You might also like
- Hemodynamic Management Pocket Card PDFDocument8 pagesHemodynamic Management Pocket Card PDFjenn1722No ratings yet
- Pharmacotherapy 10thDocument131 pagesPharmacotherapy 10thMuhamed Arsalan100% (3)
- Lymphatic Drainage of Head & NeckDocument83 pagesLymphatic Drainage of Head & Neckshanima sherinNo ratings yet
- MX 13 Spec SheetDocument2 pagesMX 13 Spec SheetHarish KumarNo ratings yet
- Cardio NotesDocument2 pagesCardio NotesMagdaraog Gabrielle A.No ratings yet
- 04-CVS - Nader 6 2019+++++++Document14 pages04-CVS - Nader 6 2019+++++++Refan NajiNo ratings yet
- Materi DR. Dr. Ery Olivianto, Sp.A (K)Document39 pagesMateri DR. Dr. Ery Olivianto, Sp.A (K)utamiprakosoNo ratings yet
- 100 Anatomy Mcqs With AnswersDocument13 pages100 Anatomy Mcqs With Answersqudsia_niazi100% (2)
- The A To Z of The HeartDocument259 pagesThe A To Z of The HeartAspenPharma100% (2)
- מצגת קרדיולוגיה מעודכנת עם שאלות 1Document289 pagesמצגת קרדיולוגיה מעודכנת עם שאלות 1adnan shwNo ratings yet
- 4 FlangesDocument52 pages4 FlangesJumanah Al-alshaikhNo ratings yet
- 01 FridmanDocument94 pages01 FridmanErwanNo ratings yet
- Trends in Appendicitis and Perforated Appendicitis Prevalence in Children in The United States, 2001-2015Document4 pagesTrends in Appendicitis and Perforated Appendicitis Prevalence in Children in The United States, 2001-2015Kristia PutricinartyNo ratings yet
- SIIIIDocument1 pageSIIIIBam SantiagoNo ratings yet
- Estimated Calorie Needs Per Day TableDocument2 pagesEstimated Calorie Needs Per Day TableИндийскаяДевушкаNo ratings yet
- Label The Point at Which England Will Produce As E. Label The Point at Which Portugal Will Produce As PDocument1 pageLabel The Point at Which England Will Produce As E. Label The Point at Which Portugal Will Produce As PS.M. YAMINUR RAHMANNo ratings yet
- 155 - Flow Chart CV .8Document1 page155 - Flow Chart CV .8Mugywara luNo ratings yet
- Unicef Fao WFP Resilience Strategy 20120116Document17 pagesUnicef Fao WFP Resilience Strategy 20120116Tequan HolderNo ratings yet
- Cast Bronze 300Document140 pagesCast Bronze 300Adrian GaribNo ratings yet
- Split Casing Centrifugal Pumps: Meccaniche Idroelettriche Service ArzignanoDocument11 pagesSplit Casing Centrifugal Pumps: Meccaniche Idroelettriche Service ArzignanoAhmed ShawkiNo ratings yet
- Block 1 - Foundation Plan: Notes Drawing TitleDocument1 pageBlock 1 - Foundation Plan: Notes Drawing TitleKennedyNo ratings yet
- Allele 100bp DNA LadderDocument1 pageAllele 100bp DNA LadderAlleleBiotechNo ratings yet
- Price History: Tables and ChartsDocument16 pagesPrice History: Tables and ChartsAmir Mahmoud Mahdavi AbhariNo ratings yet
- Gold 18jan2023 YardeniDocument19 pagesGold 18jan2023 YardeniscribbugNo ratings yet
- Consequences of Ocean Acidification For FisheriesDocument32 pagesConsequences of Ocean Acidification For FisheriesDei Gioerel Garbosa BalindoaNo ratings yet
- Valvula ElectroneumaticaDocument4 pagesValvula ElectroneumaticaVictor Hugo Alvarez CortinezNo ratings yet
- 2018 41 Moesm1 EsmDocument11 pages2018 41 Moesm1 EsmChae SonNo ratings yet
- Schedule of WindowsDocument1 pageSchedule of Windowsfrancis sebastian lagamayoNo ratings yet
- Mid Power Laser Sources Ylr 100 Watt 2 KW in CWDocument2 pagesMid Power Laser Sources Ylr 100 Watt 2 KW in CWAbderrahmen HerichiNo ratings yet
- Propeller Can Be Sized Within or Above The Speed Range ShownDocument3 pagesPropeller Can Be Sized Within or Above The Speed Range ShownadelsoNo ratings yet
- PRC 251 Fireproofingforhydrocarbonfireexposuresv 1Document8 pagesPRC 251 Fireproofingforhydrocarbonfireexposuresv 1Abdul HafeezNo ratings yet
- D 1 D 2 D 3 D 4: Schedule of Doors and WindowsDocument1 pageD 1 D 2 D 3 D 4: Schedule of Doors and WindowsJoenyl Fernand CaingcoyNo ratings yet
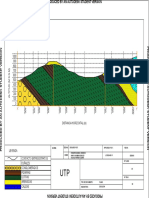
