Professional Documents
Culture Documents
111 Full
Uploaded by
Rizky Fadhilah87Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
111 Full
Uploaded by
Rizky Fadhilah87Copyright:
Available Formats
See discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/14923013
Medical personnel's knowledge of and ability to use inhaling devices. Metered-
dose inhalers, spacing chambers, and breath-actuated dry powder inhalers
Article in Chest · January 1994
DOI: 10.1378/chest.105.1.111 · Source: PubMed
CITATIONS READS
262 280
4 authors, including:
Nicola Hanania Rich Wittman
Baylor College of Medicine Stanford Medicine
473 PUBLICATIONS 15,285 CITATIONS 3 PUBLICATIONS 333 CITATIONS
SEE PROFILE SEE PROFILE
Kenneth R Chapman
University of Toronto
516 PUBLICATIONS 16,991 CITATIONS
SEE PROFILE
Some of the authors of this publication are also working on these related projects:
Chronic obstructive pulmonary disease patient reported outcome instruments View project
Scalable Health View project
All content following this page was uploaded by Kenneth R Chapman on 03 June 2014.
The user has requested enhancement of the downloaded file.
Medical personnel's knowledge of and ability to
use inhaling devices. Metered-dose inhalers,
spacing chambers, and breath-actuated dry
powder inhalers.
N A Hanania, R Wittman, S Kesten and K R Chapman
Chest 1994;105;111-116
The online version of this article, along with updated information and services
can be found online on the World Wide Web at:
http://chestjournal.chestpubs.org/content/105/1/111
Chest is the official journal of the American College of Chest Physicians. It has
been published monthly since 1935. Copyright1994by the American College of
Chest Physicians, 3300 Dundee Road, Northbrook, IL 60062. All rights
reserved. No part of this article or PDF may be reproduced or distributed
without the prior written permission of the copyright holder.
(http://chestjournal.chestpubs.org/site/misc/reprints.xhtml) ISSN:0012-3692
Downloaded from chestjournal.chestpubs.org by guest on July 13, 2011
© 1994 American College of Chest Physicians
Medical Personnel’s Knowledge of and
Ability to Use Inhaling Devices*
Metered-Dose Inhalers, Spacing Chambers, and
Breath-actuated Dry Powder Inhalers
Nicola A. Hanania, M.D.; Richard Wittman;
Steven Kesten, M.D., F.C.C.P.; and Kenneth R. Chapman, M.D., F.C.C.P.
Background: Current treatment strategies for asthma and versus 82 ± 13 percent and 69 ± 24 percent, respectively
chronic obstructive pulmonaiy disease (COPD) emphasize (p < 0.0001); for the Aerochamber, 98 ± 2 percent versus
the inhalation route, yet patients often misuse metered- 78 ± 2Opercentand57 ± 31 percent(p < O.0001);andforthe
dose inhalers (MDI). To address this problem, patient Tuchuhaler, 60 ± 30 percent versus 12 ± 23 percent and
education by medical personnel has been recommended 21 ± 30 percent (p < 0.0001). Knowledge of and practical
and a variety of alternate inhaler devices have been skills with the devices were roughly proportional to the
developed. length of time the device had been in clinical use, Tuthu-
Methods: We surveyed medical personnel to assess their baler demonstration scores being lower than either MDI
knowledge of and ability to use three widely used inhaler orAerochamberscores(p = O.O5andp = 0.09, respectively).
devices; MDI, MDI with a pacing chamber (Aerocham- More RTs (77 percent) had received formal instruction on
her, Trudell Medical, Canada), and a breath-actuated the use ofdevices at schoolthan either RNs (30 percent) or
multidose &y powder inhaler (Tinhuhaler, Astra Phar- MDs (43 percent) (p ‘c 0.05).
macy, Inc., Conada). Thirty respiratory therapists (RT), Conclusion: We conclude that (1) many medical personnel
30 registered nurses (RN), and 30 medical house staff responsible for monitoring and instructing patients in opti-
physicians (MD)were asked to demonstnite the use of each mal inhaler use lack rudimentary skills with these devices,
device using placebo inhalers and to answer 11 clinically (2) nurses and physicians seldom receive formal training in
relevant questions related to the use and maintenance of the use ofinhaling devices, and (3) newer inhaling devices
the tested devices. designed to obviate problems of technique are at present
Results: The Rrs pereent mean knowledge score (67±5 less likely to be used well by medical personnel soon after
percent) was significantly higher than those achieved by their introduction.
