You might also like
- Microcirculation in Cardiovascular DiseasesFrom EverandMicrocirculation in Cardiovascular DiseasesEnrico Agabiti-RoseiNo ratings yet
- AnotherDocument11 pagesAnotherTudor DumitrascuNo ratings yet
- Mitral Annular Disjunction: A Systematic Review of The LiteratureDocument10 pagesMitral Annular Disjunction: A Systematic Review of The LiteratureAlznoskillNo ratings yet
- Surgery 1Document14 pagesSurgery 1Pau MendozaNo ratings yet
- Syntax ScoreDocument10 pagesSyntax ScoreInggitaDarmawanNo ratings yet
- Evidence-Based Diagnosis and Management of Chronic Subdural HematomaDocument9 pagesEvidence-Based Diagnosis and Management of Chronic Subdural HematomaJorge MontenegroNo ratings yet
- Mitral Valve Disease-Current Management and Future ChallengesDocument11 pagesMitral Valve Disease-Current Management and Future ChallengesjuanpbagurNo ratings yet
- Connective Tissue Diseases: Focus On Microcirculatory Bed: O.I. Zarudna, I.K. Venher, A.V. DovbushDocument8 pagesConnective Tissue Diseases: Focus On Microcirculatory Bed: O.I. Zarudna, I.K. Venher, A.V. DovbushdjdNo ratings yet
- Laboratory Diagnosis of Infective 2017Document10 pagesLaboratory Diagnosis of Infective 2017DragnosNo ratings yet
- Prevalence of Anatomical Variations of Circle of Willis in South Indian Population Succumbing To Isolated Traumatic Brain Injury - A Cadaveric StudyDocument6 pagesPrevalence of Anatomical Variations of Circle of Willis in South Indian Population Succumbing To Isolated Traumatic Brain Injury - A Cadaveric StudyIJAR JOURNALNo ratings yet
- Chronic Myeloid Leukemia: Chronic Phase Presenting As Extramedullary PresentationDocument6 pagesChronic Myeloid Leukemia: Chronic Phase Presenting As Extramedullary PresentationOjas MahajanNo ratings yet
- Atm 08 23 1626Document12 pagesAtm 08 23 1626Susana MalleaNo ratings yet
- Surgical Anatomy of Thyroid and Incidence of Malignancy in Solitary Nodule of ThyroidDocument7 pagesSurgical Anatomy of Thyroid and Incidence of Malignancy in Solitary Nodule of ThyroidFloyd balansagNo ratings yet
- OMICS Journal of Radiology: Pulmonary Hypertension Secondary To Cardiac Hydatid Cyst EmbolismDocument2 pagesOMICS Journal of Radiology: Pulmonary Hypertension Secondary To Cardiac Hydatid Cyst EmbolismAgusNo ratings yet
- Journal NeuroDocument6 pagesJournal NeuroBetari DhiraNo ratings yet
- Infectious Endo Carditis With Sub Aortic Diapharagma in A Patient With Coarctation of The AortaDocument3 pagesInfectious Endo Carditis With Sub Aortic Diapharagma in A Patient With Coarctation of The AortaIJAR JOURNALNo ratings yet
- Mitral Stenosis 2Document4 pagesMitral Stenosis 2Mai Nguyễn Thị NgọcNo ratings yet
- Short - and Long-Term Outcomes at A Single InstitutionDocument7 pagesShort - and Long-Term Outcomes at A Single InstitutionJonathan Frimpong AnsahNo ratings yet
- MNJ ToastDocument4 pagesMNJ ToastRichard SuherlimNo ratings yet
- Ajc 10018 Review GunerDocument11 pagesAjc 10018 Review GunerMaria Goretty L. TobingNo ratings yet
- International Journal of Surgery Case ReportsDocument6 pagesInternational Journal of Surgery Case ReportsUmar UsmanNo ratings yet
- gs-10-03-1135Document12 pagesgs-10-03-1135Ashu AberaNo ratings yet
