Professional Documents
Culture Documents
Clinical Performance of Direct Versus Indirect
Uploaded by
Cristian FernandoOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Clinical Performance of Direct Versus Indirect
Uploaded by
Cristian FernandoCopyright:
Available Formats
[Downloaded free from http://www.jcd.org.in on Thursday, February 22, 2018, IP: 61.16.135.
114]
Review Article
Clinical performance of direct versus indirect
composite restorations in posterior teeth:
A systematic review
Rubeena Abdul Azeem, Nivedhitha Malli Sureshbabu
Department of Conservative Dentistry and Endodontics, Saveetha Dental College, Saveetha University, Chennai, Tamil Nadu, India
Abstract
Background: Composite resin, serves as esthetic alternative to amalgam and cast restorations. Posterior teeth can be restored
using direct or indirect composite restorations. The selection between direct and indirect technique is a clinically challenging
decision‑making process. Most important influencing factor is the amount of remaining tooth substance.
Aim: The aim of this systematic review was to compare the clinical performance of direct versus indirect composite restorations
in posterior teeth.
Materials and Methods: The databases searched included PubMed CENTRAL (until July 2015), Medline, and Cochrane
Database of Systematic Reviews. The bibliographies of clinical studies and reviews identified in the electronic search were
analyzed to identify studies which were published outside the electronically searched journals. The primary outcome measure
was evaluation of the survival of direct and indirect composite restorations in posterior teeth.
Results: This review included thirteen studies in which clinical performance of various types of direct and indirect composite
restorations in posterior teeth were compared. Out of the thirteen studies which were included seven studies had a high risk of
bias and five studies had a moderate risk of bias. One study having a low risk of bias, concluded that there was no significant
difference between direct and indirect technique. However, the available evidence revealed inconclusive results.
Conclusion: Further research should focus on randomized controlled trials with long term follow-up to give concrete evidence
on the clinical performce of direct and indirect composite restorations.
Keywords: Clinical evaluation; indirect technique; posterior teeth; single‑visit direct composite restorations, survival rate
INTRODUCTION Ceramic restorations have the disadvantages of being
expensive, brittle, prone to fracture and can induce wear
Increase in demand for esthetics has led to the development with opposing tooth’s surface.[2] Recently, there has been
of tooth‑colored, nonmetallic restorations such as direct increase in the use of resin composites in posterior teeth.
composite restorations, indirect composite inlays, and Composites typically involve filler particles dispersed
ceramic inlays or onlays.[1] within a matrix phase.
Among the currently available composite materials, hybrid,
Address for correspondence: microfilled and nanofilled composites are commonly
Dr. Rubeena Abdul Azeem, Department of Conservative being used for posterior restorations. Microfilled
Dentistry and Endodontics,Saveetha Dental College, Saveetha
University, 162, Poonamallee High Road, Velappanchavadi, composites have 37%–40% volume filler loading, whereas
Chennai - 600 077, Tamil Nadu, India. nanofilled composites have 60% volume filler loading.[3]
E-mail: DrRubeenaAbdulAzeem@gmail.com Nanofilled composites show high translucency similar to
Date of submission : 08.08.2016
Review completed : 21.11.2017 This is an open access article distributed under the terms of the Creative
Date of acceptance : 25.12.2017 Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which
allows others to remix, tweak, and build upon the work non‑commercially,
as long as the author is credited and the new creations are licensed under
Access this article online the identical terms.
Quick Response Code: For reprints contact: reprints@medknow.com
Website:
www.jcd.org.in
How to cite this article: Azeem RA, Sureshbabu NM. Clinical
performance of direct versus indirect composite restorations
DOI: in posterior teeth: A systematic review. J Conserv Dent
10.4103/JCD.JCD_213_16
2018;21:2-9.
2 © 2018 Journal of Conservative Dentistry | Published by Wolters Kluwer - Medknow
[Downloaded free from http://www.jcd.org.in on Thursday, February 22, 2018, IP: 61.16.135.114]
Azeem and Sureshbabu: Direct versus indirect composite restorations in posterior teeth - SR
microfilled composites and physical properties similar to Indirect inlay system requires an impression to fabricate
hybrid composite.[4] In addition to being esthetic, these the inlay in the laboratory. In addition to conventional
materials are relatively less expensive, induce lesser wear light‑curing and heat‑curing for polymerization,
of opposing tooth structure and are based on the principle laboratory processing may use heat (140°C), pressure
of minimally invasive procedure. (0.6 MPa for 10 min) and nitrogen atmosphere. These
materials have improved physical properties, resistance
There are different techniques for placement of composite to wear and attain a higher degree of polymerization. The
resin restorations. It includes direct and indirect polymerization shrinkage does not occur in the prepared
technique. The selection between direct and indirect tooth, so induced stresses are reduced which reduces the
technique is a challenging decision making process. potential for leakage.
