You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
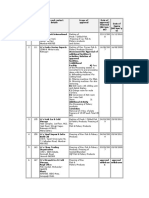
- COSHH Assessment TemplateDocument2 pagesCOSHH Assessment TemplaterichardNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- S1-2018-362227-bibliographyDocument5 pagesS1-2018-362227-bibliographyRizky Fadhilah87No ratings yet
- 111 FullDocument9 pages111 FullRizky Fadhilah87No ratings yet
- Knowledge and Practice Asthmatic Patients Regard Using Meter Dose InhalerDocument9 pagesKnowledge and Practice Asthmatic Patients Regard Using Meter Dose InhalerRizky Fadhilah87No ratings yet
- COPD 157403 Knowledge and Pharmaceutical Care Practice of Inhaled Therap - 030918Document10 pagesCOPD 157403 Knowledge and Pharmaceutical Care Practice of Inhaled Therap - 030918Rizky Fadhilah87No ratings yet
- Nursing ExamDocument9 pagesNursing ExamEmma IntiaNo ratings yet
- Principles of CGMP in Pharmaceutical IndustriesDocument6 pagesPrinciples of CGMP in Pharmaceutical IndustriesSamer SowidanNo ratings yet
- LEADERSHIP PAPER SELF-REFLECTION AND GROUP PLAN - Docx FINALDocument7 pagesLEADERSHIP PAPER SELF-REFLECTION AND GROUP PLAN - Docx FINALJennifer MedeirosNo ratings yet
- Ayurveda - The Surgical InstrumentsDocument346 pagesAyurveda - The Surgical InstrumentsSumit GonNo ratings yet
- 33 Exp Jan 20Document35 pages33 Exp Jan 20Muhammad YousufNo ratings yet
- LVL G-01 Sheet 1 of 6 - Drainage - Detail 2 SheetDocument1 pageLVL G-01 Sheet 1 of 6 - Drainage - Detail 2 SheetRajasekaran GunasekaranNo ratings yet
- Unknown 79 Mycology University of Adelaide PDFDocument1 pageUnknown 79 Mycology University of Adelaide PDFLinda Gonzalez (Maddy)No ratings yet
- Cleaningvssanitizingservsafe1583366413072 PDFDocument2 pagesCleaningvssanitizingservsafe1583366413072 PDFHenry SNo ratings yet
- ArticleDocument10 pagesArticleperley.matiasNo ratings yet
- Arne Langaskens - HerbalistDocument3 pagesArne Langaskens - HerbalistFilipNo ratings yet
- Basic Training: Elementary First Aid: Written AssessmentDocument2 pagesBasic Training: Elementary First Aid: Written AssessmentClark LlameraNo ratings yet
- Swim Training Plan 5k ImproverDocument8 pagesSwim Training Plan 5k Improver8b6hjzhqwtNo ratings yet
- Popular Notions About Discipline of PsychologyDocument5 pagesPopular Notions About Discipline of PsychologyThe noble savageNo ratings yet
- List of ReferencesDocument3 pagesList of ReferencesRave MiradoraNo ratings yet
- Mine? ? ??Document16 pagesMine? ? ??Samskruthi ChallaNo ratings yet
- Tummo EssenceDocument7 pagesTummo EssenceJose AssuncaoNo ratings yet
- Ca1 PrelimDocument60 pagesCa1 PrelimAira EspleguiraNo ratings yet
- Cephalosporin UnitDocument11 pagesCephalosporin Unitviper1402No ratings yet
- EU Approved Units EIA - MaharashtraDocument7 pagesEU Approved Units EIA - MaharashtragibinkumarNo ratings yet
- Jurnal Ckd-EpiDocument6 pagesJurnal Ckd-EpinezaNo ratings yet
- Oral Pathology Flipchart - Carissa WachendorfDocument18 pagesOral Pathology Flipchart - Carissa Wachendorfapi-499223511No ratings yet
- What Is Crystal Methamphetamine?Document2 pagesWhat Is Crystal Methamphetamine?losangelesNo ratings yet
- Walkthrough21 PDFDocument51 pagesWalkthrough21 PDFAnas SantyNo ratings yet
- List of Empanelled Hospitals & Diagnostic Centres DGEHSDocument33 pagesList of Empanelled Hospitals & Diagnostic Centres DGEHSaaryan0% (2)
- Group Assignment RAP SWOT&TOWS HongeditDocument10 pagesGroup Assignment RAP SWOT&TOWS HongeditBùi Thị Thu HồngNo ratings yet
- EAPPQ4W4CADocument9 pagesEAPPQ4W4CAPhebi ReyNo ratings yet
- SJODR 48 555 556 CDocument2 pagesSJODR 48 555 556 Cyasser bedirNo ratings yet
- AgrmmentDocument1 pageAgrmmenthdydueuejeNo ratings yet
- D2 0905 Paediatric Reference Intervals - An Update - Tina YenDocument25 pagesD2 0905 Paediatric Reference Intervals - An Update - Tina YenkamalNo ratings yet