You might also like
- Cap 5Document14 pagesCap 5NatsumiTakamoriNo ratings yet
- Stem Cell Implants Emerging Innovation For Stroke RecoveryDocument14 pagesStem Cell Implants Emerging Innovation For Stroke RecoveryAthenaeum Scientific PublishersNo ratings yet
- neuroasia-2023-28(4)-857Document10 pagesneuroasia-2023-28(4)-857B VeerendrasaiNo ratings yet
- Mesenchymal Stem Cells in Cardiac Regeneration: A Detailed Progress Report of The Last 6 Years (2010 - 2015)Document25 pagesMesenchymal Stem Cells in Cardiac Regeneration: A Detailed Progress Report of The Last 6 Years (2010 - 2015)flying highNo ratings yet
- BstractDocument9 pagesBstractmerosaber622001No ratings yet
- SCCAA 7820 Mesenchymal Stem Cells in The Treatment of Ischemic Stroke 111110Document7 pagesSCCAA 7820 Mesenchymal Stem Cells in The Treatment of Ischemic Stroke 111110Nur FitriahNo ratings yet
- Song 2020Document12 pagesSong 2020RK VermaNo ratings yet
- Secretome 4 PDFDocument17 pagesSecretome 4 PDFAditya Rama DevaraNo ratings yet
- Jurnal Stem CellDocument11 pagesJurnal Stem CellprimaswariNo ratings yet
- Mariott I 2014Document10 pagesMariott I 2014Vinnie Juliana YonatanNo ratings yet
- Afina Thara P - UNAIRDocument6 pagesAfina Thara P - UNAIRThara Pitaloka VreundschapNo ratings yet
- Comparing the Therapeutic Potential of Stem CellsDocument30 pagesComparing the Therapeutic Potential of Stem CellsAnaaya SinghaniaNo ratings yet
- Tissue EngineeringDocument8 pagesTissue EngineeringJimsNo ratings yet
- Cells 10 01043 v2Document17 pagesCells 10 01043 v2marina ruzyatiNo ratings yet
- Review Article: Neuroprotective Effects of Stem Cells in Ischemic StrokeDocument7 pagesReview Article: Neuroprotective Effects of Stem Cells in Ischemic StrokesalmaNo ratings yet
- Usos TerapeuticosDocument33 pagesUsos TerapeuticosJob MonobeNo ratings yet
- Clinic Trăilă of StemDocument22 pagesClinic Trăilă of StemRadu AvramNo ratings yet
- 2019 Article 73Document10 pages2019 Article 73Radu AvramNo ratings yet
- FlippingBook MeSCPro - ProSTEMDocument6 pagesFlippingBook MeSCPro - ProSTEMAdi Putra AriantoNo ratings yet
- Ijms 24 08386Document17 pagesIjms 24 08386Janniel SajolNo ratings yet
- The Future Role of Mesenchymal Stem Cells inDocument5 pagesThe Future Role of Mesenchymal Stem Cells inAthenaeum Scientific PublishersNo ratings yet
- 3 - Mesenchymal Stromal Cells As A Potential Therapeutic For Neurological DisordersDocument6 pages3 - Mesenchymal Stromal Cells As A Potential Therapeutic For Neurological DisordersÊndel AlvesNo ratings yet
- Checinski 2022 Autologous Stem Cells Transplants IDocument23 pagesChecinski 2022 Autologous Stem Cells Transplants Ibarrera2001No ratings yet
- 1 s2.0 S018844092030638X MainDocument9 pages1 s2.0 S018844092030638X MainDarshan GandhiNo ratings yet
- ijmm_21_3_271_PDFDocument9 pagesijmm_21_3_271_PDFbixiv81367No ratings yet
- Cell Tracking in Cardiac RepairDocument16 pagesCell Tracking in Cardiac RepairdeadcorpsesNo ratings yet
- Immunobiology of Human Mesenchymal Stem Cells and Future Use in Hematopoietic Stem Cell TransplantationDocument14 pagesImmunobiology of Human Mesenchymal Stem Cells and Future Use in Hematopoietic Stem Cell TransplantationTharissa SyabaniaNo ratings yet
