Document10 pagesGuizzetti - 2016Bogdan TrandafirNo ratings yet
- Infective Endocarditis GuideDocument201 pagesInfective Endocarditis GuideAbnet WondimuNo ratings yet
- kern2003 (1)Document8 pageskern2003 (1)Eryc Luan DiasNo ratings yet
- (Methods in Molecular Medicine) Andrew J. Pollard, Martin C.J. Maiden - Meningococcal Disease (2001, Humana Press)Document662 pages(Methods in Molecular Medicine) Andrew J. Pollard, Martin C.J. Maiden - Meningococcal Disease (2001, Humana Press)gnkgbjkgjkNo ratings yet
- Lactate in Sepsis PDFDocument8 pagesLactate in Sepsis PDFAngela PuspitaNo ratings yet
- My Publication EpjmrDocument7 pagesMy Publication EpjmrMd. ImranNo ratings yet
- Blood Culture: A Key Investigation FORDocument19 pagesBlood Culture: A Key Investigation FORJordan Alvarez Toro100% (1)
- Celullitis JAMA. 2016Document13 pagesCelullitis JAMA. 2016J Pablo Giles ZamNo ratings yet
- Asj-2020-0262tbc o Brucella ImglesDocument8 pagesAsj-2020-0262tbc o Brucella ImglesThais LudenaNo ratings yet
- Infectious Endocarditis: Diagnosis and TreatmentDocument6 pagesInfectious Endocarditis: Diagnosis and TreatmentMelissa Aina Mohd YusofNo ratings yet
- COHORT - TB MenigealDocument11 pagesCOHORT - TB MenigealYA MAAPNo ratings yet
- International Journal of Surgery Case ReportsDocument5 pagesInternational Journal of Surgery Case ReportsJayzel LaureanoNo ratings yet
- Ciz 1049Document9 pagesCiz 1049Justin WilliemNo ratings yet
- Medical Mycology Case ReportsDocument4 pagesMedical Mycology Case ReportsSebastián Garay HuertasNo ratings yet
- Systematic Review On Risk Factors Related To Central Venous Catheter InfectionDocument18 pagesSystematic Review On Risk Factors Related To Central Venous Catheter InfectionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fimmu 13 900594Document11 pagesFimmu 13 900594Troy Prasi Fajagutana AvelinoNo ratings yet
- Hemodialysis Catheter-Related Bloodstream InfectionsDocument7 pagesHemodialysis Catheter-Related Bloodstream InfectionsHGZ 83 MoreliaNo ratings yet
- 1Document2 pages1Srinath M VNo ratings yet
- Jurnal Interna 123456Document9 pagesJurnal Interna 123456vonnyandira28No ratings yet
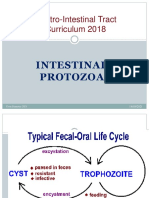
- Intestinal Protozoa 2021Document50 pagesIntestinal Protozoa 2021DragnosNo ratings yet
- 590S10Cest2 PDFDocument31 pages590S10Cest2 PDFmuhammad nurhadiNo ratings yet
- Materi Trombosis Untuk Mahasiswa (Desember 2020)Document78 pagesMateri Trombosis Untuk Mahasiswa (Desember 2020)DragnosNo ratings yet
- Infectious EndocarditisDocument49 pagesInfectious EndocarditisDennisFrankKondoNo ratings yet
- Anti AnginaDocument42 pagesAnti AnginaDragnosNo ratings yet
- Attachment Lab ReportsDocument43 pagesAttachment Lab ReportsEVANS ELCANAH33% (6)
- Preparing and Writing Research Proposals: © C.P.P. Reid, Univ. Arizona M. Kleine, IUFRO-SPDC Update 2004Document226 pagesPreparing and Writing Research Proposals: © C.P.P. Reid, Univ. Arizona M. Kleine, IUFRO-SPDC Update 2004Kumeydi SheekaaNo ratings yet
- Esmat Khaled Allam: Key Words: Potato, Wild-Type, PSTVDDocument10 pagesEsmat Khaled Allam: Key Words: Potato, Wild-Type, PSTVDhishoNo ratings yet
- Complete MCQ ,.,.Document35 pagesComplete MCQ ,.,.shoaibjan4916765No ratings yet
- All in Trans Molecular BiologyDocument12 pagesAll in Trans Molecular BiologyCASTILLO, ANGELA ALEXA A.No ratings yet