Single visit direct posterior composite restorations allows
for preservation of tooth structure.[5] In this technique, To overcome the disadvantages of first generation indirect
following etching and application of bonding agent to composites, in the early 1990s, a second generation
the prepared cavity, composite restoration is built up of indirect composites was introduced which included
in increments, curing one layer at a time allowing the microhybrid composites with fillers of approximately 66%
practitioner to sculpt the restoration. Hence, cavities are by volume. This resulted in improved mechanical properties
filled incrementally with facially and lingually inclined with flexural strength in the range of 120–160 MPa and
mesiodistal layers of maximum 2 mm. The layering elastic modulus of 8.5–12 GPa.[8]
technique effectively reduces polymerization stress by
minimizing the C‑factor. As the C‑factor reduces, the Composite inlays provide better contouring of proximal
bond strength increases. surfaces, occlusal contacts, improved wear resistance,
reduced polymerization shrinkage, improved fracture
Advantages of direct technique include increased strength resistance, and biocompatibility.[9] The drawbacks of
of remaining tooth structure and potential for repair. composite inlays are increased cost and time, requires two
However, mechanical strength of these restorations is appointments, fabrication of a temporary restoration, and
inferior to that of indirect composite restorations. Other low potential for repair.
disadvantages include occlusal and proximal wear, surface
roughness, marginal discoloration, loss of marginal Hence, the selection between direct and indirect composite
integrity, postoperative sensitivity, secondary caries, cusp restorations is challenging. Many clinical studies have been
flexure, technique sensitive, less‑than‑ideal bonding to performed on success or survival rate of direct and indirect
dentin, and low fracture toughness. composite restorations individually. Very few articles
have studied comparing direct versus indirect composite
Indirect technique refers to fabrication of the restoration restorations. Hence, the primary objective of this systematic
outside the oral cavity in the laboratory following which review was to compare the clinical performance of direct
it is luted to the tooth with resin cement. There are two versus indirect composite restorations in posterior teeth.
types of indirect composite restorations, first and second
generation of indirect composite restorations.
Aim
This systematic review aimed at comparing the clinical
The first generation of indirect composite restorations was
performance of direct versus indirect composite
introduced in the 1980s. These restorations have shown
restorations in posterior teeth.
failures in clinical studies. In spite of their secondary curing,
they exhibited low levels of flexural strength (60–80 MPa)
and elastic modulus (2–3.5 GPa), a resin volume more than Structured question
50% and higher wear levels.[6] Is there a better clinical performance of direct composite
restorations when compared with indirect composite
The fabrication process differs for direct composite inlays restorations in posterior teeth?
and indirect inlays. For direct composite inlays first a
separating medium is applied to the prepared tooth. The MATERIALS AND METHODS
resin pattern is then formed, light‑cured and removed
from the preparation. The rough inlay is then exposed to Sources used
additional light for approximately 4–6 min or heat activated For identification of studies included or considered for
at 110ºC for 7 min, after which the preparation is etched, this review, detailed search was done in the following
the inlay is cemented into place with a dual‑cure resin, and databases:
is then polished. This technique can be completed in a • PubMed advanced search (until July 2015)
single sitting since it eliminates the need for an impression • Medline
of the cavity.[7] • Cochrane Database of Systematic Reviews.
Journal of Conservative Dentistry | Volume 21 | Issue 1 | January-February 2018 3
[Downloaded free from http://www.jcd.org.in on Thursday, February 22, 2018, IP: 61.16.135.114]
Azeem and Sureshbabu: Direct versus indirect composite restorations in posterior teeth - SR
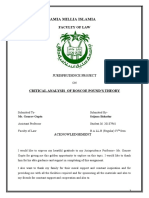
Language Therefore, a total of 13 publications fulfilled all criteria
No language restrictions were applied during the electronic for inclusion. [Chart 1 shows the search flowchart, general
search. Articles with translations of foreign language information of selected articles are given in Tables 1 and 2
available were included to eliminate possible language shows the evidence level of selected articles, Table 3 shows
bias. the risk of bias– major criteria and outcome of included
studies are given in Table 4]. Graph 1 shows the sample size
Hand searching distribution and Graph 2 shows the survival rate.
Journal of Restorative Dentistry.
DISCUSSION
Types of studies
Studies included were randomized controlled trials and A total of 1466 teeth were included in this review. Out
clinical trials comparing direct and indirect composite of 1466 teeth, 741 teeth received direct composite
restorations. restorations and 725 teeth received indirect composite
restorations. Age group of the patients was <55 years.
Inclusion criteria
Patients 18–55 years of age with vital posterior teeth. Of the thirteen studies included in this review, three were
randomized controlled clinical trials and remaining 10 were
Exclusion criteria comparative clinical trials. Follow‑up period was 6 years,
The studies which were excluded are: 2 years, 11 years, 5 years, 3 years, 1 year, 1 year, 1 year,
• Case reports/case series 3 years, 5 years, 3 years, 1 year, and 2 years, respectively.
• Animal studies All the patients in whom various types of restorations
• In vitro studies were placed were followed up and variables assessed
• Studies not meeting the inclusion criteria were as follows: surface texture, marginal discoloration,
• Studies in which direct and indirect composite color match, anatomic form, retention, marginal integrity,
restorations have not been compared. gingival adaptation, postoperative symptoms, occlusion,
patient compliance, sensitivity, restoration integrity, tooth
RESULTS integrity, and secondary caries.