- Eufred Study Results: Progressive Occlusion Increases Over Time Ive Occlusion Increases ODocument20 pagesEufred Study Results: Progressive Occlusion Increases Over Time Ive Occlusion Increases OUssiy RachmanNo ratings yet
- Articulo 8Document7 pagesArticulo 8Marcela RodriguezNo ratings yet
- Ajc 16 12 980 989Document10 pagesAjc 16 12 980 989Maria Goretty L. TobingNo ratings yet
- Bone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyDocument4 pagesBone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyivanNo ratings yet
- Mitral Valve Endocarditis in Hypertrophic Cardiomyopathy: Case Report and Literature ReviewDocument3 pagesMitral Valve Endocarditis in Hypertrophic Cardiomyopathy: Case Report and Literature ReviewChristabella Natalia WijayaNo ratings yet
- SilotoraksDocument8 pagesSilotoraksFitri Amelia RizkiNo ratings yet
- Standard Treatment Guidelines Interventional Radiology: Ministry of Health & Family Welfare Govt. of IndiaDocument75 pagesStandard Treatment Guidelines Interventional Radiology: Ministry of Health & Family Welfare Govt. of IndiaKaustubhNo ratings yet
- Lower Extremity Artery Aneurysms and Their Management-An Institutional ExperienceDocument8 pagesLower Extremity Artery Aneurysms and Their Management-An Institutional ExperienceIJAR JOURNALNo ratings yet
- 1-s2.0-S187864802200444X-mainDocument2 pages1-s2.0-S187864802200444X-mainade lydia br.siregarNo ratings yet
- Rheumatic Mitral Valve Surgery: About 1025 Cases: Original Research ArticleDocument7 pagesRheumatic Mitral Valve Surgery: About 1025 Cases: Original Research ArticleThanh BinhNo ratings yet
- Full Length Research Article: ISSN: 2230-9926Document2 pagesFull Length Research Article: ISSN: 2230-9926Avik singhNo ratings yet
- Acute Ischaemic Stroke in Infective Endocarditis: Pathophysiology and Clinical Outcomes in Patients Treated With Reperfusion TherapyDocument13 pagesAcute Ischaemic Stroke in Infective Endocarditis: Pathophysiology and Clinical Outcomes in Patients Treated With Reperfusion TherapyPatrick NunsioNo ratings yet
- Clinicopathological Study of Varicose Veins (Descriptive Study)Document10 pagesClinicopathological Study of Varicose Veins (Descriptive Study)Vlad DraculaNo ratings yet
- Assessment of AtherosclerosisDocument10 pagesAssessment of AtherosclerosisCalysta CitraNo ratings yet
- Hot Topics in Tetralogy of FallotDocument12 pagesHot Topics in Tetralogy of FallotqanitaNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, KarnatakaDocument18 pagesRajiv Gandhi University of Health Sciences, Bangalore, KarnatakaprashantghodkeNo ratings yet
- Recommended.: Comment (I - (1) : MAJOR REVISION ISDocument7 pagesRecommended.: Comment (I - (1) : MAJOR REVISION ISBilal Khan MarwatNo ratings yet
- Frequency of Coronary Artery Disease in Valvular Aortic Stenosis :experience of The Cardiology Center of Mohamed V Military Hospital About 148 CasesDocument5 pagesFrequency of Coronary Artery Disease in Valvular Aortic Stenosis :experience of The Cardiology Center of Mohamed V Military Hospital About 148 CasesIJAR JOURNALNo ratings yet
- TurkeyGMJ 62 200 enDocument6 pagesTurkeyGMJ 62 200 enCocoNo ratings yet
- J Jacc 2022 09 044Document17 pagesJ Jacc 2022 09 044Ivan BitunjacNo ratings yet