eitherthe RNs (39 ± 7 percent) orthe MDs (48 ± 7 percent) (Chest 1994; 105: 111-1 6)
(for all p ‘C 0.0001). Similarly, percent mean demonstration
MD = house staffphysiclan; MDI = metered-dose Inhaler;
scores for each device were significantly higher for RTs
RN = registered nurse; RT = respiratory therapist
than either RN or MD groups; for MDI, 97 ± 3 percent
C urrent treatment strategies for asthma and chronic only 10 to 15 percent of the aerosol actually reaches
obstructive pulmonary disease (COPD) empha- the lung.4’6 Clinically important problems arise when
size the role of self-administered inhalation therapy.’ patients fail to use the MDI properly often mistiming
The regular use of inhaled anti-inflammatory agents inhalation and canister actuation.7’8 Several studies
with inhaled B-agonists for rescue is now considered have shown that 24 to 89 percent of patients have poor
to be the cornerstone for the optimal long-term asthma technique when using the MDI.’2 To remedy this
therapy. Similarly in COPD, inhaled therapy appears problem, patient education by medical personnel has
to offer greater benefit with less risk of side effects been recommended,5”3”4 a variety of alternate easy-
than oral therapy. The use of hand-held inhalation to-use inhalation devices have been developed,’5’8
devices provides a rapid, cost-effective, and safe and several teaching tools including videotapes and
method of delivering drugs to the lung. Successful pamphlets have been introduced. However, few stud-
therapy is dependent on the proper deposition of the ies have assessed the ability of medical personnel to
drug in the lung, although some effects can arise from use MDI’ and available data are discouraging. No
drug either deposited in the oropharyrix and absorbed study has assessed the ability of medical personnel to
locally or swallowed and absorbed from the gastroin- use the newer inhalation devices. We, therefore, under-
testinal tract. Metered-dose inhalers (MDI) are the took the following study to survey three groups of
devices most commonly used for aerosolized drug medical personnel to assess their knowledge of
delivery. Even with the best inhalation technique, and ability to use three different commonly used inhaling
devices.
*From the Asthma Centre, The Toronto Hospital, University of METHODS
Toronto, Toronto, Canada. Subjects
Manuscript received February 8, 1993; revision accepted April 13.
Reprint requests: Dr. Chapman, 4-011 ECW, 399 Bathurst Street, The study was performed at The Toronto Hospital (a tertiary
Toronto, Ontario, Canada M5T2S8 care university-based hospital). Thirty respiratory therapists (RTs), 30
CHEST I 105 I 1 I JANUARY, 1994 111
Downloaded from chestjournal.chestpubs.org by guest on July 13, 2011
© 1994 American College of Chest Physicians
Table 1-Steps Used to A88e88 Demonstration Score
Step MDI* Aerochamber Turbuhaler
1 Remove cap Remove caps and connect Remove cover
2 Shake inhaler Hold inhaler and spacer together and Hold inhaler upright
shake
3 Hold inhaler upright Exhale to (FRC) or (RV) Turn bottom clockwise then
anticlockwise
4 Tilt head back or keep at level ‘lilt head back or keep at level Exhale away from inhaler to (FRC) or
(1W)
5 Exhale to functional residual capacity Insert mouthpiece between lips Insert mouthpiece between lips
(FRC) or residual volume (RV)
6 Insert or keep mouthpiece 2-4 cm Actuate canister once . Breathe in forcefully and deeply
away from mouth
7 Begin breathing then actuate canister Inhale slowly and deeply Do not exhale, remove inhaler from the
once mouth
8 Continue slow, deep inspiration Should hear a hissing sound and not Hold breath to comfort (5-10 s)
a whistle
9 Hold breath for 5-10 s Hold breath for 5-10 s (may repeat Exhale, wait 20-30 s before a second
steps 7-9) inhalation
10 Exhale, wait for 20-30 s before a Wait for 20-30 s Hold upright
second actuation
11 Shake again before a second Shake again before a second Rotate bottom again before a second
actuation actuation inhalation
*MDI =
metered-dose inhaler.
registered nurses (RNs) working on the medical and respiratory by means ofa written criteria for each device (Table 1). Prior to the
wards, and 30 medical house staff physicians (MDs) (internal study, the research assistants monitored patient performance si-
medicine residents and interns) were asked to participate. All multaneously on a trial basis until their demonstration scores were
medical personnel enrolled were involved in the daily care of in agreement ( ± 1/11). The interview comprised three sections. In
patients and prescribed, administered, or dispensed the inhaler the first section, background information was recorded, including
devices being assessed. Participants were contacted in the morning age, year of graduation, and the method of acquiring inhaler skills.
of the proposed interview and were kept blinded to the content of A knowledge score was derived by asking each participant to answer
the survey until the time of the interview. Each interview was 1 1 clinically relevant questions related to the use and maintenance
completed without interruption. An effort was made to ensure that of the devices tested (Table 2). In the third and last section,
the atmosphere during the interview would be relaxed; it was participants were evaluated for their ability to use three commonly
clearly stated to each participant that the survey was in no way a used devices; an MDI, an MDI with a spacing chamber (Aerocham-
job performance review and that all the results would remain ber), and a dry powder multidose inhaler (Turbuhaler). (This last
confidential. device is not currently available for drug delivery in the United
States but is used extensively elsewhere. It is a breath-actuated dry
Protocol powder inhaler in which all 200 doses of the drug are preloaded.