Description of studies Owing to the heterogeneity among the studies such as
The search identified 117 publications, of which 88 were differences in the composite type, sample size and follow-
excluded after reviewing the title or abstract. Full articles up period, we could not perform a meta-analysis.
were obtained for 29 studies; 18 of these publications
were excluded after reading the full text article. Hence, Interpretation of results
a total of 11 articles fulfilled the inclusion criteria. Two According to Karaarslan et al.,[10] the study was performed
handsearched articles fulfilled the inclusion criteria. on seventy patients. 140 teeth were equally divided
into two groups (n = 70). Seventy patients were in
Records identified through Additional records identified Group‑I (direct composite): Gradia Posterior (GP),
Identification
database searching
(n = 117)
through other sources
(n = 2)
P60 (Filtek P60 [FP]), Surefil Posterior (SP), and Bisco Aelite
LS Packable (BAP) and Group‑II (indirect composite): GP,
FP, SP and Tescera ATL (TATL) system TESCERA™ ATL™
Records after duplicates removed (Aqua, Thermal, Light) [Table 1]. Variables evaluated
(n = 119)
were surface texture, marginal discoloration, color
Screening
match, retention, marginal integrity, gingival adaptation,
postoperative symptoms, and secondary caries. This study
Records screened Records excluded
(n = 31) (n = 88) concluded that indirect restorations have less surface
roughness, postoperative sensitivity, and soft‑tissue
Full-text articles excluded, with irritation than direct restorations. The clinical performances
Eligibility
reasons (n = 18)
• No comparison (n = 14) of the indirect restorations were more satisfactory than the
Full-text articles assessed • Restorations were not evaluated
for eligibility according to USPHS criteria direct restorations.
(n = 13) (n = 3)
• Study was done in pediatric
patients (n = 1) According to Fennis et al.,[11] 176 premolars in
Included
Studies included in
157 patients were divided into two groups, namely,
qualitative synthesis Group‑I (direct composite):AP‑X (n = 92) and Group‑II
(n = 13)
(indirect composite): Estenia (n = 82) [Table 1]. In this study,
Chart 1: Search flow chart retention variable was evaluated. This study concluded that
4 Journal of Conservative Dentistry | Volume 21 | Issue 1 | January-February 2018
[Downloaded free from http://www.jcd.org.in on Thursday, February 22, 2018, IP: 61.16.135.114]
Azeem and Sureshbabu: Direct versus indirect composite restorations in posterior teeth - SR
Table 1: General information of selected articles
Author and Study design Sample size Age Materials used Variables evaluated
year Direct composite Indirect composite
Karaarslan Clinical study 70 subjects 18-55 years *GP, FP, SP and BAP *GP, FP, SP and 1, 2, 3, 5, 6, 7, 8, 14
et al., 2014[10] (140 teeth) (n=70) TATL system
32 ‑ male (n=70)
38 ‑ female
Fennis Randomized 157 subjects 35-81 years, AP‑X (hybrid resin Estenia (hybrid 5
et al., 2014[11] control trial, (176 premolars) 54.9 years composite) (n=92) ceramic) (n=84)
blocked 77 ‑ male (mean)
randomization 80 ‑ female
Ozakar‑Ilday Clinical trial 49 subjects 32 years (mean) Valux plus (n=20) DI system (hybrid 1, 2, 3, 4, 6, 8, 9, 10, 11, 12, 13
et al., 2013[12] 28 ‑ male composite), TATL
21 ‑ female system (microhybrid
composite) (n=40)
Cetin Clinical trial 54 subjects 20-28 years, #Nanofilled #TATL 1, 2, 3, 5, 6, 7, 8, 14
et al., 2013[13] (108 teeth) 23 years (mean) composite: FSXT, (microhybrid), E
22 ‑ men TEC (nanohybrid), (hybrid ceramic)
32 ‑ women AA (reinforced (n=41)
nanofill) (n=67)
Mendonça Clinical study 30 subjects 18-45 years, Tetric ceram (n=44) Targis (n=32) 1, 2, 3, 4, 6, 14
et al., 2010[14] (76 teeth) 29.8 (mean)
15 ‑ men
15 ‑ women
Cetin and Clinical study 54 subjects 20-28 years, #Nanofilled #TATL 1, 2, 3, 4, 5, 6, 7, 8
Unlu, 2009[15] 22 ‑ male 23 years (mean) composite: FSXT, (microhybrid),
32 ‑ female TEC (nanohybrid), E (hybrid ceramic)
(100 teeth) AA (reinforced (n=20/group)
nanofill) (n=20/
group)
Bartlett and Randomized Tooth wear Tooth wear Heliomolar New microfilled 2, 3, 4, 6, 10, 12, 13, 14
Sundaram, clinical trial group: group: 25- HB (microfilled resin resin composite
2006[16] 16 subjects, 62 years, composite) (n=29) (n=29)
control group: 43 years (mean), Tooth wear group: 16, Tooth wear group:
