You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Personalized Diet PDFDocument38 pagesPersonalized Diet PDFbuhaptserenNo ratings yet
- Semi Detailed Lesson Plan in HealhtDocument2 pagesSemi Detailed Lesson Plan in HealhtJeriel Baton Seguido100% (6)
- When A Parent Dies - A Systematic Review of The Effects of Support Programs For Parentally Bereaved Children and Their CaregiversDocument15 pagesWhen A Parent Dies - A Systematic Review of The Effects of Support Programs For Parentally Bereaved Children and Their CaregiversSorina ElenaNo ratings yet
- Respirology - 2012 - SIERRA VARGAS - Air Pollution Impact and PreventionDocument8 pagesRespirology - 2012 - SIERRA VARGAS - Air Pollution Impact and PreventionSorina ElenaNo ratings yet
- Enhancing The Role of Private Practitioners in Tuberculosis Prevention and Care Activities in IndiaDocument7 pagesEnhancing The Role of Private Practitioners in Tuberculosis Prevention and Care Activities in IndiaSorina ElenaNo ratings yet
- The Grief and Bereavement Experiences of Informal Caregivers: A Scoping Review of The North American LiteratureDocument17 pagesThe Grief and Bereavement Experiences of Informal Caregivers: A Scoping Review of The North American LiteratureSorina ElenaNo ratings yet
- 2020 Article 5324Document8 pages2020 Article 5324Sorina ElenaNo ratings yet
- Tuberculosis Vaccines and Prevention of InfectionDocument22 pagesTuberculosis Vaccines and Prevention of InfectionSorina ElenaNo ratings yet
- Towards New TB Vaccines: Seminars in ImmunopathologyDocument17 pagesTowards New TB Vaccines: Seminars in ImmunopathologySorina ElenaNo ratings yet
- Tuberculosis Prevention in Children: A Prospective Community-Based Study in South AfricaDocument10 pagesTuberculosis Prevention in Children: A Prospective Community-Based Study in South AfricaSorina ElenaNo ratings yet
- MDR-TB Treatment As Prevention: The Projected Population-Level Impact of Expanded Treatment For Multidrug-Resistant TuberculosisDocument16 pagesMDR-TB Treatment As Prevention: The Projected Population-Level Impact of Expanded Treatment For Multidrug-Resistant TuberculosisSorina ElenaNo ratings yet
- Too Little Too Late: Waiting For TB To Come: SciencedirectDocument3 pagesToo Little Too Late: Waiting For TB To Come: SciencedirectSorina ElenaNo ratings yet
- Drug-Resistant TB: Deadly, Costly and in Need of A VaccineDocument6 pagesDrug-Resistant TB: Deadly, Costly and in Need of A VaccineSorina ElenaNo ratings yet
- Prevention of TB Using Rifampicin Plus Isoniazid Reduces Nevirapine Concentrations in HIV-exposed InfantsDocument7 pagesPrevention of TB Using Rifampicin Plus Isoniazid Reduces Nevirapine Concentrations in HIV-exposed InfantsSorina ElenaNo ratings yet
- TB Anywhere Is TB Everywhere: Commentary Open AccessDocument3 pagesTB Anywhere Is TB Everywhere: Commentary Open AccessSorina ElenaNo ratings yet
- The Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) Trial: Baseline CharacteristicsDocument12 pagesThe Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) Trial: Baseline CharacteristicsSorina ElenaNo ratings yet
- M. Tuberculosis Infection in HIV-exposedDocument9 pagesM. Tuberculosis Infection in HIV-exposedSorina ElenaNo ratings yet
- Obesity and Diabetes As High-Risk Factors For Severe Coronavirus Disease 2019 (Covid-19)Document14 pagesObesity and Diabetes As High-Risk Factors For Severe Coronavirus Disease 2019 (Covid-19)Sorina ElenaNo ratings yet
- Review: SM Kotila, L Payne Hallström, N Jansen, P Helbling, I AbubakarDocument12 pagesReview: SM Kotila, L Payne Hallström, N Jansen, P Helbling, I AbubakarSorina ElenaNo ratings yet
- Jix 362Document7 pagesJix 362Sorina ElenaNo ratings yet
- Nonproteinuric Diabetic Kidney DiseaseDocument9 pagesNonproteinuric Diabetic Kidney DiseaseSorina ElenaNo ratings yet
- COVID-19 and The Kidney: ReviewDocument13 pagesCOVID-19 and The Kidney: ReviewSorina ElenaNo ratings yet
- Neural Stem Cell Transplantation For Neurodegenerative DiseasesDocument21 pagesNeural Stem Cell Transplantation For Neurodegenerative DiseasesSorina ElenaNo ratings yet