Medications are delivered without lactose or other adjuvants used
All participants were interviewed by one of two research assistants
commonly in other dry powder devices. A protective cap must be
who were trained to use placebo devices and to assess device usage
removed from the device before each use. Before forceful inhalation
Table 2-Questions (Jsedfor Knowledge Score Assessment from the mouthpiece, a dosage of drug is dropped from a reservoir
chamber into an inhalation chamber by the simple expedient of
Qu estion Question Content* rotating a knob at the bottom of the device. The device does not
require shaking before use. Because drug delivery is inhaled without
1 Determining when MDI is empty
propellant, coordination problems are obviated.) Those being tested
2 Determining when a Turbuhaler is empty
were not allowed to refer to package inserts or other printed
3 Slow inspiration recommended when using an
instructions. All participants were given placebo inhalers and were
MDI
asked to take two puffs using each device. A demonstration score
4 Turbuhaler cleaning procedure
was recorded according to the correct performance of 1 1 steps for
5 Aerochamber decreases aerosol deposition in the
mouth
Table 3-Ircent Mean (± SD) De,nonstration and
6 When using the Turbuhaler, one does not feel the
Knowledge Scores5
medication go down
7 Importance ofrinsing the mouth after using an
8
inhaled steroid
Order ofuse; a-stimulant and inhaled steroid
Knowledge
Score
‘- MDI
Demonstration
Turbuhaler
Score
Aerochamber
9 Waiting for at least 20 s before taking a second puff
from an MDI Fr 67±5 97±3 60±30 98±2
10 Breathholding for 10 s after inhaling the aerosol or RN 39±7 82±13 12±23 78±20
the dry powder MD 48±7 69±24 21±30 57±31
11 Aerochamber cleaning procedure
*MDI = metered-dose inhaler; RT respiratory therapist;
MDI = met ered-dose inhaler. RN = registered nurse; MD house staff physician.
112 Medical Personnel and Inhaling Devices (Hanania eta!)
Downloaded from chestjournal.chestpubs.org by guest on July 13, 2011
© 1994 American College of Chest Physicians
0
lii
I
U)
-J
#{149}RT
a,
0
C-, URN
C.)
4
i MD
.- H
ONE SIX SEVEN EIGHT NINE TEN ELEVEN
STEP
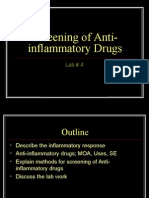
Ficuiu: 1. Proportion of medical personnel correctl performing individual steps in the self-
administration of the MDI.
each device (Table 2). The order ofpresentation ofthe devices aS Differences among groups in knowledge score were assessed b
randomized prior to the interview. The participant s’as given a one-way ANOVA. \Vliere significant differences existed, specific
grade of 0 if he or she skipped a step, perfoniwd a step inadequately. pair.se (o)pfl5()5 vere iiiade vitli the Student’s t test (unpaired.
answered a question incorrectly. or skipped a question. Respondents two-tailed). Differences were considered statistically significant at
were given a grade of 1 for each step performed correctly and for p < 0.05.
each question answered correctly.
Data Analysis RESULTS
Differences in demonstration scores were assessed h two-way Percent mean scores ± SD for each group and each
analysis of variance (ANOVA) using device and group categories. device are listed in Table 3.
100 -
90 -
80-
70
0
w
I 60
(I)
-J
a. #{149}RT
50
0
C-, URN
C.) 40
4
MD
30
20
10
0
ONE TWO ThREE FOUR FIVE SIX SEVEN EIGHT NINE TEN ELEVEN
STEP
FIGURE 2. Proportion of medical personnel correctly performing individual steps in the self-administration
of the Aerochamber.
CHEST I 105 I 1 I JANUARY, 1994 113
Downloaded from chestjournal.chestpubs.org by guest on July 13, 2011
© 1994 American College of Chest Physicians
90’
80
70
a 60
URT
URN
i
LIMD
4304
C.,
a,
840 50
20 I I L--
______ [U __________
Ii iii __________________ . I I ____
0i
10-41
ONE TWO THREE FOUR FIVE SIX SEVEN EIGHT NINE TEN ELEVEN
STEP
FIGURE 3. Proportion of medical personnel correctly performing individual steps in the self-administra-
tion of the Turbuhaler.
Demonstration Scores the Turbuhaler (Fig 3). This was chiefly because of
The percent mean demonstration score for RTs the total unfamiliarity with the device by most of the
(85 ± 21 percent) for all devices tested was significantly medical personnel.
higher than that achieved by either RNs (57 ± 39 Knowledge Scores
percent) or MDs (49 ± 25 percent) (for all p < 0.0001). The RTs’ percent knowledge score (67 percent) was
Mean demonstration scores for each of the three
signficantly higher than either the RNs’ (39 percent)
tested devices were significantly higher for RTs than
or the MDs’ (48 percent) scores (for all p < 0.0001).
either RN or MD groups (for all p < 0.0001). Mean Knowledge scores of the RNs and MDs were not
demonstration scores for RNs and MDs for all devices
statistically different (p = 0.07). Most frequently incor-
combined were not statistically different (p = 0.12). rect answers were related to the use and maintenance
However demonstration scores for the MDI and the of the Turbuhaler and the Aerochamber (questions
Aerochamber were statistically higher for RNs than 2,4,6, and 11) and to the knowledge of breathholding
for MDs (p = 0.01 and 0.003, respectively). The prac- after inhalation of aerosol from the MDI (question 10).
tical skills for these devices were roughly proportional Significantly more RTs (70 percent) had received
to the length of time the device had been in clinical formal instruction on using the devices at school than
use. For all medical personnel, Turbuhaler demon-
either RNs (30 percent) or MDs (43 percent) (p < 0.05).
stration scores (30.9 percent) tended to be lower than
The most common sources for acquiring knowledge
either MDI (82.7 percent) or Aerochamber (77.6
about the techniques were from observation and/or
percent) scores (p = 0.05 and p = 0.09, respectively).
from reading the pamphlets supplied by the pharma-
When using the MDI, 100 percent of the RTs, 83 ceutical company. The knowledge and practical skills
percent of the RNs, and 53 percent of MDs could
for the devices tested were roughly proportional to
perform 8 of 1 1 steps correctly, the most frequent
the length of time the device had been in clinical use.