13 subjects control group: control group: 13 16, control group:
28-65 years, 13
39 years (mean)
Pallesen and Randomized 28 subjects 19-64 years, +BD and EP (n=56) +BD, EP and ISO 1, 2, 3, 4, 6, 14
Qvist, 2003[17] clinical study 8 ‑ male 35 years (mean) (n=84)
20 ‑ female
(88 premolars,
52 molars)
Manhart Prospective, 45 subjects Tetric, blend‑a‑lux, Tetric, blend‑a‑lux, 1, 2, 3, 4, 6, 8, 9, 10, 11, 12, 13
et al., 2000[18] clinical trial (37 premolars, Pertac‑hybrid unifil Pertac‑hybrid unifil
23 molars) (hybrid composite) (hybrid composite)
(n=30) (n=30)
Wassell Clinical study 73 subjects 29.6±10.3 years Coltene BD (small Coltene BD (small 1, 2, 3, 6, 7, 8, 9, 14
et al., 2000[19] 19 ‑ male (mean) particle hybrid particle hybrid
54 ‑ female composite) (n=100) composite) (n=100)
Scheibenbogen‑ Prospective, 45 subjects Tetric, blend‑a‑lux, Tetric, blend‑a‑lux, 1, 2, 3, 4, 6, 8, 9, 10, 11, 12, 13
Fuchsbrunner clinical trial (37 premolars, Pertac‑hybrid unifil Pertac‑hybrid unifil
et al., 1999[20] 23 molars) (hybrid composite) (hybrid composite)
(n=30) (n=30)
Scheibenbogen Prospective, 45 subjects 25-63 years, Tetric, blend‑a‑lux, Tetric, blend‑a‑lux, 1, 2, 3, 4, 6, 8, 9, 10, 11, 12, 13
et al., 1997[21] clinical trial (65 premolars, 37 years (mean) Pertac‑hybrid unifil Pertac‑hybrid unifil
23 molars) (hybrid composite) (hybrid composite)
(n=43) (n=45)
Wassell Clinical study 73 subjects 29.6±10.3 years Coltene BD (small Coltene BD (small 1, 2, 3, 6, 7, 8, 9, 14
et al., 1995[22] 19 ‑ male (mean) particle hybrid particle hybrid
54 ‑ female composite) (n=100) composite) (n=100)
*1 ‑ GP: Gradia posterior, FP: Filtek P60, SP: Surefil posterior, BAP: Bisco Aelite LS Packable, #4, 6 ‑ FSXT: Filtek Supreme XT, TEC: Tetric EvoCeram,
AA: AELITE Aesthetic, TATL: Tescera ATL, E: Estenia, +8 ‑ BD: Brilliant dentin, EP: Estilux posterior, ISO: SR‑Isosit. Variable 1: Surface texture,
Variable 2: Marginal discoloration, Variable 3: Color match, Variable 4: Anatomic form, Variable 5: Retention, Variable 6: Marginal integrity, Variable 7: Gingival
adaptation, Variable 8: Postoperative symptoms, Variable 9: Occlusion, Variable 10: Patient compliance, Variable 11: Sensitivity, Variable 12: Restoration integrity, Variable
13: Tooth integrity, Variable 14: Secondary caries
there was no statistically significant difference between According to Ozakar‑Ilday et al.,[12] 49 individuals were
direct and indirect restorations. divided into two groups. Group‑I (direct composite): Valux
Journal of Conservative Dentistry | Volume 21 | Issue 1 | January-February 2018 5
[Downloaded free from http://www.jcd.org.in on Thursday, February 22, 2018, IP: 61.16.135.114]
Azeem and Sureshbabu: Direct versus indirect composite restorations in posterior teeth - SR
plus (n = 20), Group‑II (indirect composite): DI system and evaluated: surface texture, marginal discoloration, color
TATL system (n = 40). The results of this study concluded match, anatomic form, marginal integrity, and secondary
that indirect resin restorations showed better scores than caries. The results of this study concluded that direct
direct composite restorations. restorations performed better than indirect composite
inlays for marginal integrity.
According to Cetin et al.,[13] 108 teeth in a group of 54
individuals were included and distributed into two groups. According to Cetin and Unlu,[15] 100 teeth in 54 patients
Group‑I (direct composite): Filtek Supreme XT (FSXT), were divided into two groups of 20 restorations per
Tetric EvoCeram (TEC) and AELITE Aesthetic (AA) (n = 67), group (n = 20). Group‑I (Direct composite): FSXT, TEC,
Group‑II (indirect composite): TATL and E (n = 41) [Table 1]. and AA (n = 20/group) and Group‑II (Indirect composite):
Variables evaluated in this study were surface texture, TATL and E (n = 20/group) [Table 1]. Variables evaluated
marginal discoloration, color match, retention, marginal in this study were surface texture, marginal discoloration,
integrity, gingival adaptation, postoperative symptoms, color match, anatomic form, retention, marginal integrity,
and secondary caries. This study concluded that there was gingival adaptation, and postoperative symptoms. This
no statistically significant difference between direct and study concluded that there was no statistically significant
indirect restorations. difference between direct and indirect restorations.
