You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- AHA ACLS Post Test Answer Key 2023Document33 pagesAHA ACLS Post Test Answer Key 2023c100% (10)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
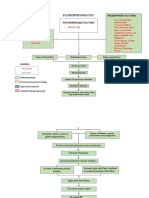
- Pathophysiology of Pulmonary Embolism (Loria.J)Document2 pagesPathophysiology of Pulmonary Embolism (Loria.J)Justine Mae Loria0% (1)
- Chapter 26 PULMONARY VASCULAR DISEASEDocument10 pagesChapter 26 PULMONARY VASCULAR DISEASEZahra Margrette SchuckNo ratings yet
- EKG Flash CardsDocument5 pagesEKG Flash CardsRyann Sampino FreitasNo ratings yet
- Heart SoundsDocument20 pagesHeart Soundsshd9617No ratings yet
- Neurology XXXXDocument13 pagesNeurology XXXXAmeer AslamNo ratings yet
- NCM 118 CARDIO LECTURE LIFE THREATENING EMERGENCY CONGESTIVE HEART FAILURE MVIMMACULATA 2021 For Canvas-1Document46 pagesNCM 118 CARDIO LECTURE LIFE THREATENING EMERGENCY CONGESTIVE HEART FAILURE MVIMMACULATA 2021 For Canvas-1Pollen Siega BunalNo ratings yet
- Acute Kidney InjuryDocument31 pagesAcute Kidney InjuryShaista ZarreenNo ratings yet
- The Junior Doctor's Guide To Gastroenterology (Sep 22, 2011) - (1846193524) - (CRC Press) PDFDocument153 pagesThe Junior Doctor's Guide To Gastroenterology (Sep 22, 2011) - (1846193524) - (CRC Press) PDFmadimadi11No ratings yet
- Summary of Face Reading in Chinese MedicineDocument25 pagesSummary of Face Reading in Chinese MedicineDoña InesNo ratings yet
- Breast Self ExaminationDocument18 pagesBreast Self ExaminationjenrastaNo ratings yet
- CHF With Obstructive UropathyDocument28 pagesCHF With Obstructive UropathyJohn OrtizNo ratings yet
- Dental Management in Medically Compromised Patients Hypertens IonDocument17 pagesDental Management in Medically Compromised Patients Hypertens Ionآلقہيہسہيہ مہجہآهہدNo ratings yet
- Case Study On DehydrationDocument4 pagesCase Study On DehydrationDustin Dela CruzNo ratings yet
- System Disorder: PneumothoraxDocument1 pageSystem Disorder: PneumothoraxEli ReyesNo ratings yet
- Thoracic Aortic AneurysmsDocument4 pagesThoracic Aortic AneurysmsJoan Melissa SomeraNo ratings yet
- Cataract White ArmyDocument16 pagesCataract White Armyamraayman21No ratings yet
- Newborn Physiology PathologyDocument99 pagesNewborn Physiology Pathologythev0206100% (1)
- Nursing Care of Client With Life Threatening Conditions Acute Ill, Multi-Organ Problems High Acuity and Emergency SituationsDocument43 pagesNursing Care of Client With Life Threatening Conditions Acute Ill, Multi-Organ Problems High Acuity and Emergency SituationsGlaiza Fabia100% (1)
- Grade 2 Edema On Arms and Legs (Grade 2 Periorbital Edema: Additional Not From The Searched Case StudyDocument3 pagesGrade 2 Edema On Arms and Legs (Grade 2 Periorbital Edema: Additional Not From The Searched Case StudyKim Glaidyl BontuyanNo ratings yet
- PATH 1 ALL Lectures Final1Document2,054 pagesPATH 1 ALL Lectures Final1Andleeb Imran100% (1)
- The ECG in Hypothermia - Osborn WavesDocument2 pagesThe ECG in Hypothermia - Osborn WavesVid MirosevicNo ratings yet
- DRUG STUDY AtorvastatinDocument1 pageDRUG STUDY AtorvastatinKyla BeconiaNo ratings yet
- Cardiovascular System - 4th EdDocument33 pagesCardiovascular System - 4th EdLeah ArabesNo ratings yet
- P0St-Operative Care: Presented by Monika Devi M.SC (N) HCN, SrhuDocument20 pagesP0St-Operative Care: Presented by Monika Devi M.SC (N) HCN, SrhuOng KarlNo ratings yet
- Heart EmbryologyDocument27 pagesHeart EmbryologyAlena JosephNo ratings yet
- Ton Mitral Valve ReplacementDocument3 pagesTon Mitral Valve ReplacementSony TonNo ratings yet
- Hypertension: Signs and SymptomsDocument7 pagesHypertension: Signs and SymptomsAdinia NugrahiniNo ratings yet
- 1b. Pediatrics Subject Exam - Content Outline - NBMEDocument8 pages1b. Pediatrics Subject Exam - Content Outline - NBMEmeiraimNo ratings yet
- Hyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesDocument6 pagesHyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesLeitavia D.No ratings yet