You might also like
- Atlas of Inflammatory Bowel DiseasesFrom EverandAtlas of Inflammatory Bowel DiseasesWon Ho KimNo ratings yet
- Nci 2 215Document7 pagesNci 2 215TanvirNo ratings yet
- 2015 Article 841Document6 pages2015 Article 841Anh ThưNo ratings yet
- Ymj 59 317Document8 pagesYmj 59 317ItaloLozanoPalominoNo ratings yet
- 18 Los Ejercicios de Schroth Mejoran La Calidad de Vida Relacionada Con La SaludDocument8 pages18 Los Ejercicios de Schroth Mejoran La Calidad de Vida Relacionada Con La SaludMike Bukowski MoreidaNo ratings yet
- Luomajoki Testbatterij LWKDocument13 pagesLuomajoki Testbatterij LWKMylouNo ratings yet
- Diagnostics 12 02631 v2Document16 pagesDiagnostics 12 02631 v2DinaNo ratings yet
- Melese 2020 - Effectiveness of Kinesiotaping OA Knee SRMA jpr-13-1267Document10 pagesMelese 2020 - Effectiveness of Kinesiotaping OA Knee SRMA jpr-13-1267Ikhsan JohnsonNo ratings yet
- Prevalence of and Factors Associated With Sarcopenia Among Elderly Individuals With HypertensionDocument10 pagesPrevalence of and Factors Associated With Sarcopenia Among Elderly Individuals With HypertensionZaskia PutriNo ratings yet
- 1 s2.0 S0753332220309148 MainDocument7 pages1 s2.0 S0753332220309148 Mainyayu latifahNo ratings yet
- Cambios en La Funcion Pulmonar y La Capacidad Funcional en Adolescentes Con Escoliosis Idiopatica LeveDocument11 pagesCambios en La Funcion Pulmonar y La Capacidad Funcional en Adolescentes Con Escoliosis Idiopatica Levefabri190987No ratings yet
- Severidad Oa RodillaDocument10 pagesSeveridad Oa RodillaFrancisco Vicent PachecoNo ratings yet
- Kss Taos Good PrintDocument10 pagesKss Taos Good PrintAfifah Nur FauzaniNo ratings yet
- Knee Osteoarthritis Patient 5Document8 pagesKnee Osteoarthritis Patient 5TanvirNo ratings yet
- Is The Prognosis of Osgood-Schlatter Poorer Than Anticipated?Document9 pagesIs The Prognosis of Osgood-Schlatter Poorer Than Anticipated?gastón giosciaNo ratings yet
- Correlation Between Metabolic Syndrome and Knee Osteoarthritis: Data From The Korean National Health and Nutrition Examination Survey (Knhanes)Document8 pagesCorrelation Between Metabolic Syndrome and Knee Osteoarthritis: Data From The Korean National Health and Nutrition Examination Survey (Knhanes)Agatha GeraldyneNo ratings yet
- Injury August 2023Document369 pagesInjury August 2023isx hdzNo ratings yet
- Grip StrengthDocument11 pagesGrip StrengthMiguel Angel HermosilloNo ratings yet
- The Effect of Body Mass Index On Components Size in Patients With Total Knee ReplacementDocument5 pagesThe Effect of Body Mass Index On Components Size in Patients With Total Knee ReplacementalirezanouriNo ratings yet
- Adhesive Capsulitis of The Shoulder: Protocol For The Adhesive Capsulitis Biomarker (Adcab) StudyDocument6 pagesAdhesive Capsulitis of The Shoulder: Protocol For The Adhesive Capsulitis Biomarker (Adcab) StudyRuben FigueroaNo ratings yet
- Ankylosing Spondylitis Areview DITDEC2019Document6 pagesAnkylosing Spondylitis Areview DITDEC2019Nazmul IslamNo ratings yet
- The Effectiveness of Ultrasound Treatment For The Management of KDocument7 pagesThe Effectiveness of Ultrasound Treatment For The Management of Kkrishnamunirajulu1028No ratings yet
- Work-Related Musculoskeletal Disorders Among DentiDocument7 pagesWork-Related Musculoskeletal Disorders Among DentiLjupce GorgievskiNo ratings yet
- Fractura de CaderaDocument9 pagesFractura de CaderaWendy Lorely Téllez HernándezNo ratings yet
- Jurnal Remato 2Document8 pagesJurnal Remato 2aandakuNo ratings yet
- Pereira 2015Document9 pagesPereira 2015Amalia RosaNo ratings yet
- Maturitas: SciencedirectDocument6 pagesMaturitas: Sciencedirectaeroforce20No ratings yet
- Kinesiophobia in Relation To Physical Activity in Chronic Neck PainDocument8 pagesKinesiophobia in Relation To Physical Activity in Chronic Neck PainCelia CaballeroNo ratings yet
