You might also like
- Test Bank For Medical Terminology For Health Professions 8th Edition by EhrlichDocument13 pagesTest Bank For Medical Terminology For Health Professions 8th Edition by EhrlichJames Chapman100% (35)
- Pathophysiology HemothoraxDocument1 pagePathophysiology HemothoraxFlauros Ryu Jabien50% (4)
- Quality of Life and People Living With AIDS: Relationship With Sociodemographic and Health AspectsDocument9 pagesQuality of Life and People Living With AIDS: Relationship With Sociodemographic and Health AspectsCyril Jane Caanyagan AcutNo ratings yet
- Self-Esteem in Patients With Diabetes Mellitus and Foot UlcersDocument7 pagesSelf-Esteem in Patients With Diabetes Mellitus and Foot UlcerslatifaNo ratings yet
- 10 1111@idj 12576Document7 pages10 1111@idj 12576badria bawazirNo ratings yet
- Caranza Diagnosis EnglishDocument3 pagesCaranza Diagnosis EnglishZuwandi Abd KadirNo ratings yet
- Pmedicine D 19 04148 PDFDocument23 pagesPmedicine D 19 04148 PDFFelipe GentaNo ratings yet
- Collado Boira2021Document10 pagesCollado Boira2021Andreia LopesNo ratings yet
- Global, Regional Prevalence, Incidence and Risk Factors of Knee Osteoarthritis PopulationDocument13 pagesGlobal, Regional Prevalence, Incidence and Risk Factors of Knee Osteoarthritis PopulationnurjannahnasirNo ratings yet
- Association Between Orthodontic Treatment and Periodontal DiseasesDocument10 pagesAssociation Between Orthodontic Treatment and Periodontal DiseasesLalo MojicaNo ratings yet
- 1 s2.0 S0278239122001793 Main PDFDocument33 pages1 s2.0 S0278239122001793 Main PDFKEN WONG SIONG HOUNo ratings yet
- Quality of Life Assessment Among Patients Undergoing Total Knee Arthroplasty in ManausDocument8 pagesQuality of Life Assessment Among Patients Undergoing Total Knee Arthroplasty in ManausRehu CooperNo ratings yet
- Obesity and Oral Health - Is There An Association?: Collegium Antropologicum September 2012Document6 pagesObesity and Oral Health - Is There An Association?: Collegium Antropologicum September 2012Nicolas YoungNo ratings yet
- Prpic2012 PDFDocument6 pagesPrpic2012 PDFNicolas YoungNo ratings yet
- Prpic2012 PDFDocument6 pagesPrpic2012 PDFNicolas YoungNo ratings yet
- Obesity and Oral Health - Is There An Association?: Collegium Antropologicum September 2012Document6 pagesObesity and Oral Health - Is There An Association?: Collegium Antropologicum September 2012Nicolas YoungNo ratings yet
- 1 s2.0 S2237936319300553 Main PDFDocument7 pages1 s2.0 S2237936319300553 Main PDFkasilyaNo ratings yet
- Coloproctology: Results of Videolaparoscopic Surgical Treatment of Diverticular Disease of The ColonDocument5 pagesColoproctology: Results of Videolaparoscopic Surgical Treatment of Diverticular Disease of The ColonMaxend Arselino SilooyNo ratings yet
- PEÑARANDADocument8 pagesPEÑARANDAAlejandroNo ratings yet
- s13104 017 2406 2Document8 pagess13104 017 2406 2Clarissa Simon FactumNo ratings yet
- ArtigooDocument9 pagesArtigooWilliam SchutzNo ratings yet
- Can Endoscopic Atrophy Predict Histological Atrophy? Historical Study in United Kingdom and JapanDocument12 pagesCan Endoscopic Atrophy Predict Histological Atrophy? Historical Study in United Kingdom and JapanJosseph EscobarNo ratings yet
- Assessment of KnowledgeDocument17 pagesAssessment of KnowledgeNiningNo ratings yet
- Full Length Research Article: ISSN: 2230-9926Document5 pagesFull Length Research Article: ISSN: 2230-9926yaqthanhaiderz yaqthanhaiderzNo ratings yet
- The American Journal of SurgeryDocument6 pagesThe American Journal of SurgeryBriando Stevano LinelejanNo ratings yet
- The Journal of The Economics of Ageing: Full Length ArticleDocument9 pagesThe Journal of The Economics of Ageing: Full Length Articlemandeep kaurNo ratings yet
- CH in PopulationDocument11 pagesCH in PopulationMaria CorbuNo ratings yet