According to Mendonça et al.,[14] 76 teeth in 30 patients According to Bartlett and Sundaram,[16] 16 patients were
were divided into two groups: Group‑I (Direct composite): included in tooth wear group and 13 patients in control
Tetric Ceram (n = 44) and Group‑II (indirect composite): group. Twenty‑nine direct and indirect restorations were
Targis (n = 32) [Table 1]. The following variables were placed [Table 1]. The results of this study concluded that
the use of direct and indirect composite restorations in
worn posterior teeth is contraindicated.
Table 2: Evidence level of selected articles
Author Study design Level of evidence According to Pallesen and Qvist,[17] 140 teeth in
ES Karaarslan et al., 2014 Clinical study 3 28 individuals were divided into Gr‑I (Direct composite):
WM Fennis et al., 2014 Randomized 2
control trial,
Brilliant Dentin (BD) and Estilux posterior (EP) (n = 56)
blocked and Group‑II (indirect composite): BD, EP and
randomization ISO (n = 84) [Table 1]. This study revealed no difference in
N Ozakar‑Ilday et al., 2013 Clinical trial 3 the long‑term performance of direct restorations or inlays
AR Cetin et al., 2013 Clinical trial 3
Mendonca JS et al., 2010 Clinical study 3
made from the same material.
AR Cetin and N Unlu, 2009 Clinical study 3
D Bartlett and G Randomized 2 According to Manhart et al.[18] 60 teeth in 45 patients
Sundaram, 2006 clinical trial were distributed equally into Group‑I (Direct composite):
Ulla Pallesen and Vibeke Randomized 2
Qvist, 2003 clinical study
Tetric, Blend‑a‑lux, Pertac‑Hybrid Unifil (n = 30) and
J Manhart et al., 2000 Prospective, 3 Group‑II (Indirect composite): Tetric, Blend‑a‑lux,
clinical trial Pertac‑Hybrid Unifil (n = 30) [Table 1]. This study concluded
RW Wassell et al., 2000 Clinical study 3 that inlays exhibited better anatomic form of the surface
A Scheibenbogen‑Fuchsbrunner Prospective, 3
et al., 1999 clinical trial
than direct restorations.
A Scheibenbogen et al., 1997 Prospective, 3
clinical trial According to Wassell et al.,[19] 73 patients received 100 pairs
RW Wassell et al., 1995 Clinical study 3 of direct and indirect restorations made from the same
Table 3: Risk of bias‑major criteria
Study Randomization Allocation concealment Assessor blinded Dropouts described Risk of bias
ES Karaarslan et al., 2014 No No Unclear None High
WM Fennis et al., 2014 Yes No No Yes Moderate
N Ozakar‑Ilday et al., 2013 No No Unclear None High
AR Cetin et al., 2013 Yes No Unclear None High
Mendonca JS et al., 2010 No No Unclear None High
AR Cetin and N Unlu, 2009 No No Unclear None High
D Bartlett and G Sundaram, 2006 Unclear No No Yes High
Ulla Pallesen and Vibeke Qvist, 2003 Yes No No Yes Moderate
J Manhart et al., 2000 No No Yes Yes Moderate
RW Wassell et al., 2000 Yes No Yes Yes Low
A Scheibenbogen‑Fuchsbrunner et al., 1999 No No Yes Yes Moderate
A Scheibenbogen et al., 1997 No No No No High
RW Wassell et al., 1995 Yes No Yes No Moderate
6 Journal of Conservative Dentistry | Volume 21 | Issue 1 | January-February 2018
[Downloaded free from http://www.jcd.org.in on Thursday, February 22, 2018, IP: 61.16.135.114]
Azeem and Sureshbabu: Direct versus indirect composite restorations in posterior teeth - SR
Table 4: Outcome in the included studies summation tables for variables of interest
Author and year Longest follow up Study groups and outcomes at the longest follow up period
period Survival rate
Direct composite Indirect composite
ES Karaarslan et al., 2014 1 year GP, FP, SP and BAP (n=70; GP, FP, SP and TATL system (n=70; 100%)
100%)
WM Fennis et al., 2014 5.6 years for direct AP‑X (n=92; 91.2%) Estenia (n=84; 83.2%)
technique, 6 years
for indirect technique
N Ozakar‑Ilday et al., 2013 3 years Valux plus (n=20; 67%) DI system, TATL system (n=40)
DI system ‑ 86%, ATL system ‑ 93%
AR Cetin et al., 2013 5 years FSXT, TEC, AA (n=67; 98.4%) TATL, E (n=41; 97.5%)
Mendonca JS et al., 2010 1 year Tetric ceram (n=44; 100%) Targis (n=32; 100%)
AR Cetin and N Unlu, 2009 1 year FSXT, TEC, AA (n=20/group; TATL, E (n=20/group; 100%)
100%)
D Bartlett and G Sundaram, 2 years Heliomolar HB (n=29; 79%) New microfilled resin composite (n=29; 64%)
2006
Ulla Pallesen and Vibeke Qvist, 11 years BD and EP (n=56; 70%) BD, EP and ISO (n=84; 88%)
2003
J Manhart et al., 2000 3 years Tetric, blend‑a‑lux, Pertac‑hybrid Tetric, blend‑a‑lux, Pertac‑hybrid unifil (n=30;
unifil (n=30; 87%) 93%)
RW Wassell et al., 2000 5 years Coltene BD (n=100; 92.5%) Coltene BD (n=100; 82.6%)