problems being the failure to coordinate actuation
with inhalation and to breathhold after inhalation DISCUSSION
(steps 7 and 9) (Figure 1). With the use of the During the last few years, emphasis has been made
Aerochamber, 100 percent of the RTs, 87 percent of on the important role played by medical professionals
the RNs, and 43 percent of the MDs could perform in repeatedly instructing and monitoring patients for
8 of 1 1 steps correctly. Breathholding after inspira- the optimal use of inhaled medication delivery de-
tion and inspiration after actuation (steps 8 and 9) vices.’2#{176}However, our data show that many of these
were the most common problems (Fig 2). Forty percent medical personnel lack rudimentary skills with these
of RTs, 13 percent of MDs, but none of the RNs could devices and many lack elementary theoretic knowl-
perform 8 of 1 1 steps correctly when asked to use edge about their use. Of the medical and paramedical
114 Medical Personnel and Inhaling Devices (Hanania et a!)
Downloaded from chestjournal.chestpubs.org by guest on July 13, 2011
© 1994 American College of Chest Physicians
groups tested, house staff and nurses seem least likely Unlike previous studies, we have addressed the
to use inhaling devices correctly and this may reflect required technique for taking multiple puffs from an
their lack of formal training in professional schools or inhaler. Many medications are prescribed in dosages
postgraduate training programs. Our data a1o show of more than a single puff and this increases the
that newer inhaling devices may be less optimally likelihood of making an error. For example, failure to
used than devices that have been in common usage wait an appropriate interval between actuations with
for several years. an MDI may result in a little or no medication being
Numerous studies have documented poor MDI delivered with the second actuation. In the case of the
technique by patients both young and old.’#{176}’3The Turbuhaler, patients may actuate the dry powder
results of our study would offer at least one explanation device twice before inhalation, a technique that wastes
for poor MDI usage by patients. The frequent inability a dose of drug as the dry powder reservoir rotates out
of physicians and some nonphysician medical staff to of the inhalation chamber. Such errors, we suspect,
use inhaling devices would result in poor instruction are commonly overlooked in clinical practice and have
ofpatients with consequent poor patient technique. not generally been the subject of published MDI
At a time when patient education is being emphasized usage studies.
in self-management schemes for asthma, this lack of Our findings with respect to Turbuhaler usage were
basic knowledge by medical staff is regrettable and somewhat surprising. The device, developed for the
must be addressed. Our study is not the first study to breath-actuated delivery of small quantities of dry
suggest that caregivers may use inhaling devices powder medication, is usually regarded as easy to use
inadequately. Kelling and colleagues’9 reported that and is relatively free from coordination problems
physicians were generally unable to use MDIs prop-
associated with other inhalers. Numerous studies have
erly despite their frequent prescription of such devices
demonstrated its clinical efficacy in various patient
to patients. Our study confirms and extends these
populations.27 However, such studies have been done
findings, showing that other medical personnel groups
under carefully controlled conditions suitable for a
may share this lack of knowledge and that the lack of
research trial for registration purposes; that is, such
know-ledge may extend to a wider variety of inhaling
studies reflect optimal patient instruction under ideal
devices.
noncinical circumstances. In actual clinical usage, this
Our findingsare compatible with those of two recent
relatively simple-to-use device appears to be misused
studies reporting that respiratory therapists were more
frequently by health care professionals. It is not clear
likely to use MDIs correctly than MDs or nurses.2122
how significant such mishandling is in the clinical
We suspect that this is attributable to the specialized
setting. The effectiveness of some bronchodilators may
nature of the Rrs task and to the higher likelihood of
be relatively insensitive to even grossly inadequate
formal education on inhaler devices received by this
technique given their redistribution by the endobron-
group. This would suggest a significant role for non-
chial circulation. However, the delivery of topical
physician medical personnel in education programs.
corticosteroids and other anti-inflammatory agents
Given the time required for asthma and COPD
may be more technique sensitive. We suspect that the
education programs, the use of nonphysician health
potential for has not been
misuse widely appreciated
care professionals is likely to be more cost-effective
and, in the case of inhaler usage, more likely to be and little attention has been given to the use of such
novel inhaling devices in postgraduate continuing
effective. Other nonphysician assistants could include
medical education courses. Indeed, the major respon-
clinical pharmacists, physician assistants, laboratory
technologists, and others. Thus, physicians should sibility for educating medical staff about such newly
carefully train their assistants to teach patients via introduced devices seem to fall on the companies
discussion, demonstration, and repeated observation responsible for their manufacture. The finding of poor
of their inhaler technique. The use of nonphysician Turbuhaler usage by medical personnel would explain
educators is more feasible in the clinic or hospital our clinical impressions that many patients have diffi-
setting and may be less practical in solo primary culty using these devices when first referred for
practice. Up to a third of patients in primary practice specialist assessment (Chapman, Epstein, Kesten,
are treated for respiratory problems but only few of unpublished observations, 1993). Indeed, we have seen
those are likely to be referred for a specialized many examples of Turbuhaler dispensed by retail
assessment and education. Hence, primary care phys- pharmacies bearing the label “shake well,” an obvious
icians must become personally familiar with appro- misuse of the device that would greatly impair its
pnate inhaler usage. Although our study did not survey efficacy. The observations of our study should prompt
the adequacy of inhaler usage by primary care physi- the implementation of a postmarketing surveillance
cians, we suspect that it might be even worse than program for this and all new inhaler devices.
