You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
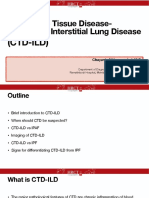
- Connective Tissue Disease-Associated Interstitial Lung DiseaseDocument35 pagesConnective Tissue Disease-Associated Interstitial Lung DiseaseSilp SatjawattanavimolNo ratings yet
- Pulmonary Alveolar Proteinosis (PAP) : Punchalee Kaenmuang M.DDocument42 pagesPulmonary Alveolar Proteinosis (PAP) : Punchalee Kaenmuang M.DSilp SatjawattanavimolNo ratings yet
- Interstitial Pneumonia With Autoimmune Features (IPAF) : Interesting CaseDocument10 pagesInterstitial Pneumonia With Autoimmune Features (IPAF) : Interesting CaseSilp SatjawattanavimolNo ratings yet
- STATA Command SummaryDocument3 pagesSTATA Command SummarySilp SatjawattanavimolNo ratings yet
- Basic STATA CommandDocument5 pagesBasic STATA CommandSilp SatjawattanavimolNo ratings yet
- Nitra Piyavisetpat, MD Medpark Hospital King Chulalongkorn Memorial HospitalDocument42 pagesNitra Piyavisetpat, MD Medpark Hospital King Chulalongkorn Memorial HospitalSilp SatjawattanavimolNo ratings yet
- MCQ Internal Med 2018-Chest PDFDocument44 pagesMCQ Internal Med 2018-Chest PDFSilp SatjawattanavimolNo ratings yet
- ICM Neuroradiology: Siri-On Tritrakarn, M.D. Division of Diagnostic NeuroradiologyDocument41 pagesICM Neuroradiology: Siri-On Tritrakarn, M.D. Division of Diagnostic NeuroradiologySilp SatjawattanavimolNo ratings yet
- Introduction To Gastrointestinal Radiology: Piyaporn Apisarnthanarak, M.D. Faculty of Medicine Siriraj HospitalDocument37 pagesIntroduction To Gastrointestinal Radiology: Piyaporn Apisarnthanarak, M.D. Faculty of Medicine Siriraj HospitalSilp Satjawattanavimol100% (1)
- Cannabis PreparationDocument44 pagesCannabis PreparationSilp SatjawattanavimolNo ratings yet
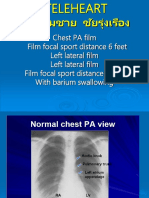
- Chest PA Film Film Focal Sport Distance 6 Feet Left Lateral Film Left Lateral Film Film Focal Sport Distance 6 Feet With Barium SwallowingDocument39 pagesChest PA Film Film Focal Sport Distance 6 Feet Left Lateral Film Left Lateral Film Film Focal Sport Distance 6 Feet With Barium SwallowingSilp SatjawattanavimolNo ratings yet
- The Vanish TrialDocument41 pagesThe Vanish TrialSilp SatjawattanavimolNo ratings yet
- PART - A (40 Marks) : CLASS X (2020-21) English (Code 0184) Sample Paper-08Document9 pagesPART - A (40 Marks) : CLASS X (2020-21) English (Code 0184) Sample Paper-08Poonam GuptaNo ratings yet
- BDRRM LIST OF PPAsDocument4 pagesBDRRM LIST OF PPAsYang Rhea100% (2)
- Soal Anestesi April 2012Document5 pagesSoal Anestesi April 2012farid akbarNo ratings yet
- Iso Chain 7xDocument12 pagesIso Chain 7xAnonymous hndaj8zCA100% (1)
- Articles 2138057 PDFDocument14 pagesArticles 2138057 PDFsandra garcia molinaNo ratings yet
- Kamagradubai - Ae-Kamagra Dubai - Online Herbal Supplement Store in Dubai UAEDocument222 pagesKamagradubai - Ae-Kamagra Dubai - Online Herbal Supplement Store in Dubai UAEkamagradubai0No ratings yet
- (Draft) Contoh - HSE Action PlanDocument8 pages(Draft) Contoh - HSE Action PlanmamanNo ratings yet
- Form C and DDocument3 pagesForm C and DJerome DalisayNo ratings yet
- RegQuest August 2018Document12 pagesRegQuest August 2018Lou EdwardsNo ratings yet
- IPC Project On IntoxicationDocument17 pagesIPC Project On IntoxicationDeepak RavNo ratings yet
- Substance Use Addiction QuestionsDocument2 pagesSubstance Use Addiction Questionsapi-545456609No ratings yet
- Health Care Ethics - Ncm108Document8 pagesHealth Care Ethics - Ncm108AlyNo ratings yet
- Theoretical Foundation in Nursing - ReviewerDocument17 pagesTheoretical Foundation in Nursing - ReviewerTresnan QuiomNo ratings yet
- NCP Impaiered Skin IntegrityDocument1 pageNCP Impaiered Skin Integrityeiram2264% (11)
- Letter To PhilhealthDocument5 pagesLetter To PhilhealthCCC DocsNo ratings yet
- Endografts For The Treatment of Abdominal Aortic ADocument15 pagesEndografts For The Treatment of Abdominal Aortic AAhmed MohammedNo ratings yet
- Dementia Care Course 2Document17 pagesDementia Care Course 2MandalinaNo ratings yet
- Operating Manual - MiniSpin (Plus)Document40 pagesOperating Manual - MiniSpin (Plus)Claudio Verna100% (1)
- Blood Transfusion TeachingDocument18 pagesBlood Transfusion Teachingapi-277522722No ratings yet
- Eastern Medicine Curricular 2004Document111 pagesEastern Medicine Curricular 2004Hakeem Farhan TariqiNo ratings yet
- Writing Module:: ParaphrasingDocument23 pagesWriting Module:: Paraphrasingpot poootNo ratings yet
- Electricity From The Polestar N30 Lowfield MRI System Regarding Resecting Nonenhancing Intraaxial Brain Lesionsmlpuo PDFDocument1 pageElectricity From The Polestar N30 Lowfield MRI System Regarding Resecting Nonenhancing Intraaxial Brain Lesionsmlpuo PDFswitchmint1No ratings yet
- 2 Imrad ResearchDocument15 pages2 Imrad Researchninyawenceslao4No ratings yet
- 7e Lesson PlanDocument6 pages7e Lesson PlanDave Matthew LibiranNo ratings yet
- Form-6 Leave FormDocument6 pagesForm-6 Leave FormjeynsilbonzaNo ratings yet
- Clinical Oncology AssignmentDocument6 pagesClinical Oncology Assignmentapi-280366843No ratings yet
- HSM 476 Article ReviewDocument8 pagesHSM 476 Article ReviewNur AdibahNo ratings yet
- In Vivo Efficacy of Diospyros Abyssinica Leaf 80% Methanolic Extract From Tooro Botanical Gardens On Wounds Using MiceDocument18 pagesIn Vivo Efficacy of Diospyros Abyssinica Leaf 80% Methanolic Extract From Tooro Botanical Gardens On Wounds Using MiceKIU PUBLICATION AND EXTENSIONNo ratings yet
- DR Lal Pathlabs: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini Delhi 110085Document5 pagesDR Lal Pathlabs: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini Delhi 110085ankurindustries20No ratings yet
- Fix Fix Soal Pat Bahasa Dan Sastra Inggris Kelas X Ipa 1, X Ips 1-4Document30 pagesFix Fix Soal Pat Bahasa Dan Sastra Inggris Kelas X Ipa 1, X Ips 1-4Eka MurniatiNo ratings yet