- (RCT) Cardiovascular Injuries After Covid-19 InfectionDocument7 pages(RCT) Cardiovascular Injuries After Covid-19 InfectionPatrick NunsioNo ratings yet
- Clinical Determinants of CoronaryDocument82 pagesClinical Determinants of CoronarySitiMaghfirahHafizNo ratings yet
- Fana Alemseged Endovascular Thrombectomy For Basil - 231118 - 114208Document8 pagesFana Alemseged Endovascular Thrombectomy For Basil - 231118 - 114208Luis Guilherme ScalianteNo ratings yet
- 20221022-8547-Dc62ai Porcelon AortaDocument5 pages20221022-8547-Dc62ai Porcelon AortasaNo ratings yet
- Jurnal HDDocument6 pagesJurnal HDAdi SuciptoNo ratings yet
- A Study On Complications of Ventriculoperitoneal Shunt Surgery in Bir Hospital, Kathmandu, NepalDocument4 pagesA Study On Complications of Ventriculoperitoneal Shunt Surgery in Bir Hospital, Kathmandu, NepalHaziq AnuarNo ratings yet
- Bomba_de_flujo_microaxial_en_el_shock_cardiogénico_relacionado_conDocument12 pagesBomba_de_flujo_microaxial_en_el_shock_cardiogénico_relacionado_conAdrianaIDCNo ratings yet
- Endovascular Management of Acute Epidural Hematomas: Clinical Experience With 80 CasesDocument7 pagesEndovascular Management of Acute Epidural Hematomas: Clinical Experience With 80 CasesDeby AnditaNo ratings yet
- The Relationship Between Multimorbidity and Quality of Life On Acute Myocardial Infaction Patients Undergoing Percutaneous Coronary Intervention in Haji Adam Malik Hospital MedanDocument11 pagesThe Relationship Between Multimorbidity and Quality of Life On Acute Myocardial Infaction Patients Undergoing Percutaneous Coronary Intervention in Haji Adam Malik Hospital MedanInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pharm D (PB) 2 YEAR 2020-2021: Under The Guidance of GuideDocument41 pagesPharm D (PB) 2 YEAR 2020-2021: Under The Guidance of Guidesufiya fatimaNo ratings yet
- Midterm Outcomes of Minimally Invasive Mitral Valve Surgery in A Heterogeneous Valve Pathology Cohort: Respect or Resect?Document12 pagesMidterm Outcomes of Minimally Invasive Mitral Valve Surgery in A Heterogeneous Valve Pathology Cohort: Respect or Resect?mony saNo ratings yet
- JCM 10 03239Document42 pagesJCM 10 03239Pamela MusabelliuNo ratings yet
- Okello2017 Article RheumaticHeartDiseaseInUgandaPDocument10 pagesOkello2017 Article RheumaticHeartDiseaseInUgandaPyosefinNo ratings yet
- Balami 2017Document14 pagesBalami 2017palmaputri pinantiNo ratings yet
- A Case Presentation On Acute Coronary Syndrome and Myocardial InfarctionDocument53 pagesA Case Presentation On Acute Coronary Syndrome and Myocardial InfarctionAsniah Hadjiadatu AbdullahNo ratings yet
- A Case Presentation On Acute Coronary Syndrome and Myocardial InfarctionDocument55 pagesA Case Presentation On Acute Coronary Syndrome and Myocardial InfarctionAsniah Hadjiadatu AbdullahNo ratings yet
- Management of Epistaxis in Patients With Ventricular Assist Device: A Retrospective ReviewDocument6 pagesManagement of Epistaxis in Patients With Ventricular Assist Device: A Retrospective ReviewDenta HaritsaNo ratings yet
- Unit 2 GEC 106Document132 pagesUnit 2 GEC 106fernando.gl559No ratings yet
- Montageanleitung sf25 35 enDocument20 pagesMontageanleitung sf25 35 enPaulo santosNo ratings yet