- Effect of The Microenvironment On Mesenchymal Stem Cell Paracrine Signaling: Opportunities To Engineer The Therapeutic EffectDocument15 pagesEffect of The Microenvironment On Mesenchymal Stem Cell Paracrine Signaling: Opportunities To Engineer The Therapeutic Effectrunky febrankaNo ratings yet
- 59d4 PDFDocument15 pages59d4 PDFrunky febrankaNo ratings yet
- Neuro-Oncology: Stem Cell-Based Therapies For Tumors in The Brain: Are We There Yet?Document13 pagesNeuro-Oncology: Stem Cell-Based Therapies For Tumors in The Brain: Are We There Yet?Vinnie Juliana YonatanNo ratings yet
- Cancer Stem Cell Niche The Place To BeDocument7 pagesCancer Stem Cell Niche The Place To BeAlejandra Isabel Juarez JimenezNo ratings yet
- 2021 Front. Cell Dev. Biol. Laundos TL Et Al.Document15 pages2021 Front. Cell Dev. Biol. Laundos TL Et Al.PerpetuaNo ratings yet
- Review Article: Stem Cells: Innovations in Clinical ApplicationsDocument10 pagesReview Article: Stem Cells: Innovations in Clinical Applications03151206639No ratings yet
- The Potencial of Mesenchymal Stem CellsDocument14 pagesThe Potencial of Mesenchymal Stem CellsBruno SouzaNo ratings yet
- NeurologyDocument19 pagesNeurologymerosaber622001No ratings yet
- Knee Stem CellsDocument25 pagesKnee Stem CellsKN TMNo ratings yet
- Pharmaceuticals 13 00031Document18 pagesPharmaceuticals 13 00031DwitaRiadiniNo ratings yet
- Prospect of Stem Cells Conditioned Medium (Secretome) in Ligament and Tendon Healing: A Systematic ReviewDocument8 pagesProspect of Stem Cells Conditioned Medium (Secretome) in Ligament and Tendon Healing: A Systematic ReviewMuhammad RifqoNo ratings yet
- Advanced Models of Human Skeletal Muscle Differentiation - 2021 - Current OpiniDocument13 pagesAdvanced Models of Human Skeletal Muscle Differentiation - 2021 - Current OpinimetrorespoNo ratings yet
- Data CollectionDocument9 pagesData Collectionapi-512131053No ratings yet
- Stem Cell Therapy: A Novel & Futuristic Treatment Modality For Disaster InjuriesDocument17 pagesStem Cell Therapy: A Novel & Futuristic Treatment Modality For Disaster InjuriesChiboyKrenzNo ratings yet
- Bone Marrow Mesenchymal Stem Cell-Derived ExosomesDocument9 pagesBone Marrow Mesenchymal Stem Cell-Derived Exosomesiam_ca2No ratings yet
- Menstrual Blood Derived Stem Cells and Their Scope in Regenerative Medicine A Review ArticleDocument6 pagesMenstrual Blood Derived Stem Cells and Their Scope in Regenerative Medicine A Review ArticleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Stem Cells and Cancer Stem Cells, Volume 2 - Stem Cells and Cancer Stem Cells, Therapeutic Applications in Disease and Injury - Volume 2Document409 pagesStem Cells and Cancer Stem Cells, Volume 2 - Stem Cells and Cancer Stem Cells, Therapeutic Applications in Disease and Injury - Volume 2ArtanNo ratings yet
- JR 043 - Mesenchymal Stem Cell and Clinical Application in Chronic Lung Disease.210921-RevisionDocument10 pagesJR 043 - Mesenchymal Stem Cell and Clinical Application in Chronic Lung Disease.210921-RevisionLaila MaulidNo ratings yet
- Secretome of Mesenchymal Stromal Cells As A Possible Innovative Therapeutic Tools in Facial Nerve Injury TreatmentDocument7 pagesSecretome of Mesenchymal Stromal Cells As A Possible Innovative Therapeutic Tools in Facial Nerve Injury TreatmentIgor HermandoNo ratings yet