A Scheibenbogen‑Fuchsbrunner 2 years Tetric, blend‑a‑lux, Pertac‑hybrid Tetric, blend‑a‑lux, Pertac‑hybrid unifil (n=30;
et al., 1999 unifil (n=30; 90%) 93%)
A Scheibenbogen et al., 1997 1 year Tetric, blend‑a‑lux, Pertac‑hybrid Tetric, blend‑a‑lux, Pertac‑hybrid unifil (n=45;
unifil (n=43; 85%) 85%)
RW Wassell et al., 1995 3 years Coltene BD (n=100; 96%) Coltene BD (n=100; 92%)
GP: Gradia posterior, FP: Filtek P60, SP: Surefil posterior, BAP: Bisco Aelite LS Packable, TATL: Tescera ATL, TEC: Tetric EvoCeram, FSXT: Filtek Supreme XT,
AA: AELITE Aesthetic, E: Estenia, BD: Brilliant dentin, EP: Estilux posterior, ISO: SR‑Isosit
Graph 1: Sample size distribution
Graph 2: Survival rate
material (Coltene BD) [Table 1]. This study concluded
that there was no significant difference in the clinical Unifil (n = 45) [Table 1]. The results of this study concluded
performance between direct and indirect technique and that for the criteria surface texture, anatomical form of
the direct inlay method gave no clinical advantage over surface and occlusion, inlays showed superior clinical
conventional, incremental placement technique. performance.
According to Scheibenbogen‑Fuchsbrunner et al.,[20] According to Wassell et al.[22] 73 patients received 100 pairs
60 teeth were divided into Group‑I (direct composite): of direct and indirect restorations made from the same
Tetric, Blend‑a‑lux, Pertac‑Hybrid Unifil (n = 30) and material (Coltene BD) [Table 1]. This study observed that
Group‑II (indirect composite): Tetric, Blend‑a‑lux, the clinical performance of both types of materials was
Pertac‑Hybrid Unifil (n = 30) [Table 1]. This study concluded similar.
that inlays demonstrated better anatomic form of the
surface than direct restorations. Defending the results
Indirect composite restorations have superior surface
According to Scheibenbogen et al.[21] 88 teeth were divided texture, anatomic form, occlusion, tooth integrity, lesser
into Group‑I (Direct composite): Tetric, Blend‑a‑lux, sensitivity, gingival bleeding and marginal discoloration
Pertac‑Hybrid Unifil (n = 43) and Group‑II (Indirect whereas direct composite restorations have shown superior
composite): Tetric, Blend‑a‑lux, Pertac‑Hybrid restoration integrity. However, the available evidence
Journal of Conservative Dentistry | Volume 21 | Issue 1 | January-February 2018 7
[Downloaded free from http://www.jcd.org.in on Thursday, February 22, 2018, IP: 61.16.135.114]
Azeem and Sureshbabu: Direct versus indirect composite restorations in posterior teeth - SR
reveals there was no significant difference in the clinical studies with high risk of bias, three studies reported that
performance between direct and indirect technique. The composite inlays showed superior clinical performance
direct inlay technique gave no clinical advantage over than direct composite restorations, another three studies
conventional, incremental placement. concluded that there was no significant difference between
direct and indirect composite restorations. One study
Quality of evidence reported that direct composite restorations performed
Three of the studies included in this review have a level better than indirect composite inlays for marginal integrity.
of evidence 2, whereas remaining ten studies have level Therefore, properly designed randomized controlled
of evidence 3. Three studies are randomized clinical trials, studies with long‑term follow‑up must be performed to
thus the level of evidence is high [Table 2]. One study had give concrete evidence on the clinical performance of
a low risk of bias. Five out of thirteen trials included in direct and indirect composite restorations.
this systematic review showed a “moderate” risk of bias,
whereas seven studies showed a “high” risk of bias [Table 3]. Financial support and sponsorship
Nil.
Report on outliers data
No outlier data obtained. Conflicts of interest
There are no conflicts of interest.
Inference
Indirect composite inlays showed superior clinical REFERENCES
performance to direct composite restorations in spite
1. Manhart J, Scheibenbogen‑Fuchsbrunner A, Chen HY, Hickel R.
of greater loss of tooth structure, more clinical steps A 2‑year clinical study of composite and ceramic inlays. Clin Oral
and procedure of fabrication and exhibited significantly Investig 2000;4:192‑8.
better anatomic form than direct composite restorations. 2. Burke EJ, Qualtrough AJ. Aesthetic inlays: Composite or ceramic? Br
Dent J 1994;176:53‑60.