- Electrode ChemDocument17 pagesElectrode Chemapi-372366467% (3)
- En Eco-Drive Panel ConnectionDocument4 pagesEn Eco-Drive Panel ConnectionElectroventica ElectroventicaNo ratings yet
- Stock TakeDocument14 pagesStock Takesafare2222No ratings yet
- VE With CLE 10-Module 22-4th Quarter - CASTRODocument5 pagesVE With CLE 10-Module 22-4th Quarter - CASTRORojan ClarkNo ratings yet
- 2016 Practical Theory Questions SolutionDocument36 pages2016 Practical Theory Questions Solutionsheeess gaadaNo ratings yet
- Victory Over Sin Through Total ConsecrationDocument3 pagesVictory Over Sin Through Total ConsecrationJhon Ray OtañesNo ratings yet
- 2009 - Mazars Insight Ifrs 5 enDocument36 pages2009 - Mazars Insight Ifrs 5 enSahar FekihNo ratings yet
- The Philosophy of Composition (1846)Document20 pagesThe Philosophy of Composition (1846)Denise CoronelNo ratings yet
- Internal Control QuestionnaireDocument19 pagesInternal Control QuestionnaireIchsanNo ratings yet
- Information Pack: Creative Media EducationDocument26 pagesInformation Pack: Creative Media EducationDaniel VladimirovNo ratings yet
- Batch Op LOPA WorksheetDocument35 pagesBatch Op LOPA WorksheetShruti JoshiNo ratings yet
- Salary Survey (Hong Kong) - 2022Document7 pagesSalary Survey (Hong Kong) - 2022Nathan SmithNo ratings yet
- 19 G15 - Polycystic Ovary Syndrome v12.22.2021 1Document3 pages19 G15 - Polycystic Ovary Syndrome v12.22.2021 1decota.sydneyNo ratings yet
- azezew(1)Document48 pagesazezew(1)temesgen AsmamawNo ratings yet
- Earth Works Volume Conversion and Swell FactorsDocument4 pagesEarth Works Volume Conversion and Swell FactorsJj BarakaNo ratings yet
- Country/Airport City Laboratory: AfghanistanDocument25 pagesCountry/Airport City Laboratory: AfghanistanLudovic DumitruNo ratings yet
- Audit of Intangible AssetDocument3 pagesAudit of Intangible Assetd.pagkatoytoyNo ratings yet
- Invoice Being Charged Sued If or Violation Has This in Wrongful - RightfulDocument67 pagesInvoice Being Charged Sued If or Violation Has This in Wrongful - RightfulSteven SchoferNo ratings yet
- PDF 20220814 211454 0000Document6 pagesPDF 20220814 211454 0000Madhav MehtaNo ratings yet
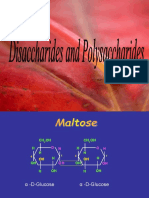
- Disaccharides and PolysaccharidesDocument17 pagesDisaccharides and PolysaccharidesAarthi shreeNo ratings yet
- Management The Essentials Australia 4th Edition Robbins Test BankDocument29 pagesManagement The Essentials Australia 4th Edition Robbins Test Bankfidelmanhangmhr100% (38)
- 1.0sg Equations and Inequalities - Study GuideDocument1 page1.0sg Equations and Inequalities - Study Guiderad58No ratings yet
- CDC121 Weekly Schedule Spring 2017 RidDocument5 pagesCDC121 Weekly Schedule Spring 2017 RidAnonymous x1Lu4qE623No ratings yet
- Pilani MTech SS PDFDocument12 pagesPilani MTech SS PDFonline accountNo ratings yet
- 5 Set Model Question Mathematics (116) MGMT XI UGHSSDocument13 pages5 Set Model Question Mathematics (116) MGMT XI UGHSSSachin ChakradharNo ratings yet
- Soften, Soothe, AllowDocument1 pageSoften, Soothe, AllowTatiannaMartinsNo ratings yet
- The Pevearsion of Russian LiteratureDocument8 pagesThe Pevearsion of Russian LiteratureStan MazoNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)