- Prevalence of Vitiligo and Associated Comorbidities in KoreaDocument7 pagesPrevalence of Vitiligo and Associated Comorbidities in KoreaRatna NingsihNo ratings yet
- J Clinic Periodontology - 2020 - Graetz - Oral Health Related Quality of Life Impacts Are Low 27 Years After PeriodontalDocument10 pagesJ Clinic Periodontology - 2020 - Graetz - Oral Health Related Quality of Life Impacts Are Low 27 Years After PeriodontalISABEL ESCOBAR MINOTASNo ratings yet
- Role of Geriatric Oncologists in Optimizing Care of Urological Oncology PatientsDocument10 pagesRole of Geriatric Oncologists in Optimizing Care of Urological Oncology PatientsrocioNo ratings yet
- Peerj 5258Document17 pagesPeerj 5258mmputraNo ratings yet
- Association Between Periodontal Health andDocument7 pagesAssociation Between Periodontal Health andTran DuongNo ratings yet
- 05-Is Measurement of The Gingival Biotype ReliableDocument6 pages05-Is Measurement of The Gingival Biotype ReliableaemontoNo ratings yet
- Vallejo Rosero2019Document21 pagesVallejo Rosero2019sdadNo ratings yet
- Case-Control Study of Oral Disease Indexes in Individuals With Head and Neck Cancer After Antineoplastic TherapyDocument6 pagesCase-Control Study of Oral Disease Indexes in Individuals With Head and Neck Cancer After Antineoplastic TherapyGeorgia.annaNo ratings yet
- Clinical Features and Antimicrobial Susceptibility of Oral B 2022 Journal ofDocument6 pagesClinical Features and Antimicrobial Susceptibility of Oral B 2022 Journal ofDavid ABCNo ratings yet
- O Idoso Institucionalizado Perfis Sociodemográficos e Clínico-Funcionais Relacionados À TonturaDocument11 pagesO Idoso Institucionalizado Perfis Sociodemográficos e Clínico-Funcionais Relacionados À TonturaAlmir VitoriaNo ratings yet
- "Living With A Stoma": Exploring The Lived Experience of Patients With Permanent ColostomyDocument15 pages"Living With A Stoma": Exploring The Lived Experience of Patients With Permanent ColostomyDaniel AbomaNo ratings yet
- 1 s2.0 S1201971220300862 MainDocument6 pages1 s2.0 S1201971220300862 MainLyrian LohNo ratings yet
- Association Between Resilience and Quality of Life in Patients With Colon CancerDocument7 pagesAssociation Between Resilience and Quality of Life in Patients With Colon CancerICR CONSULTORESNo ratings yet
- Managementofedentulous Patients: Damian J. Lee,, Paola C. SaponaroDocument13 pagesManagementofedentulous Patients: Damian J. Lee,, Paola C. SaponaroDANTE DELEGUERYNo ratings yet
- Quality of Life After Bladder Cancer: A Cross-Sectional Survey of Patient-Reported OutcomesDocument12 pagesQuality of Life After Bladder Cancer: A Cross-Sectional Survey of Patient-Reported OutcomesSteve GannabanNo ratings yet
- Ijerph 17 05824Document12 pagesIjerph 17 05824elvin peraltaNo ratings yet
- Tumors of Foot and Ankle A Single Institution Experience PDFDocument6 pagesTumors of Foot and Ankle A Single Institution Experience PDFICNo ratings yet
- Abstracts COMAPI 2014 IJMSDocument20 pagesAbstracts COMAPI 2014 IJMSfelipetheNo ratings yet
- BMC GeriatricsDocument12 pagesBMC Geriatricsjessica eNo ratings yet
- Managementofedentulous Patients: Damian J. Lee,, Paola C. SaponaroDocument13 pagesManagementofedentulous Patients: Damian J. Lee,, Paola C. Saponarosnehal jaiswalNo ratings yet
- Effectiveness of Instruction Program in Improving Balance Level Among Seniors With OsteoporosisDocument8 pagesEffectiveness of Instruction Program in Improving Balance Level Among Seniors With OsteoporosisCentral Asian StudiesNo ratings yet
- Pereira 2015Document9 pagesPereira 2015Amalia RosaNo ratings yet
- Burden of Oral Mucositis in Stem Cell Transplant Patients-The Patients' PerspectiveDocument8 pagesBurden of Oral Mucositis in Stem Cell Transplant Patients-The Patients' PerspectivePaola GilNo ratings yet
- Anemia and Periodontitis: An Enigma?: Dr. Soumya. K. Nair, Dr. Mohamed Faizuddin, Dr. Jayanthi.D.,M.D.SDocument8 pagesAnemia and Periodontitis: An Enigma?: Dr. Soumya. K. Nair, Dr. Mohamed Faizuddin, Dr. Jayanthi.D.,M.D.SNovie ApriantiNo ratings yet