- Trabajo 6 Geologia CorteDocument1 pageTrabajo 6 Geologia Cortejtrinacokhotmail.comNo ratings yet
- Schedule of Doors & Windows: D1 D2 D4 D3 W1Document1 pageSchedule of Doors & Windows: D1 D2 D4 D3 W1Jay HernandezNo ratings yet
- Price History: Tables and ChartsDocument16 pagesPrice History: Tables and Chartslouis donyNo ratings yet
- Rates of Cov 19 by VaccinationDocument6 pagesRates of Cov 19 by VaccinationGilberto AlvesNo ratings yet
- Adults Respiratory Examination - P1 P9Document9 pagesAdults Respiratory Examination - P1 P9Tiago SilvaNo ratings yet
- Naturals Menu WomenDocument8 pagesNaturals Menu WomenMachilipatnam NaturalsNo ratings yet
- ATUM (Rhamnosa E.coli)Document4 pagesATUM (Rhamnosa E.coli)Ruth MichelleeNo ratings yet
- 40 - Southern Cross - Iso Pump - 125 X 100 - 250 - 1200 3000 RPMDocument1 page40 - Southern Cross - Iso Pump - 125 X 100 - 250 - 1200 3000 RPMJAZZ KING PROJECTNo ratings yet
- Voltage TransformersDocument26 pagesVoltage TransformersMostafa ShoaibNo ratings yet
- Fakultas Teknik: Denah Lantai 1 Kantor WalikotaDocument1 pageFakultas Teknik: Denah Lantai 1 Kantor WalikotaraNo ratings yet
- Parallel Pump Curves TA2538 X 4, 1760 RPM : L/Sec 200 300 400 500 600 700 800 900 1000 1100 1200Document1 pageParallel Pump Curves TA2538 X 4, 1760 RPM : L/Sec 200 300 400 500 600 700 800 900 1000 1100 1200Rubi AbionNo ratings yet
- Charvi Pandey Aayushi Srivastava Ravi Kumar Shagun Jhalani Nav Krishna Chaudhary Kainesh Patel Milan ShambharkarDocument59 pagesCharvi Pandey Aayushi Srivastava Ravi Kumar Shagun Jhalani Nav Krishna Chaudhary Kainesh Patel Milan ShambharkarNavedNo ratings yet
- IDP Movement Trend Tracking - Jun-Dec 16Document1 pageIDP Movement Trend Tracking - Jun-Dec 16YenThiLeNo ratings yet
- Writing 1 EmmaDocument1 pageWriting 1 Emmaroom8ncsNo ratings yet
- MTP CAD 1-Layout3Document1 pageMTP CAD 1-Layout3Laurence Emmanuel BenedictosNo ratings yet
- Description: Tags: 2004PaySchedDocument6 pagesDescription: Tags: 2004PaySchedanon-579857No ratings yet
- Description: Tags: p0003TableAFultimeDocument1 pageDescription: Tags: p0003TableAFultimeanon-994991No ratings yet
- Writing Term 3 EmmaDocument1 pageWriting Term 3 Emmaroom8ncsNo ratings yet
- Writing Term 3 JordanDocument1 pageWriting Term 3 Jordanroom8ncsNo ratings yet
- Appendix 2.: Estimated Calorie Needs Per Day, by Age, Sex, & Physical Activity LevelDocument2 pagesAppendix 2.: Estimated Calorie Needs Per Day, by Age, Sex, & Physical Activity LevelGloryJaneNo ratings yet
- International Summary July 2016 FIRST PAGE ONLYDocument1 pageInternational Summary July 2016 FIRST PAGE ONLYLe ThyNo ratings yet
- DF Transformer TR20Document2 pagesDF Transformer TR20Mostafa ShoaibNo ratings yet
- Estimated Calorie RequirementsDocument2 pagesEstimated Calorie Requirementsaurora mamaradloNo ratings yet
- Volume Galian Dan TimbunanDocument56 pagesVolume Galian Dan Timbunandinal031No ratings yet
- Writing Term 3 KyleDocument1 pageWriting Term 3 Kyleroom8ncsNo ratings yet
- DosageDocument1 pageDosagemustabshirah.nayerNo ratings yet
- Writing 1 KyleDocument1 pageWriting 1 Kyleroom8ncsNo ratings yet
- Floor Standing Enclosures Multicompact - MT: Standard Door Enclosures Series TCC - TSC - TFCDocument1 pageFloor Standing Enclosures Multicompact - MT: Standard Door Enclosures Series TCC - TSC - TFCAdel AdelNo ratings yet
- Writing 1 RowenDocument1 pageWriting 1 Rowenroom8ncsNo ratings yet
- BreakerDocument1 pageBreakerPrasad RaviproluNo ratings yet
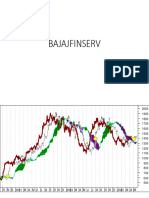
- BAJAJFINSERVDocument2 pagesBAJAJFINSERVStuart BroodNo ratings yet
- Steelbenchmarker 230508Document16 pagesSteelbenchmarker 230508NadaNo ratings yet
- Pac56 Mx13specsheet 2021 Final DigitalhiresDocument2 pagesPac56 Mx13specsheet 2021 Final Digitalhiresgaurao.pandeNo ratings yet
- Writing 1 KapilDocument1 pageWriting 1 Kapilroom8ncsNo ratings yet