among recently graduated MDs working in a teaching In summary, we have extended the observations of
hospital. Further study is clearly warranted. others who have found that medical personnel often
CHEST I 105 I 1 I JANUARY, 1994 115
Downloaded from chestjournal.chestpubs.org by guest on July 13, 2011
© 1994 American College of Chest Physicians
misuse MDIs. We found that this is true for other 13 SelfTH, Rumback MJ, Kelso TM. Correct use of metered-dose
types of inhaler devices, particularly newer ones with inhalers and spacer devices. Postgrad Med 1992; 92:95-106
14 Newman SP, Clarke SW. The proper use of metered-dose
which physicians and nonphysician health profession-
inhalers. Chest 1984; 86:342-43
als have little time to become familiar. Appropriate 15 Crompton GK. New inhalation devices. Eur Respir J 1988;
programs of postmarketing survefflance may help to 1:679-80
identify these problem areas with newer devices and 16 Jones K. New delivery systems for asthma drugs. Practitioner
1989; 233:265-67
would suggest appropriate educational responses.
17 Konig P. Spacer devices used with metered-dose inhalers,
breakthrough or gimmick? Chest 1985; 88:276-84
REFERENCES
18 Wetterlin KIL. Design and function ofTurbuhaler. In: Newman
1 National Asthma Education Program. Guidelines for the diag- SP, Mor#{233}n
F, Crompton GK, eds. New concept of inhalation
nosis and management ofasthma. Bethesda, Md: Dept of Health therapy. Medicom, 1987; 85-9
and Human Services, August 1991, DHHS publication 91-3042 19 Kelling JS, Strohl KP, Smith RL, Altose MD. Physician knowl-
2 Chapman KR, Bowie DM, Goldstein RS, et al. Canadian edge in the use of canister nebulizers. Chest 1983; 83:612-14
Thoracic Society Workshop Group: guidelines for the assessment 20 Self TH, Brooks JB, Lieberman P. Ryan MR. The value of
and management of chronic obstructive pulmonary disease. Can demonstration and role ofthe pharmacist in teaching the correct
Med Assoc J 1992; 147:420-28 use of pressurized bronchodilators. Can Med Assoc J 1983;
3 Tinkelman DG, Berkowitz RB, Cole WQ. Aerosols in the 128:129-31
treatment of asthma. J Asthma 1991; 28:243-49 21 Guidry GG, Brown WD, Stogner SW, George RB. Incorrect
4 Newman SP. Aerosol deposition considerations in inhalation use of metered dose inhalers by medical personnel. Chest
therapy. Chest 1985; 88:152S-160S 1992; 101:31-3
5 Di Benedetto C, Clarke SW. Inhalation therapy in asthma. JR 22 Interiano B, Guntupalli KK. Metered dose inhalers: do health
Society Med 1992; 339:814 care providers know what to teach? Arch Intern Med 1993;
6 Human B. Aerosol deposition and delivery of therapeutic 153:81-5
aerosols. J Asthma 1991; 28:239-42 23 SeIfTH, Kelso
TM, Arheart KL, et al. Nurses’ performance of
7 Lindgren S, Bake B, Larsson S. Clinical consequences of inhalation technique with metered dose inhaler plus spacer
inadequate inhalation technique in asthma therapy. Eur J Respir device. Ann Pharmacother 1993; 27:185-87
Dis 1987; 70:93-8 24 Hansen OR, Pedersen S. Optimal inhalation technique for
8 Saunders KB. Misuse of inhaled bronchodilator agents. BMJ terbutaline Turbuhaler. Eur Respir J 1989; 2:637-39
1965; 1:1037-38 25 Alto E, Havu M, et al. Comparison of turbutaline turbuhaler
9 Allen SC, Prior A. What determines whether an elderly patient and albuterol chlorofluorocarbon (CFC) inhaler in middle
can use a metered dose inhaler correctly? BrJ Dis Chest 1986; aged and elderly patients with obstructive lung disease. Ann
8:45-9 Allergy 1992; 69:33-6
10 Epstein SW, Manning CPR, Ashley MJ, Corey PN. Survey of 26 Bce J, Stiksa C, Svensson K, Asbrink E. New method of
the clinical use ofpressurized aerosol inhalers. Can Med Assoc evaluating patient preference for different inhalation devices.
I 1979; 120:813-16 Ann Allergy 1992; 68:285-60
11 Shim C, Williams MH Jr. The adequacy ofinhalation of aerosol 27 Hultquist C, Ahlstr#{246}m H, et al. A double blind comparison
from canister nebulizers. Am J Med 1980; 69:891-94 between a new multi-dose powder inhaler (Turbuhaler) and
12 Crompton GK. Problems patients have using pressurized aerosol metered dose inhaler in children with asthma. Allergy 1989;
inhalers. Eur J Respir Dis 1982; 63(suppl 119):101-04 44:467-70
116 Medical Personnel and Inhaling Devices (Hanania eta!)
Downloaded from chestjournal.chestpubs.org by guest on July 13, 2011
© 1994 American College of Chest Physicians
Medical personnel's knowledge of and ability to use inhaling devices.