- Oral Soft Tissue Biopsies in Oporto, Portugal: An Eight Year Retrospective AnalysisDocument9 pagesOral Soft Tissue Biopsies in Oporto, Portugal: An Eight Year Retrospective Analysisjuan pablo meneses rojasNo ratings yet
- Comparison of Effects of Bracket Types and Treatment Duration On Periodontal Health of Adult PatientsDocument5 pagesComparison of Effects of Bracket Types and Treatment Duration On Periodontal Health of Adult Patientsluthfi fernandaNo ratings yet
- Comparison of Two Survey Instruments Measuring Quality of Life in Pediatric Dentofacial PatientsDocument6 pagesComparison of Two Survey Instruments Measuring Quality of Life in Pediatric Dentofacial PatientsFrancelia Quiñonez RuvalcabaNo ratings yet
- Quality of Life and Characteristics of Colostomy PatientsDocument8 pagesQuality of Life and Characteristics of Colostomy PatientsJurnal Ners UNAIRNo ratings yet
- 1 s2.0 S2531137919300951 MainDocument7 pages1 s2.0 S2531137919300951 MainTohariNo ratings yet
- Obezitatea La Copii Si Boala ParodontalaDocument8 pagesObezitatea La Copii Si Boala ParodontalaLavinia PascuNo ratings yet
- Art:10.1186/s12903 015 0052 4Document8 pagesArt:10.1186/s12903 015 0052 4Laura Mejia VergaraNo ratings yet
- QUALITY OF LIFE OF PATIENTS WITH END-STOMA IN MEDAN RevisionDocument12 pagesQUALITY OF LIFE OF PATIENTS WITH END-STOMA IN MEDAN RevisionNorma YantiNo ratings yet
- Management of Edentulous DCNADocument13 pagesManagement of Edentulous DCNAJohnNo ratings yet
- Journal of Periodontology - 2018 - Lang - Periodontal HealthDocument8 pagesJournal of Periodontology - 2018 - Lang - Periodontal HealthMonica MartínezNo ratings yet
- Diagnostic Problems in Tumors of Head and Neck: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Head and Neck: Selected TopicsRating: 5 out of 5 stars5/5 (1)
- EMP2 3 E12630Document25 pagesEMP2 3 E12630Briando Stevano LinelejanNo ratings yet
- Current Practices in Endotracheal Tube Size Selection For AdultsDocument5 pagesCurrent Practices in Endotracheal Tube Size Selection For AdultsBriando Stevano LinelejanNo ratings yet
- Pouches and Stomas: Key PointsDocument6 pagesPouches and Stomas: Key PointsBriando Stevano LinelejanNo ratings yet
- Contemporary Clinical Trials: SciencedirectDocument6 pagesContemporary Clinical Trials: SciencedirectBriando Stevano LinelejanNo ratings yet
- The American Journal of SurgeryDocument6 pagesThe American Journal of SurgeryBriando Stevano LinelejanNo ratings yet
- Accepted Manuscript: Clinical NeurophysiologyDocument52 pagesAccepted Manuscript: Clinical NeurophysiologyBriando Stevano LinelejanNo ratings yet
- Humanimmunodeficiency Virusinitialassessmentand Routinefollow-UpDocument16 pagesHumanimmunodeficiency Virusinitialassessmentand Routinefollow-UpBriando Stevano LinelejanNo ratings yet
- Navigation-Guided Reduction and Orbital Floor Reconstruction in The Treatment of Zygomatic-Orbital-Maxillary Complex FracturesDocument7 pagesNavigation-Guided Reduction and Orbital Floor Reconstruction in The Treatment of Zygomatic-Orbital-Maxillary Complex FracturesBriando Stevano LinelejanNo ratings yet
- American Journal of Clinical HypnosisDocument6 pagesAmerican Journal of Clinical HypnosisBriando Stevano LinelejanNo ratings yet
- Zygomatic Fractures: Classification and Complications: TveterasDocument7 pagesZygomatic Fractures: Classification and Complications: TveterasBriando Stevano LinelejanNo ratings yet
- Evaluation of Treatment of Zygomatic Bone and Zygomatic Arch Fractures: A Retrospective Study of 10 YearsDocument6 pagesEvaluation of Treatment of Zygomatic Bone and Zygomatic Arch Fractures: A Retrospective Study of 10 YearsBriando Stevano LinelejanNo ratings yet
- List of EpidemicsDocument49 pagesList of EpidemicsBriando Stevano LinelejanNo ratings yet