- Effectiveness of The Quadriceps Strengthening Exercise On Pain and Functional Ability of The Women With Osteoarthritis (OA)Document6 pagesEffectiveness of The Quadriceps Strengthening Exercise On Pain and Functional Ability of The Women With Osteoarthritis (OA)Siti lestarinurhamidahNo ratings yet
- Tennis Elbow JOSPT ArticleDocument11 pagesTennis Elbow JOSPT ArticleHasan RahmanNo ratings yet
- Contemporary Clinical Trials CommunicationsDocument8 pagesContemporary Clinical Trials CommunicationsLuis HerreraNo ratings yet
- Quality of Life Physical Functioning and Psychosocial Function Among Patients With Achondroplasia A Targeted Literature ReviewDocument14 pagesQuality of Life Physical Functioning and Psychosocial Function Among Patients With Achondroplasia A Targeted Literature ReviewjakelinelagoadvNo ratings yet
- Exercise For Improving Age-Related Hyperkyphotic Posture: A Systematic ReviewDocument12 pagesExercise For Improving Age-Related Hyperkyphotic Posture: A Systematic ReviewfadiaprimadestyNo ratings yet
- Milwauke BraceDocument21 pagesMilwauke BraceDhiny RatuNo ratings yet
- 2020 Article 3188Document9 pages2020 Article 3188Abril SantiagoNo ratings yet
- A Prospective Study of Efficacy and Outcome Analysis of Role of PRP Injection in Osteoarthritis of Knee Joint 40 Cases Prospective AnalysisDocument6 pagesA Prospective Study of Efficacy and Outcome Analysis of Role of PRP Injection in Osteoarthritis of Knee Joint 40 Cases Prospective AnalysisIJAR JOURNALNo ratings yet
- The Association of Spinal Osteoarthritis With Lumbar LordosisDocument7 pagesThe Association of Spinal Osteoarthritis With Lumbar LordosisPatricio Fernando Garay GallardoNo ratings yet
- High Intensity Interval Training: A Potential Method For Treating SarcopeniaDocument16 pagesHigh Intensity Interval Training: A Potential Method For Treating SarcopeniaFernando CeballosNo ratings yet
- Demographic Profile, Clinical and Analysis of Osteoarthritis Patients in SurabayaDocument6 pagesDemographic Profile, Clinical and Analysis of Osteoarthritis Patients in SurabayaummuNo ratings yet
- Coppieters IDocument15 pagesCoppieters Ihelenlamlam200011No ratings yet
- Journal of Taibah University Medical SciencesDocument7 pagesJournal of Taibah University Medical SciencesIlham Amal MNo ratings yet
- Family Medicine & Medical Science ResearchDocument9 pagesFamily Medicine & Medical Science ResearchAndhika DNo ratings yet
- Annals of Medicine and Surgery: Bareza Rezaei, Elahe Mousavi, Bahram Heshmati, Shaphagh AsadiDocument8 pagesAnnals of Medicine and Surgery: Bareza Rezaei, Elahe Mousavi, Bahram Heshmati, Shaphagh AsadiGeysel SuarezNo ratings yet
- Jurnal Srs SkoliosisDocument5 pagesJurnal Srs SkoliosisDhiny RatuNo ratings yet
- Factors Affecting Self Reported Physical Disability Among Middle Aged Patients With Knee OsteoarthritisDocument8 pagesFactors Affecting Self Reported Physical Disability Among Middle Aged Patients With Knee OsteoarthritisEditor IJTSRDNo ratings yet
- Health Outcomes of Sarcopenia A Systematic ReviewDocument16 pagesHealth Outcomes of Sarcopenia A Systematic Reviewmanuel VenegasNo ratings yet
- Effects of Physical Activity Interventions On AgingDocument12 pagesEffects of Physical Activity Interventions On AgingHargo PsyNo ratings yet
- s00586 010 1543 2Document11 pagess00586 010 1543 2mohamed hazemNo ratings yet
- 2678-Article Text-8150-2-10-20190518Document8 pages2678-Article Text-8150-2-10-20190518Muh SukriNo ratings yet
- Kaptein-Common-Sense Model-OsteoarthritisDocument9 pagesKaptein-Common-Sense Model-OsteoarthritisZyania MelchyNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument9 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Vårbakken2019 Article RelativeDifferenceInMuscleStreDocument13 pagesVårbakken2019 Article RelativeDifferenceInMuscleStreMufidah AlhadarNo ratings yet