However, there was no statistically significant difference 3. Lu H, Lee YK, Oguri M, Powers JM. Properties of a dental resin composite
in the clinical performance between direct and indirect with a spherical inorganic filler. Oper Dent 2006;31:734‑40.
4. Mitra SB, Wu D, Holmes BN. An application of nanotechnology in
technique. advanced dental materials. J Am Dent Assoc 2003;134:1382‑90.
5. Ericson D. What is minimally invasive dentistry? Oral Health Prev Dent
2004;2 Suppl 1:287‑92.
Direct and indirect composite restorations in molars 6. Peutzfeldt A. Indirect resin and ceramic systems. Oper Dent
showed significantly higher failure rate compared with 2001;200:1153‑76.
premolars. Restoration of worn posterior teeth using direct 7. Garber DA, Goldstein RE. Porcelain and Composite Inlays and Onlays.
Illinois: Quintessence Publishing Co. Inc.; 1994. p. 117‑33.
and indirect composite restorations is contraindicated. 8. Miara P. Aesthetic guidelines for second‑generation indirect inlay
and onlay composite restorations. Pract Periodontics Aesthet Dent
1998;10:423‑31.
Further studies must be performed with standard study 9. Howard NY. Advanced use of an esthetic indirect posterior resin system.
procedures and larger or adequate sample size to give Compend Contin Educ Dent 1997;18:1044‑6, 1048, 1050.
10. Karaarslan ES, Ertas E, Bulucu B. Clinical evaluation of direct
concrete evidence on the long term clinical performance composite restorations and inlays: Results at 12 months. J Res Dent
of direct and indirect composite restorations. Furthermore, 2014;2:70‑7.
there is a need for comparison of direct fiber‑reinforced 11. Fennis WM, Kuijs RH, Roeters FJ, Creugers NH, Kreulen CM.
Randomized control trial of composite cuspal restorations: Five‑year
composite and indirect composite restorations as no results. J Dent Res 2014;93:36‑41.
studies have been reported so far. 12. Ozakar‑Ilday N, Zorba YO, Yildiz M, Erdem V, Seven N, Demirbuga S,
et al. Three‑year clinical performance of two indirect composite inlays
compared to direct composite restorations. Med Oral Patol Oral Cir
CONCLUSION Bucal 2013;18:e521‑8.
13. Cetin AR, Unlu N, Cobanoglu N. A five‑year clinical evaluation of direct
nanofilled and indirect composite resin restorations in posterior teeth.
With the available evidence, this review concludes that Oper Dent 2013;38:E1‑11.
14. Mendonça JS, Neto RG, Santiago SL, Lauris JR, Navarro MF,
three studies included in this review have high level of de Carvalho RM, et al. Direct resin composite restorations versus
evidence, seven studies have a high risk of bias and five indirect composite inlays: One‑year results. J Contemp Dent Pract
studies have moderate risk of bias. One study having a 2010;11:025‑32.
15. Cetin AR, Unlu N. One‑year clinical evaluation of direct nanofilled
low risk of bias, concluded that there was no significant and indirect composite restorations in posterior teeth. Dent Mater J
difference between direct and indirect technique. 2009;28:620‑6.
16. Bartlett D, Sundaram G. An up to 3‑year randomized clinical study
comparing indirect and direct resin composites used to restore worn
Out of five studies that have a moderate risk of bias, three posterior teeth. Int J Prosthodont 2006;19:613‑7.
studies reported that there was no significant difference 17. Pallesen U, Qvist V. Composite resin fillings and inlays. An 11‑year
evaluation. Clin Oral Investig 2003;7:71‑9.
between direct and indirect composite restorations 18. Manhart J, Neuerer P, Scheibenbogen‑Fuchsbrunner A, Hickel R.
and remaining studies concluded that indirect inlays Three‑year clinical evaluation of direct and indirect composite
restorations in posterior teeth. J Prosthet Dent 2000;84:289‑96.
demonstrated significantly better anatomic form of surface 19. Wassell RW, Walls AW, McCabe JF. Direct composite inlays
than direct composite restorations. Among the seven versus conventional composite restorations: 5‑year follow‑up.
8 Journal of Conservative Dentistry | Volume 21 | Issue 1 | January-February 2018
[Downloaded free from http://www.jcd.org.in on Thursday, February 22, 2018, IP: 61.16.135.114]
Azeem and Sureshbabu: Direct versus indirect composite restorations in posterior teeth - SR
J Dent 2000;28:375‑82. Hickel R, et al. One‑year clinical evaluation of composite fillings and
20. Scheibenbogen‑Fuchsbrunner A, Manhart J, Kremers L, Kunzelmann KH, inlays in posterior teeth. Clin Oral Investig 1997;1:65‑70.