Metered-dose inhalers, spacing chambers, and breath-actuated dry powder
inhalers.
N A Hanania, R Wittman, S Kesten and K R Chapman
Chest 1994;105; 111-116
This information is current as of July 13, 2011
Updated Information & Services
Updated Information and services can be found at:
http://chestjournal.chestpubs.org/content/105/1/111
Cited Bys
This article has been cited by 8 HighWire-hosted articles:
http://chestjournal.chestpubs.org/content/105/1/111#related-urls
Permissions & Licensing
Information about reproducing this article in parts (figures, tables) or in its entirety can be found
online at:
http://www.chestpubs.org/site/misc/reprints.xhtml
Reprints
Information about ordering reprints can be found online:
http://www.chestpubs.org/site/misc/reprints.xhtml
Citation Alerts
Receive free e-mail alerts when new articles cite this article. To sign up, select the "Services" link to
the right of the online article.
Images in PowerPoint format
Figures that appear in CHEST articles can be downloaded for teaching purposes in PowerPoint
slide format. See any online figure for directions.
Downloaded from chestjournal.chestpubs.org by guest on July 13, 2011
© 1994 American College of Chest Physicians
View publication stats
You might also like
- EMRA Antibiotic Guide EMRADocument2 pagesEMRA Antibiotic Guide EMRAPaoNu0% (3)
- Weaning An Adult Patient From Invasive Mechanical VentilationDocument22 pagesWeaning An Adult Patient From Invasive Mechanical VentilationYuanda ArztNo ratings yet
- 7 - The Biliary TractDocument48 pages7 - The Biliary TractKim RamosNo ratings yet
- Investigations in Psychiatry Guide Medical DiagnosesDocument59 pagesInvestigations in Psychiatry Guide Medical Diagnoseskiran mahal100% (1)
- Emergency Medicine in MBBSDocument85 pagesEmergency Medicine in MBBSPATHMAPRIYA GANESANNo ratings yet
- Anti Anxiety DrugsDocument15 pagesAnti Anxiety DrugsMr. Psycho SamNo ratings yet
- Case Study-Ectopic PNDocument55 pagesCase Study-Ectopic PNArbie Jacinto100% (2)
- Mark Fredderick R. Abejo RN, MAN: Fundamentals of Nursing BulletsDocument4 pagesMark Fredderick R. Abejo RN, MAN: Fundamentals of Nursing BulletsDan Hernandez100% (1)
- Doctor List SL - No. Doctorcode Doctorname Qualification Grade CategoryDocument174 pagesDoctor List SL - No. Doctorcode Doctorname Qualification Grade CategoryumeshNo ratings yet
- Predictors of Correct Technique in Patients UsingDocument11 pagesPredictors of Correct Technique in Patients UsingPetra ŠalamúnováNo ratings yet
- 2 DiaphragmaticExcursionDocument5 pages2 DiaphragmaticExcursionTiago XavierNo ratings yet
- Respiratory Medicine: Short CommunicationDocument3 pagesRespiratory Medicine: Short CommunicationFernando SarmientoNo ratings yet
- Palen - Et - Al-2016-Npj - Primary - Care - Respiratory - MedicineDocument8 pagesPalen - Et - Al-2016-Npj - Primary - Care - Respiratory - Medicinetechang1No ratings yet
- Correct Inhalation Technique Is Critical in Achieving GoodDocument2 pagesCorrect Inhalation Technique Is Critical in Achieving GoodSelvy YusmaNo ratings yet
- Kontrak Belajar Gadar Igd BaruDocument14 pagesKontrak Belajar Gadar Igd BaruAstridNo ratings yet
- Amikinhal TrialDocument11 pagesAmikinhal TrialBreno Bertozo SilvaNo ratings yet
- Maximizing Success With Rapid Sequence IntubationsDocument11 pagesMaximizing Success With Rapid Sequence IntubationsRaymond RosarioNo ratings yet
- Protocolos Weaining 2011Document14 pagesProtocolos Weaining 2011perla islasNo ratings yet
- Tate Avila DayDocument1 pageTate Avila DayHemantNo ratings yet
- Physicians-knowledge-Plaza-J Aerosol Med Pulm Drug Deliver-2012 25 16-22-1Document8 pagesPhysicians-knowledge-Plaza-J Aerosol Med Pulm Drug Deliver-2012 25 16-22-1Dejan ŽujovićNo ratings yet
- Article: ResearchDocument17 pagesArticle: Researchryan yovanNo ratings yet
- Multicéntrico Lellouche Et AllDocument7 pagesMulticéntrico Lellouche Et AllterapiafisicapilaresNo ratings yet
- 2 DiaphragmaticExcursionDocument4 pages2 DiaphragmaticExcursionAnandhu GNo ratings yet
- The Fatigued AnesthesiologistDocument2 pagesThe Fatigued AnesthesiologistaksinuNo ratings yet
- 3083 12086 2 PB 1Document10 pages3083 12086 2 PB 1adultnursingspecialtyNo ratings yet
- MedicinalDocument12 pagesMedicinalchrist.sony95No ratings yet
- ICU Management of COVID Patients: PreventionDocument13 pagesICU Management of COVID Patients: PreventionYuri SadewoNo ratings yet