- Abstracts / Osteoarthritis and Cartilage 22 (2014) S57 - S489 S413Document2 pagesAbstracts / Osteoarthritis and Cartilage 22 (2014) S57 - S489 S413Yasmin AbassNo ratings yet
- EscoliosisDocument9 pagesEscoliosisJorge Lucas JimenezNo ratings yet
- Clinician Guide - SarcopeniaDocument7 pagesClinician Guide - SarcopeniaPeter petroffNo ratings yet
- Ao 2Document10 pagesAo 2Ayu SuprabawatiNo ratings yet
- Movement Detection Impaired in Patients With Knee Osteoarthritis Compared To Healthy Controls: A Cross-Sectional Case-Control StudyDocument10 pagesMovement Detection Impaired in Patients With Knee Osteoarthritis Compared To Healthy Controls: A Cross-Sectional Case-Control StudyDavid SugiartoNo ratings yet
- Ijerph 19 10510Document15 pagesIjerph 19 10510Victor CristianNo ratings yet
- Children 10 00954 v3Document14 pagesChildren 10 00954 v3ravneetNo ratings yet
- Ahn 2012Document6 pagesAhn 2012Anonymous gMLTpER9IUNo ratings yet
- Abstracts / Osteoarthritis and Cartilage 22 (2014) S57 - S489 S413Document2 pagesAbstracts / Osteoarthritis and Cartilage 22 (2014) S57 - S489 S413Yasmin AbassNo ratings yet
- Osteoartritis TerapeuticaDocument10 pagesOsteoartritis TerapeuticaYasmin AbassNo ratings yet
- Cells 08 00824Document15 pagesCells 08 00824Yasmin AbassNo ratings yet
- Acr 24125Document10 pagesAcr 24125Yasmin AbassNo ratings yet
- ArticleDocument5 pagesArticleYasmin AbassNo ratings yet
- TUV SUD CE Certificate (1500V New Standard)Document3 pagesTUV SUD CE Certificate (1500V New Standard)iszlaitundeNo ratings yet
- Ocean Climate Change EssayDocument2 pagesOcean Climate Change EssayRahmad RivaldiNo ratings yet
- Osmanabadi Goat Breed Status PaperDocument7 pagesOsmanabadi Goat Breed Status PaperShaikh Tausif AhmedNo ratings yet
- ARC 393: Building For DisasterDocument13 pagesARC 393: Building For DisasterAbdullah Al Mamun PrantoNo ratings yet
- 16b. Present Continuous TenseDocument9 pages16b. Present Continuous TenseGung PanjiNo ratings yet
- Chrystal Chao Ci Xin'赵: Achievements Software SkillsDocument4 pagesChrystal Chao Ci Xin'赵: Achievements Software SkillsCHAO CI XINNo ratings yet
- Marangal ES 2022 2023 3rd Quarter NSED Compliance DataDocument2 pagesMarangal ES 2022 2023 3rd Quarter NSED Compliance DatafernandoNo ratings yet
- Sairam Vidyalaya: To Study The Collision of Two Balls in Two DmensionsDocument14 pagesSairam Vidyalaya: To Study The Collision of Two Balls in Two DmensionsAditya VenkatNo ratings yet
- CSEC Biology January 2007 P1 PDFDocument10 pagesCSEC Biology January 2007 P1 PDFNalisha Persaud100% (1)
- Consumer Buying Behavior Toeards Milk ProductDocument54 pagesConsumer Buying Behavior Toeards Milk ProductsuyoganuNo ratings yet
- Subledger Accounting Cost Management DetailsDocument15 pagesSubledger Accounting Cost Management Detailszeeshan780% (1)
- Codecon Tito Jankowski Apr18Document14 pagesCodecon Tito Jankowski Apr18titojankowskiNo ratings yet
- SS-450-72M 144cells: High Efficiency Half-Cell Mono PERC ModuleDocument2 pagesSS-450-72M 144cells: High Efficiency Half-Cell Mono PERC ModuleMatheus FariasNo ratings yet
- 1922 Needle Craft Magazine 1922Document28 pages1922 Needle Craft Magazine 1922Jane Wilde100% (6)
- World Championship 2010Document4 pagesWorld Championship 2010Estella ManeaNo ratings yet
- Pamphlet On Quality Assurance Planning PSC SleepersDocument6 pagesPamphlet On Quality Assurance Planning PSC SleepersDineshKMPNo ratings yet
- Reference Letter For ScholarshipDocument8 pagesReference Letter For Scholarshipjcipchajd100% (2)
- Survey of Processes For High Temperature-High Pressure Gas Purification - OCR PDFDocument241 pagesSurvey of Processes For High Temperature-High Pressure Gas Purification - OCR PDFChristopher BrownNo ratings yet
- AKU Credential VerificationDocument2 pagesAKU Credential VerificationDavid RahulNo ratings yet
- PESTEL Analysis of ChinaDocument4 pagesPESTEL Analysis of ChinaJohnny VásquezNo ratings yet