- Tissue Engineering and Regeneration in Dentistry: Current StrategiesFrom EverandTissue Engineering and Regeneration in Dentistry: Current StrategiesRachel J. WaddingtonNo ratings yet
- Assingement#2 Stem CellDocument6 pagesAssingement#2 Stem Cellhaseeb ShafaatNo ratings yet
- Potential HNSC and IL-6Document18 pagesPotential HNSC and IL-6Farhan Royan PermanahadiNo ratings yet
- Stemcells 2007-0416Document12 pagesStemcells 2007-0416Ikke OppgaveNo ratings yet
- tmpDBD5 TMPDocument6 pagestmpDBD5 TMPFrontiersNo ratings yet
- Mesenchymal Stem Cell Derived-Exosomes: A Modern Approach in Translational MedicineDocument21 pagesMesenchymal Stem Cell Derived-Exosomes: A Modern Approach in Translational MedicineMuhammad Javed GabaNo ratings yet
- Strategies To Capitalize On Cell Spheroid Therapeutic Potential For Tissue Repair and Disease ModelingDocument13 pagesStrategies To Capitalize On Cell Spheroid Therapeutic Potential For Tissue Repair and Disease ModelingShai FuchsNo ratings yet
- Contemporary Biological Therapies For Cardiovascular Diseases MMH Nuri Ahmad YahyaDocument6 pagesContemporary Biological Therapies For Cardiovascular Diseases MMH Nuri Ahmad YahyaHammad. A Rehan ACCANo ratings yet
- Cell Therapy For Stroke: Emphasis On Optimizing Safety and Efficacy Profile of Endothelial Progenitor CellsDocument8 pagesCell Therapy For Stroke: Emphasis On Optimizing Safety and Efficacy Profile of Endothelial Progenitor CellsrenaraNo ratings yet
- Skeletal MuscleDocument11 pagesSkeletal MuscleStefania CristinaNo ratings yet
- 10 1016@j Biomaterials 2016 09 007Document11 pages10 1016@j Biomaterials 2016 09 007Jorge Aguirre GonzalezNo ratings yet
- Optimized Feature Extraction in Mesenchymal Stem Cells With Classification AlgorithmsDocument7 pagesOptimized Feature Extraction in Mesenchymal Stem Cells With Classification AlgorithmsGanesh adminNo ratings yet
- journal.pone.0277442Document15 pagesjournal.pone.0277442alphafoldjesus710No ratings yet
- Topik 6 MentahDocument16 pagesTopik 6 Mentahaburachman24No ratings yet
- A Simple Method To Isolate and Expand Human Umbilical CordDocument9 pagesA Simple Method To Isolate and Expand Human Umbilical Cordaburachman24No ratings yet
- Complexies of X Chromosome Inactivation Status in Female Human IPS-A Brief ReviewDocument7 pagesComplexies of X Chromosome Inactivation Status in Female Human IPS-A Brief Reviewaburachman24No ratings yet
- ID Analisis Standar Pelayanan Minimal Pada Instalasi Rawat Jalan Di Rsud Kota SemarDocument9 pagesID Analisis Standar Pelayanan Minimal Pada Instalasi Rawat Jalan Di Rsud Kota SemarrohishatulilmiyahNo ratings yet
- The Parts of The Cell and Their FunctionsDocument2 pagesThe Parts of The Cell and Their Functionsraphael100% (1)
- Inoculum Development and Growth for Microbial ProductionDocument1 pageInoculum Development and Growth for Microbial Productionrocky00023100% (5)
- 〈90〉 Fetal Bovine Serum-Quality Attributes and Functionality TestsDocument4 pages〈90〉 Fetal Bovine Serum-Quality Attributes and Functionality Testsmehrdarou.qaNo ratings yet
- Activity Sheet 1 Bacteria Take OverDocument6 pagesActivity Sheet 1 Bacteria Take OverAmor Reyes EngNo ratings yet