- New England Journal Medicine: The ofDocument13 pagesNew England Journal Medicine: The ofSorina ElenaNo ratings yet
- COVID19 Vaccination Guidefor Eligible BeneficiariesDocument16 pagesCOVID19 Vaccination Guidefor Eligible BeneficiariesKartik R. MorjariaNo ratings yet
- Panduan Penyakit Menular - Dr. Galih Endradita MDocument15 pagesPanduan Penyakit Menular - Dr. Galih Endradita Msri wahyuniNo ratings yet
- Issue Over Vaccines Newsela 9Document8 pagesIssue Over Vaccines Newsela 9api-311995468No ratings yet
- Job Responsibilities of Medical OfficersDocument8 pagesJob Responsibilities of Medical OfficersKailash NagarNo ratings yet
- Comorbidity: Apakah Merupakan Faktor Risiko: Infeksi Luka Operasi Pasca Seksio Sesarea?Document10 pagesComorbidity: Apakah Merupakan Faktor Risiko: Infeksi Luka Operasi Pasca Seksio Sesarea?Dini AgustiniNo ratings yet
- Care For Elderly - TAGALOGDocument29 pagesCare For Elderly - TAGALOGKarl Kevin MarbellaNo ratings yet
- Dugayo Activity 1Document1 pageDugayo Activity 1Ozen YuNo ratings yet
- Principles of Hospital Disaster PlanningDocument79 pagesPrinciples of Hospital Disaster PlanningRoman MamunNo ratings yet
- National Polio Laboratory Check List For Annual WHO AccreditationDocument12 pagesNational Polio Laboratory Check List For Annual WHO AccreditationSelaina NawadraNo ratings yet
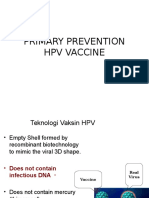
- Vaksin HPVDocument14 pagesVaksin HPVsutianiNo ratings yet
- The Process of Reproduction and Sexual Health and HygieneDocument28 pagesThe Process of Reproduction and Sexual Health and HygieneMila MagistradoNo ratings yet
- MMR 2 Vaccine InsertDocument11 pagesMMR 2 Vaccine InsertJonNo ratings yet
- Kasus Ujian PhantomDocument4 pagesKasus Ujian PhantomMishael Octaviany JirehNo ratings yet
- Nursing Management During Labor and BirthDocument23 pagesNursing Management During Labor and BirthShiella May Edquibal0% (1)
- Occupational Health and Safety For Health Workers in The Context of COVID-19Document19 pagesOccupational Health and Safety For Health Workers in The Context of COVID-19Tayib JabbarNo ratings yet
- Hydatidiform Mole: Incidence and Management Outcomes in A Tertiary Hospital in AbujaDocument5 pagesHydatidiform Mole: Incidence and Management Outcomes in A Tertiary Hospital in AbujaSasa MicinNo ratings yet
- Vision: Mabini Colleges Shall Cultivate A Culture of Excellence in EducationDocument3 pagesVision: Mabini Colleges Shall Cultivate A Culture of Excellence in EducationSharina Canaria ObogNo ratings yet
- Bardhan-Reflections On Indian Political EconomyDocument4 pagesBardhan-Reflections On Indian Political EconomyBhowmik ManasNo ratings yet
- Majalah Kesehatan Indonesia: Faktor-Faktor Penyebab Kejadian Stunting Pada BalitaDocument12 pagesMajalah Kesehatan Indonesia: Faktor-Faktor Penyebab Kejadian Stunting Pada BalitaAhmad SugihartoNo ratings yet
- Company Profile in EnglishDocument60 pagesCompany Profile in EnglishAllyraNo ratings yet
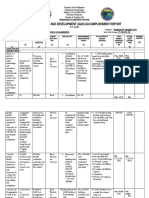
- Annual Gender and Development (Gad) Accomplishment Report: Variance/ RemarksDocument4 pagesAnnual Gender and Development (Gad) Accomplishment Report: Variance/ RemarkslorynelNo ratings yet
- Tuberculosis Mnemonics - Group 3 PDFDocument2 pagesTuberculosis Mnemonics - Group 3 PDFMaria Lea YemaNo ratings yet
- Maternal Health - Blogs Comment On Women Deliver Conference, Birth Control Coverage, Other Topics (Medical News Today - 10 June 2010)Document3 pagesMaternal Health - Blogs Comment On Women Deliver Conference, Birth Control Coverage, Other Topics (Medical News Today - 10 June 2010)National Child Health Resource Centre (NCHRC)No ratings yet
- Cert. of AcceptanceDocument3 pagesCert. of AcceptanceJessica CindyNo ratings yet
- GFSFDocument9 pagesGFSFRajendra SinghNo ratings yet
- 32 Okuthe Fao Isavet and VlcsDocument15 pages32 Okuthe Fao Isavet and VlcsObo KeroNo ratings yet
- Duh Tubuh Wanita, DR SAYU.,SpKK, WMDocument62 pagesDuh Tubuh Wanita, DR SAYU.,SpKK, WMdickypranataNo ratings yet
- Hand WashingDocument29 pagesHand WashingLharra Cagulada-PostranoNo ratings yet