- Lung Ultrasound-The Emerging Role of Respiratory TherapistsDocument13 pagesLung Ultrasound-The Emerging Role of Respiratory TherapistsArturo Loyola MaturanaNo ratings yet
- IJCRR Comparison of Acapella and RC Cornet For Airway Clearance in BronchiectasisDocument12 pagesIJCRR Comparison of Acapella and RC Cornet For Airway Clearance in Bronchiectasisvanita pathareNo ratings yet
- Knowledge Skill On Endotracheal Suctioning 2016Document7 pagesKnowledge Skill On Endotracheal Suctioning 2016Elisya KharuniawatiNo ratings yet
- Jurnal Open Closed Suction GelartiDocument9 pagesJurnal Open Closed Suction GelartiAyahe Bima MubarakaNo ratings yet
- NIRS in CovidDocument15 pagesNIRS in CovidljiljanarvicNo ratings yet
- 12Hiệu quả mở kq sớm pt gộp 2015Document10 pages12Hiệu quả mở kq sớm pt gộp 2015Cường Nguyễn HùngNo ratings yet
- Anae 14443Document7 pagesAnae 14443dr_syakbanNo ratings yet
- Inhaler Technique Education and Asthma Control AmoDocument10 pagesInhaler Technique Education and Asthma Control AmoAdi MuliadiNo ratings yet
- I - Study - Percentage of Assistance in PAV+ - Carteaux Et AlDocument9 pagesI - Study - Percentage of Assistance in PAV+ - Carteaux Et AlJuan Genaro Martinez PeñaNo ratings yet
- Tracheostomy 3Document7 pagesTracheostomy 3rizwanNo ratings yet
- Recruitment Manoeuvres in Anaesthesia - 2018Document10 pagesRecruitment Manoeuvres in Anaesthesia - 2018Angy KarakostaNo ratings yet
- Copd 14 1209Document9 pagesCopd 14 1209rizqina ajraNo ratings yet
- Airway Pressure Release VentilatiDocument9 pagesAirway Pressure Release VentilatiDavid ParraNo ratings yet
- Ferrer 2003Document7 pagesFerrer 2003Fermin LombardiaNo ratings yet
- Diaphragm Ultrasound As A New Method To Predict Extubation Outcome in Mechanically VentilaDocument7 pagesDiaphragm Ultrasound As A New Method To Predict Extubation Outcome in Mechanically VentilaSilvanaNo ratings yet
- Patient-Initiated Device Removal in Intensive Care Units - A National Prevalence StudyDocument7 pagesPatient-Initiated Device Removal in Intensive Care Units - A National Prevalence StudyJim LinNo ratings yet
- Diaphragm Function and Weaning From Mechanical VentilationDocument7 pagesDiaphragm Function and Weaning From Mechanical VentilationEzequiel SosaNo ratings yet
- Anesthesia For Advanced Bronchoscopic Procedures: State-of-the-Art ReviewDocument13 pagesAnesthesia For Advanced Bronchoscopic Procedures: State-of-the-Art ReviewRichard PhoNo ratings yet
- Biomedicine & Pharmacotherapy: Akshay Chandel, Amit K. Goyal, Goutam Ghosh, Goutam Rath TDocument11 pagesBiomedicine & Pharmacotherapy: Akshay Chandel, Amit K. Goyal, Goutam Ghosh, Goutam Rath Tm jaaaNo ratings yet
- JeradDocument10 pagesJeradzaimmuhtarNo ratings yet
- Poi 140032Document8 pagesPoi 140032د. محمد فريد الغنامNo ratings yet
- Nej Mo A 2310307Document11 pagesNej Mo A 2310307Víctor C. ValverdeNo ratings yet
- Intubazionedifficile TrueviewDocument7 pagesIntubazionedifficile Trueviewlina ukagoNo ratings yet
- Predictionof Difficult AirwayDocument6 pagesPredictionof Difficult AirwayjemyNo ratings yet
- Copd Misuse of Inhaler Devices in Clinical PracticeDocument9 pagesCopd Misuse of Inhaler Devices in Clinical PracticeAshif AnsariNo ratings yet
- Arroyo Novoa 2008Document8 pagesArroyo Novoa 2008EviNo ratings yet
- Capstone IVDocument10 pagesCapstone IVapi-631736561No ratings yet
- Ropvacaina VS Lidocaina Premdicacion IotDocument6 pagesRopvacaina VS Lidocaina Premdicacion IotFaith Lu PenalozaNo ratings yet
- 2013CarteauxCCM PAVDocument9 pages2013CarteauxCCM PAVFernando Dinamarca SotoNo ratings yet
- Use of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaDocument10 pagesUse of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaLingga AniNo ratings yet
- ENDODocument14 pagesENDOmichakishaNo ratings yet
- Jurding Sukma KyutDocument18 pagesJurding Sukma Kyutmaudi fitriantiNo ratings yet
- Development, Implementation and Impact of Simple Patient Safety Interventions in A University Teaching HospitalDocument6 pagesDevelopment, Implementation and Impact of Simple Patient Safety Interventions in A University Teaching HospitalMariale OrdóñezNo ratings yet
- Review: Stefano Nava, Nicholas HillDocument10 pagesReview: Stefano Nava, Nicholas HillLuis CortezNo ratings yet
- Anesthetics and Anesthesiology: ClinmedDocument6 pagesAnesthetics and Anesthesiology: ClinmednadaNo ratings yet