- In Mu No ModulationDocument10 pagesIn Mu No Modulationmaxi392No ratings yet
- Nematode BehaviourDocument445 pagesNematode Behaviourdouglasman100% (4)
- 5e Heredity Genetics Unit Portfolio CrespoDocument6 pages5e Heredity Genetics Unit Portfolio Crespoapi-247308630No ratings yet
- Lecture On The Physiology of Neuromuscular Junction (NMJ) by Dr. RoomiDocument18 pagesLecture On The Physiology of Neuromuscular Junction (NMJ) by Dr. RoomiMudassar Roomi100% (3)
- Comprehensive 12-Week USMLE Step 1 Study PlanDocument22 pagesComprehensive 12-Week USMLE Step 1 Study PlanMarshal BruceNo ratings yet
- Week 6Document5 pagesWeek 6janice alquizarNo ratings yet
- Biopsychology Pinel Chapter 9Document2 pagesBiopsychology Pinel Chapter 9Krisha AvorqueNo ratings yet
- Carbohydrate Metabolism Catabolism 2013Document108 pagesCarbohydrate Metabolism Catabolism 2013Anonymous nErkwtXnuS100% (1)
- BOTANY:: 2008: List - I List - IIDocument7 pagesBOTANY:: 2008: List - I List - IIjp techNo ratings yet
- Invertebrate Paleontology and Evolution. Fourth Edition (Clarkson, 1998)Document463 pagesInvertebrate Paleontology and Evolution. Fourth Edition (Clarkson, 1998)Carito Barrozo100% (1)
- Veterinary Immunology Tanuvas Notes VMC - 221 PDFDocument124 pagesVeterinary Immunology Tanuvas Notes VMC - 221 PDFSantosh BhandariNo ratings yet
- Genetic Engineering's Latest ApplicationsDocument23 pagesGenetic Engineering's Latest ApplicationsKarthika Umashankar57% (7)
- I. /58 II. /28 Total: Strictly No Erasures and Alterations Only in Multiple-Choice PartDocument2 pagesI. /58 II. /28 Total: Strictly No Erasures and Alterations Only in Multiple-Choice PartBren DonatosNo ratings yet
- Botany SubdivisionsDocument70 pagesBotany Subdivisionsjackassjoey100% (1)
- 7 Study or Research ProposalDocument3 pages7 Study or Research ProposalMir Sajjad HüSsàïñNo ratings yet
- Reproductive System Grade 7Document5 pagesReproductive System Grade 7Valentina NapitupuluNo ratings yet
- Block Schedule, 1st Semester 2018-2019Document67 pagesBlock Schedule, 1st Semester 2018-2019Kim Kenneth RocaNo ratings yet
- Dr. B. VictorDocument29 pagesDr. B. VictorBnr GoudNo ratings yet
- Mosquitoes' attraction to human sweat mechanismDocument3 pagesMosquitoes' attraction to human sweat mechanismiftitah salsabilaNo ratings yet
- Culturomics of The Plant Prokaryotic Microbiome and The - 2019 - Journal of AdvaDocument13 pagesCulturomics of The Plant Prokaryotic Microbiome and The - 2019 - Journal of AdvaSarras InfoNo ratings yet
- Report Text ExamDocument7 pagesReport Text ExamGusti Ayu Cantika Cordelia CandraNo ratings yet
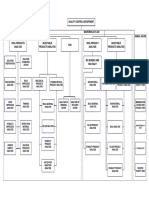
- AVP-QCD-QD-001-Quality Control DepartmentDocument1 pageAVP-QCD-QD-001-Quality Control DepartmentDilawar BakhtNo ratings yet
- Nat. Biotechnol. 2006 PédelacqDocument11 pagesNat. Biotechnol. 2006 PédelacqCarolineNo ratings yet
- Es UbdDocument4 pagesEs Ubdapi-275510930No ratings yet
- State Council of Educational Research and Training TNCF 2017 - Draft SyllabusDocument9 pagesState Council of Educational Research and Training TNCF 2017 - Draft SyllabusVenkat HariNo ratings yet
- 2.ultrastructure of Bacterial Cell 10.2.2016Document98 pages2.ultrastructure of Bacterial Cell 10.2.2016Odey BeekNo ratings yet