- QF-PCR Best Practice GuidelinesDocument11 pagesQF-PCR Best Practice GuidelinesSandeep SharmaNo ratings yet
- Truenat HLA-B27 Packinsert VER-04Document4 pagesTruenat HLA-B27 Packinsert VER-04yousra zeidanNo ratings yet
- 7-Mycobacterium Avium SubspDocument3 pages7-Mycobacterium Avium Subspreadyboy89No ratings yet
- Van Schie RC Wilson ME: J Immunol MethodsDocument9 pagesVan Schie RC Wilson ME: J Immunol MethodsGAURAVNo ratings yet
- Insight and Control of Infectious Disease in Global Scenario - P. Roy (Intech, 2012) WWDocument454 pagesInsight and Control of Infectious Disease in Global Scenario - P. Roy (Intech, 2012) WWgoutham sivasailamNo ratings yet
- Genetic Engineering: Unit 3Document60 pagesGenetic Engineering: Unit 3blackmoneygrabberNo ratings yet
- Protocol: Genetisure Pre-Screen Kit For Single Cell AnalysisDocument70 pagesProtocol: Genetisure Pre-Screen Kit For Single Cell AnalysisS CNo ratings yet
- Biochemistry Lab Review UNTDocument4 pagesBiochemistry Lab Review UNTSue WalthersNo ratings yet
- Gallaeformans Ditylenchus Sp.Document18 pagesGallaeformans Ditylenchus Sp.Edgar Medina GomezNo ratings yet
- Water RelatedDocument15 pagesWater RelatedMix Content789No ratings yet
- Cell, Vol. 90, 19-30, July 11, 1997, Copyright ©1997 byDocument12 pagesCell, Vol. 90, 19-30, July 11, 1997, Copyright ©1997 byjohnny cartinNo ratings yet
- Detecting Equine Infectious AnaemiaDocument6 pagesDetecting Equine Infectious AnaemiaWormInchNo ratings yet
- 1808 1657 Aib 85 e0712016MolecularstudiesonAfricanswineDocument9 pages1808 1657 Aib 85 e0712016MolecularstudiesonAfricanswinebotond77No ratings yet
- EDocument72 pagesECedric Kanyinda0% (1)
- 1 SMDocument12 pages1 SMyowyowNo ratings yet
- Antibiotic Resistance in A Predominantly OccurringDocument11 pagesAntibiotic Resistance in A Predominantly OccurringmaaahiiNo ratings yet
- Polymerase Chain Reaction - WikipediaDocument36 pagesPolymerase Chain Reaction - Wikipedia93428ZEFHDNo ratings yet
- Molecular DiagnosticsDocument583 pagesMolecular DiagnosticsAnthony93% (14)
- Advanced Diagnostic TechniquesDocument19 pagesAdvanced Diagnostic TechniquesSunkara Musalaiah0% (1)
- Chapter 17 - Laboratory Testing and Diagnostics - APIC Text OnlineDocument10 pagesChapter 17 - Laboratory Testing and Diagnostics - APIC Text OnlineManalAbdelazizNo ratings yet
- Jeon2019 (Microbial Production of Sebacic Acid From A Renewable Source - Production, Purification, and Polymerization)Document11 pagesJeon2019 (Microbial Production of Sebacic Acid From A Renewable Source - Production, Purification, and Polymerization)Byounghak KimNo ratings yet
- Rich Protein in Soybean (Glycine Max) Cotyledon. Purification and Gene Cloning Ma. Jamela R. Revilleza, Alfred Galvez, Deanne C. Krenz, Et Al. 1999Document12 pagesRich Protein in Soybean (Glycine Max) Cotyledon. Purification and Gene Cloning Ma. Jamela R. Revilleza, Alfred Galvez, Deanne C. Krenz, Et Al. 1999ponbohacopNo ratings yet
- DNA Fingerprinting ProcessDocument3 pagesDNA Fingerprinting ProcessSelvaraju Parthibhan100% (1)
- Comparison of Proteases in DNA Extraction Via QPCRDocument3 pagesComparison of Proteases in DNA Extraction Via QPCRWiki PediaNo ratings yet
- GENE THERAPY FOR SICKLE CELL DISEASE by Adeleye Abayomi (Seminar Report) - CORRECTIONS ADAPTEDDocument54 pagesGENE THERAPY FOR SICKLE CELL DISEASE by Adeleye Abayomi (Seminar Report) - CORRECTIONS ADAPTEDFayomi JosephNo ratings yet