- Airway Pressure Release Ventilation A Review of The Evidence, Theoretical Benefits, and Alternative Titration StrategiesDocument9 pagesAirway Pressure Release Ventilation A Review of The Evidence, Theoretical Benefits, and Alternative Titration StrategiesJose Morato E FlavianeNo ratings yet
- Vibrating Mesh Nebulisers - Can Greater Drug DelivDocument11 pagesVibrating Mesh Nebulisers - Can Greater Drug DelivShabilah Novia SNo ratings yet
- Pham - Esophageal ManometryDocument21 pagesPham - Esophageal ManometryAbraham HaneineNo ratings yet
- Annals of Pharmacotherapy 2014 StollingsDocument15 pagesAnnals of Pharmacotherapy 2014 StollingsapheatNo ratings yet
- Pharmacology: Rapid Sequence Intubation Medication TherapiesDocument10 pagesPharmacology: Rapid Sequence Intubation Medication TherapiesIvan TapiaNo ratings yet
- Infectious Diseases in the Intensive Care UnitFrom EverandInfectious Diseases in the Intensive Care UnitManish SonejaNo ratings yet
- Indian J Derma To L Cross SectionalDocument5 pagesIndian J Derma To L Cross SectionalSisca Dwi AgustinaNo ratings yet
- Knowledge and Practice Asthmatic Patients Regard Using Meter Dose InhalerDocument9 pagesKnowledge and Practice Asthmatic Patients Regard Using Meter Dose InhalerRizky Fadhilah87No ratings yet
- COPD 157403 Knowledge and Pharmaceutical Care Practice of Inhaled Therap - 030918Document10 pagesCOPD 157403 Knowledge and Pharmaceutical Care Practice of Inhaled Therap - 030918Rizky Fadhilah87No ratings yet
- MDI Use Knowledge Among Healthcare WorkersDocument5 pagesMDI Use Knowledge Among Healthcare WorkersRizky Fadhilah87No ratings yet
- Ro-Ils PaperDocument4 pagesRo-Ils Paperapi-502011468No ratings yet
- Pas Poster FinalDocument1 pagePas Poster Finalapi-256316098No ratings yet
- Imperial CollegeDocument31 pagesImperial CollegeElPaisUyNo ratings yet
- Aviva PCP Panel of SpecialistDocument13 pagesAviva PCP Panel of SpecialistSreeja ReddyNo ratings yet
- Iota AdnexDocument10 pagesIota Adnexlinh hoàngNo ratings yet
- Screening of Anti-Inflammatory DrugsDocument11 pagesScreening of Anti-Inflammatory DrugsHaleema SultanNo ratings yet
- k9 Tecc Casualty Card FinalDocument2 pagesk9 Tecc Casualty Card Finalariel4dariel4laruta100% (1)
- Perio-Prog Class 2012Document80 pagesPerio-Prog Class 2012moorenNo ratings yet
- Radiological Diagnostics of Respiratory SystemDocument70 pagesRadiological Diagnostics of Respiratory SystemVAISHALI CHOUDHARYNo ratings yet
- Immunonutrition and Critical Illness An UpdateDocument8 pagesImmunonutrition and Critical Illness An Updateklinik kf 275No ratings yet
- Home VisitingDocument14 pagesHome Visitingsehar1606No ratings yet
- Otiflox New Ear DropsDocument9 pagesOtiflox New Ear DropsShreyas ModiNo ratings yet
- Dental Claim Form SubmissionDocument2 pagesDental Claim Form Submissionnicholas beehnerNo ratings yet
- Nasal Tip Numbness After RhinoplastyDocument4 pagesNasal Tip Numbness After RhinoplastySinan Kadir AltunalNo ratings yet
- FORMAT FOR UNIT PLAN-converted-1Document2 pagesFORMAT FOR UNIT PLAN-converted-1Delphy VargheseNo ratings yet
- PDF Breathing Exercise Effective Cough CompressDocument52 pagesPDF Breathing Exercise Effective Cough CompressThanksNo ratings yet
- Suzanne Bennett Resume 2010Document3 pagesSuzanne Bennett Resume 2010Kimberly DavisNo ratings yet
- Medical Training Initiative Guide: July 2017Document22 pagesMedical Training Initiative Guide: July 2017Sanjeev SrivastavNo ratings yet
- World Health Organization Dimensions of Adherence.9Document7 pagesWorld Health Organization Dimensions of Adherence.9Lucky Radja PonoNo ratings yet
- Pharmacology: Dr. Rakesh A Malpure Dr. Chandresh B DumatarDocument3 pagesPharmacology: Dr. Rakesh A Malpure Dr. Chandresh B DumatarChandresh DumatarNo ratings yet
- Risk Factors, Diagnosis and Non-Surgical Treatment For Meniscal Tears Evidence and Recommendations A Statement Paper Commissioned by The Danish Society of Sports Physical TherapyDocument9 pagesRisk Factors, Diagnosis and Non-Surgical Treatment For Meniscal Tears Evidence and Recommendations A Statement Paper Commissioned by The Danish Society of Sports Physical TherapyItai IzhakNo ratings yet
- Laporan Lb1 Puskesmas Berdasarkan Icd-10: Kelompok Usia B L B L B NO Urut PEN Yaki TDocument36 pagesLaporan Lb1 Puskesmas Berdasarkan Icd-10: Kelompok Usia B L B L B NO Urut PEN Yaki TTogi Rut Marlita MarbunNo ratings yet