- Abdomen - KLP 10Document33 pagesAbdomen - KLP 10Briando Stevano LinelejanNo ratings yet
- Cholera Philippine Setting.Document1 pageCholera Philippine Setting.Lara TechiesNo ratings yet
- Early Complications in Prepectoral Tissue Expander Based Breast ReconstructionDocument11 pagesEarly Complications in Prepectoral Tissue Expander Based Breast ReconstructionBruno Mañon0% (1)
- Clinical Case StudyDocument39 pagesClinical Case Studyapi-240895351No ratings yet
- C1933-GL Global Pharmaceuticals Medicine Manufacturing Industry ReportDocument69 pagesC1933-GL Global Pharmaceuticals Medicine Manufacturing Industry Reportsamuel.p.collingsNo ratings yet
- Pharmacotheraphy Gastrointestinal Tract: OutlineDocument34 pagesPharmacotheraphy Gastrointestinal Tract: OutlineMaharani Dewi NugrahaNo ratings yet
- Soal Academic Reading SPDocument2 pagesSoal Academic Reading SPRisda Riani Risda100% (1)
- Indranila 2021Document22 pagesIndranila 2021reski utamiNo ratings yet
- Complex Care Concept MapDocument12 pagesComplex Care Concept Mapapi-508434862No ratings yet
- GsisDocument3 pagesGsisPecu MT ProvinceNo ratings yet
- Notes On Nursing: What It Is and What It Is Not Was A Book First Published by FlorenceDocument7 pagesNotes On Nursing: What It Is and What It Is Not Was A Book First Published by FlorenceAlexis Nichole PayaoNo ratings yet
- Cardiology-5 DysrhythmiaDocument16 pagesCardiology-5 DysrhythmiaMahmoud RamadanNo ratings yet
- Bardac 208M - APIC CSPA PosterDocument1 pageBardac 208M - APIC CSPA PosterDyaniNo ratings yet
- Data BarangDocument90 pagesData BarangBella KarinaNo ratings yet
- Fit Well Core Concepts and Labs in Physical Fitness and Wellness 13Th Edition Full ChapterDocument41 pagesFit Well Core Concepts and Labs in Physical Fitness and Wellness 13Th Edition Full Chapterwilliam.decker273100% (26)
- Physical TherapyDocument11 pagesPhysical TherapyEvelyn MedinaNo ratings yet
- Microbiology - Bio LibretextDocument782 pagesMicrobiology - Bio LibretextJomsEve Ison100% (2)
- Central Dogma and Genetic MedicineDocument4 pagesCentral Dogma and Genetic MedicineedricNo ratings yet
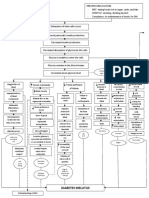
- Diabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)Document3 pagesDiabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)John Henry ValenciaNo ratings yet
- Mythos World Resources Vol 1Document20 pagesMythos World Resources Vol 1Dániel Sebestyén100% (1)
- Domiciliary Oxygen Therapy - Summary of IndicationsDocument4 pagesDomiciliary Oxygen Therapy - Summary of IndicationsAdina BatajuNo ratings yet
- A History of Britain 1945 Through Brexit Jeremy Black Full ChapterDocument51 pagesA History of Britain 1945 Through Brexit Jeremy Black Full Chapteralice.cousin115100% (18)
- 1 B. Teknologi Sel Punca Terapi HatiDocument12 pages1 B. Teknologi Sel Punca Terapi HatiarisNo ratings yet
- First Wave of Covid-19 in India and Indonesia-Laptop-Ieskoko7Document37 pagesFirst Wave of Covid-19 in India and Indonesia-Laptop-Ieskoko7Vivek NeelakantanNo ratings yet
- Pathology Mcqs Week 11: 1. in Adult Respiratory Distress SyndromeDocument4 pagesPathology Mcqs Week 11: 1. in Adult Respiratory Distress Syndromeمجتبى علي100% (5)
- Challenging Neurological Manifestations in Large Cell Neuroendocrine Carcinoma Lcnec A Case Study of Extensive Intracranial and Intradural MetastasesDocument3 pagesChallenging Neurological Manifestations in Large Cell Neuroendocrine Carcinoma Lcnec A Case Study of Extensive Intracranial and Intradural MetastasesHerald Scholarly Open AccessNo ratings yet
- Infectious Disease NotesDocument23 pagesInfectious Disease NotesaparnaNo ratings yet
- Scientific Research Journal of India SRJI Vol-3 Issue-3 Year 2014Document209 pagesScientific Research Journal of India SRJI Vol-3 Issue-3 Year 2014Dr. Krishna N. SharmaNo ratings yet
- 3RD Periodical Exam G10Document3 pages3RD Periodical Exam G10Erika Leonardo100% (2)