- Ant and LifeDocument18 pagesAnt and Liferes PDPNo ratings yet
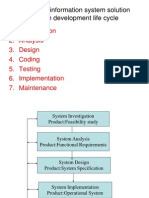
- Developing Information System SolutionDocument42 pagesDeveloping Information System SolutionAbhijeet Mahapatra71% (7)
- Non-Crystalline Solids: Glasses and Amorphous Solids: Prabhat K. GuptaDocument7 pagesNon-Crystalline Solids: Glasses and Amorphous Solids: Prabhat K. GuptaRafaela Rigoni TeixeiraNo ratings yet
- Microsoft PPT - Module4 - OrganisationChart&GraphDocument8 pagesMicrosoft PPT - Module4 - OrganisationChart&GraphOnez WanNo ratings yet
- Character Personality ClothesDocument3 pagesCharacter Personality ClothesMelania AnghelusNo ratings yet
- Plan For A DayDocument5 pagesPlan For A Dayjevinthomas420No ratings yet
- Design CakesDocument1 pageDesign CakesM-LamersNo ratings yet
- Tutorial 06 Questions With Possible Solutions: IS333: Project Management - Semester I 2021Document5 pagesTutorial 06 Questions With Possible Solutions: IS333: Project Management - Semester I 2021Chand DivneshNo ratings yet
- ElectricianSemIICITSQB PDFDocument82 pagesElectricianSemIICITSQB PDFmarvin2008No ratings yet
- Dual-Phase PWM Controller With PWM-VID Reference: General Description FeaturesDocument21 pagesDual-Phase PWM Controller With PWM-VID Reference: General Description FeaturesДмитрий НичипоровичNo ratings yet
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouFrom EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo ratings yet
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (158)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (250)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Feeling Great: The Revolutionary New Treatment for Depression and AnxietyFrom EverandFeeling Great: The Revolutionary New Treatment for Depression and AnxietyNo ratings yet
- Breaking the Chains of Transgenerational Trauma: My Journey from Surviving to ThrivingFrom EverandBreaking the Chains of Transgenerational Trauma: My Journey from Surviving to ThrivingRating: 4.5 out of 5 stars4.5/5 (30)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (141)
- The Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItFrom EverandThe Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (107)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (561)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Emotional Detox for Anxiety: 7 Steps to Release Anxiety and Energize JoyFrom EverandEmotional Detox for Anxiety: 7 Steps to Release Anxiety and Energize JoyRating: 5 out of 5 stars5/5 (6)
- Redefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackFrom EverandRedefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackRating: 4.5 out of 5 stars4.5/5 (153)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationFrom EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationRating: 5 out of 5 stars5/5 (9)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- How To Get Your Sh!t Together: Overcome Anxiety, Defeat Depression, Move on from Trauma, Get Organised, Find Meaning, Follow Your DreamsFrom EverandHow To Get Your Sh!t Together: Overcome Anxiety, Defeat Depression, Move on from Trauma, Get Organised, Find Meaning, Follow Your DreamsRating: 4 out of 5 stars4/5 (8)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1247)
- Happiness Hypothesis, The, by Jonathan Haidt - Book SummaryFrom EverandHappiness Hypothesis, The, by Jonathan Haidt - Book SummaryRating: 4.5 out of 5 stars4.5/5 (95)
- Decluttering at the Speed of Life: Winning Your Never-Ending Battle with StuffFrom EverandDecluttering at the Speed of Life: Winning Your Never-Ending Battle with StuffRating: 4.5 out of 5 stars4.5/5 (578)
- Beyond Thoughts: An Exploration Of Who We Are Beyond Our MindsFrom EverandBeyond Thoughts: An Exploration Of Who We Are Beyond Our MindsRating: 4.5 out of 5 stars4.5/5 (7)