- Medicare's Search For Effective Obesity Treatments: Diets Are Not The AnswerDocument14 pagesMedicare's Search For Effective Obesity Treatments: Diets Are Not The AnswerMantas LiekisNo ratings yet
- Low-Fat Dietary Pattern and Weight Change Over 7 Years: The Women's Health Initiative Dietary Modification TrialDocument11 pagesLow-Fat Dietary Pattern and Weight Change Over 7 Years: The Women's Health Initiative Dietary Modification TrialMantas LiekisNo ratings yet
- Knowledge Vs IgnoranceDocument2 pagesKnowledge Vs IgnoranceMantas LiekisNo ratings yet
- Early Feeding: Lifelong Health: Questions and Answers From BNF WebinarDocument3 pagesEarly Feeding: Lifelong Health: Questions and Answers From BNF WebinarMantas LiekisNo ratings yet
- Talk DR Garcia 2019Document32 pagesTalk DR Garcia 2019Mantas LiekisNo ratings yet
- Diet and Cancer: Professor Christine EdwardsDocument69 pagesDiet and Cancer: Professor Christine EdwardsMantas LiekisNo ratings yet
- Cardiac CT - Current Practice and Emerging ApplicationsDocument9 pagesCardiac CT - Current Practice and Emerging ApplicationsmonicaNo ratings yet
- Circulatory SystemDocument7 pagesCirculatory SystemWisdom DzombeNo ratings yet
- Anatomic Variants and Artefacts in Non Enhanced MRDocument8 pagesAnatomic Variants and Artefacts in Non Enhanced MRlouloupavelNo ratings yet
- Thorax Anatomy..Document21 pagesThorax Anatomy..Dungani AllanNo ratings yet
- PERCENTIL PA - MASCULINO - UpToDateDocument3 pagesPERCENTIL PA - MASCULINO - UpToDateQuisbert Rodriguez María Fernanda NicolNo ratings yet
- Practice Test: Biology: Body Fluids & Circulation For Live Session On 17-Nov-2018 On Neetprep Youtube ChannelDocument4 pagesPractice Test: Biology: Body Fluids & Circulation For Live Session On 17-Nov-2018 On Neetprep Youtube ChannelSamprita DuttaNo ratings yet
- Anatomy 2-Final-June 2023Document9 pagesAnatomy 2-Final-June 2023Douaa lkNo ratings yet
- VaricoceleDocument4 pagesVaricoceleRahajeng Ainiken PutririmasariNo ratings yet
- 1 - VSD (Part 2) - Hatem HosnyDocument28 pages1 - VSD (Part 2) - Hatem Hosnyrami ibrahiemNo ratings yet
- Materi VHD - DR - Achmad PutraDocument44 pagesMateri VHD - DR - Achmad PutraDila AswitaliaNo ratings yet
- Perspectives in Cardiovascular & Thoracic Surgery Volume III: Adult Cardiac Surgery (ACS)Document46 pagesPerspectives in Cardiovascular & Thoracic Surgery Volume III: Adult Cardiac Surgery (ACS)Mohammed AfzalNo ratings yet
- Acute Coronary Syndrome (G4)Document6 pagesAcute Coronary Syndrome (G4)Francis Josh DagohoyNo ratings yet
- Management of Pulmonary EdemaDocument42 pagesManagement of Pulmonary Edemaademato4real576No ratings yet
- ArrhythmiaDocument8 pagesArrhythmiaPrecious Grace CabahugNo ratings yet
- Transport in AnimalsDocument81 pagesTransport in AnimalsIbrahim NOORZADNo ratings yet
- Pathophysiology Tia VS CvaDocument6 pagesPathophysiology Tia VS CvaRobby Nur Zam ZamNo ratings yet
- The Cardiac Electrical System and How The HeartDocument26 pagesThe Cardiac Electrical System and How The HeartZoe Jisel LuzadasNo ratings yet
- Part1 - CIE IGCSE Biology 9 RN - SampleDocument2 pagesPart1 - CIE IGCSE Biology 9 RN - SampleJun ZheNo ratings yet
- Scalp Injuries: Neurosurgery Dr. El - MataryDocument5 pagesScalp Injuries: Neurosurgery Dr. El - Mataryflickers xxxNo ratings yet
- Syllabus ANP1105Document10 pagesSyllabus ANP1105Nusrat TazkiaNo ratings yet
- Cath Lab Optimal - Angiographic - Views - For - Invasive - Coronary - Angiography - A - Guide 2Document23 pagesCath Lab Optimal - Angiographic - Views - For - Invasive - Coronary - Angiography - A - Guide 2蘇柏霖No ratings yet
- Transportation in Plants and Animals Ncert and Extra QuestionsDocument6 pagesTransportation in Plants and Animals Ncert and Extra QuestionsNaitik MeenaNo ratings yet
- The Lymphatic SystemDocument27 pagesThe Lymphatic Systemوجد عمرNo ratings yet