Hickel R. Two‑year clinical evaluation of direct and indirect composite 22. Wassell RW, Walls AW, McCabe JF. Direct composite inlays versus
restorations in posterior teeth. J Prosthet Dent 1999;82:391‑7. conventional composite restorations: Three‑year clinical results. Br Dent
21. Scheibenbogen A, Manhart J, Kunzelmann KH, Kremers L, Benz C, J 1995;179:343‑9.
Journal of Conservative Dentistry | Volume 21 | Issue 1 | January-February 2018 9
Copyright of Journal of Conservative Dentistry is the property of Wolters Kluwer India Pvt
Ltd and its content may not be copied or emailed to multiple sites or posted to a listserv
without the copyright holder's express written permission. However, users may print,
download, or email articles for individual use.
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pigging ProcedureDocument11 pagesPigging ProcedureEndika Alfan100% (9)
- Ccie DC Full Scale Labs PDFDocument185 pagesCcie DC Full Scale Labs PDFnaveedrana100% (2)
- Workshop Manual: 3LD 450 3LD 510 3LD 450/S 3LD 510/S 4LD 640 4LD 705 4LD 820Document33 pagesWorkshop Manual: 3LD 450 3LD 510 3LD 450/S 3LD 510/S 4LD 640 4LD 705 4LD 820Ilie Viorel60% (5)
- Sir Syed Ahmed Khan and Two Nation TheoryDocument11 pagesSir Syed Ahmed Khan and Two Nation TheoryZeeshan Saeed100% (5)
- UF6 ManualDocument24 pagesUF6 ManualPhil Ruby Tigers0% (1)
- Vasuanand Bba ProjectDocument66 pagesVasuanand Bba ProjectMaster PrintersNo ratings yet
- Rapid Prototyping and ToolingDocument2 pagesRapid Prototyping and ToolingelangandhiNo ratings yet
- Boston Consultancy Group Matrix MM101Document8 pagesBoston Consultancy Group Matrix MM101Gift Simau100% (2)
- Srijana BahadurDocument13 pagesSrijana Bahadurkhadija khanNo ratings yet
- Drug-Induced Sleep Endoscopy (DISE)Document4 pagesDrug-Induced Sleep Endoscopy (DISE)Luis De jesus SolanoNo ratings yet
- VRTS - 10-13-20Document1 pageVRTS - 10-13-20Aina Saunar VargasNo ratings yet
- Fender Re-Issue 62 Jazzmaster Wiring DiagramDocument1 pageFender Re-Issue 62 Jazzmaster Wiring DiagrambenitoNo ratings yet
- Usability Test Report MemoDocument2 pagesUsability Test Report MemoTiffany PetersonNo ratings yet
- Jess's Heart Is Racing at 100 Miles Per Hour.Document3 pagesJess's Heart Is Racing at 100 Miles Per Hour.vexagon wallowNo ratings yet
- Chapter 3 - Instructional PlanningDocument30 pagesChapter 3 - Instructional PlanningMadelyne BenitezNo ratings yet
- Electronics by Gibilisco QandADocument22 pagesElectronics by Gibilisco QandAMary Rose AtendidoNo ratings yet
- Unidad 1 - Paco (Tema 3 - Paco Is Wearing A New Suit) PDFDocument24 pagesUnidad 1 - Paco (Tema 3 - Paco Is Wearing A New Suit) PDFpedropruebaNo ratings yet
- Recognition SpielDocument4 pagesRecognition SpielJoeyNo ratings yet
- Antenna Mini ProjectDocument65 pagesAntenna Mini ProjectHassan MehsenNo ratings yet
- Edavaka VillageDocument160 pagesEdavaka VillageGokul KrishnaNo ratings yet
- Imran Index 1Document11 pagesImran Index 1api-387022302No ratings yet
- Article Role of Zinc Post-Injury Wound Healing: Special inDocument3 pagesArticle Role of Zinc Post-Injury Wound Healing: Special inVinicio Rodriguez MirandaNo ratings yet
- Mathematics IDocument247 pagesMathematics IShreya PankajNo ratings yet
- Heat Transfer Fluid O&MDocument14 pagesHeat Transfer Fluid O&MOcto Adhi W PryhantoNo ratings yet
- Lesson: Identifying Author's Bias For or Against: Quarter 3 Wk-1Document4 pagesLesson: Identifying Author's Bias For or Against: Quarter 3 Wk-1Mary Cris Navarro LiboonNo ratings yet
- QMM Epgdm 1Document113 pagesQMM Epgdm 1manish guptaNo ratings yet
- Pms 500 - International Mechanics KitDocument0 pagesPms 500 - International Mechanics KitArsul RNo ratings yet
- The Adventist Perspective of Unity With CatholicismDocument12 pagesThe Adventist Perspective of Unity With Catholicismfortyniner85No ratings yet
- Cybersecurity in Operational Technology: Special ReportDocument15 pagesCybersecurity in Operational Technology: Special ReportAdrian ReyesNo ratings yet
- 02 - Thank You Maam Square Task CardsDocument8 pages02 - Thank You Maam Square Task CardsMaria Evelyn Won100% (1)