You might also like
- Preparing The Dental O Ce For Medical Emergencies: Harry Dym, DDSDocument4 pagesPreparing The Dental O Ce For Medical Emergencies: Harry Dym, DDSVenkata Ramana Murthy VasupilliNo ratings yet
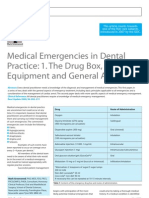
- Medical Emergencies in Dental Practice: 1. The Drug Box, Equipment and General ApproachDocument6 pagesMedical Emergencies in Dental Practice: 1. The Drug Box, Equipment and General ApproachRodelix San Juan Dacanay100% (1)
- Emergency in DentalDocument6 pagesEmergency in Dentalpuskesmas sedatiNo ratings yet
- Medical Emergencies in The Dental OfficeDocument39 pagesMedical Emergencies in The Dental OfficeTimmy ThomasNo ratings yet
- Medical Emergencies: Made By: Nitin Shishodia B.D.S - Iii YearDocument29 pagesMedical Emergencies: Made By: Nitin Shishodia B.D.S - Iii YearDrNagendra Dutt SharmaNo ratings yet
- Clinical Protocol For The Medical Emergency Treatment of Dental PatientsDocument15 pagesClinical Protocol For The Medical Emergency Treatment of Dental Patientsminaxi123No ratings yet
- Medical Emergencies in Dental Practice: A Review: July 2016Document18 pagesMedical Emergencies in Dental Practice: A Review: July 2016AnushkaNo ratings yet
- Anesthesia and Pain Management For Small AnimalsDocument20 pagesAnesthesia and Pain Management For Small Animalspedrojoao.vieiraNo ratings yet
- Table 1: Daniel - Haas@utoronto - Ca Other Sections I. Essential Emergency Drugs Ii. Additional Drugs ReferencesDocument6 pagesTable 1: Daniel - Haas@utoronto - Ca Other Sections I. Essential Emergency Drugs Ii. Additional Drugs ReferencesBasamat Ahmed SharfNo ratings yet
- Medical Emergencies in Dentistry - A Guide To A SuDocument6 pagesMedical Emergencies in Dentistry - A Guide To A SuthirumalasettychintuNo ratings yet
- Generan Anaesthesia For DentistryDocument13 pagesGeneran Anaesthesia For DentistrynissadhaniaNo ratings yet
- 128 Clinical Sedation in Dentistry: Emergency EquipmentDocument1 page128 Clinical Sedation in Dentistry: Emergency EquipmentZhyema ZhyedeeNo ratings yet
- Medical Emergencies in The Dental Practice Poster: Revised and UpdatedDocument8 pagesMedical Emergencies in The Dental Practice Poster: Revised and UpdatedMelissa Gabriela Sánchez SaucedoNo ratings yet
- Assisting in A Medical EmergencyDocument13 pagesAssisting in A Medical EmergencyanayatNo ratings yet
- Me DentalDocument41 pagesMe DentalMuhammadNo ratings yet
- Emergency Nursing ReviewerDocument17 pagesEmergency Nursing ReviewerChannelGNo ratings yet
- Syncope:: The Most Common Medical Emergency in Dentistry Is Syncope, and The MostDocument3 pagesSyncope:: The Most Common Medical Emergency in Dentistry Is Syncope, and The Mostomar alahmariNo ratings yet
- Bdjteam 201655Document4 pagesBdjteam 201655WeasleNotNo ratings yet
- Dentistry EmergenciesDocument5 pagesDentistry EmergenciesSofia PereiraNo ratings yet
- NEJM VICM Viewers ChoiceDocument19 pagesNEJM VICM Viewers ChoiceAnonymous cQWavnNo ratings yet
- Medical Emergency in Paediatric Dental ClinicDocument75 pagesMedical Emergency in Paediatric Dental ClinicAkshay Sreeraman KecheryNo ratings yet
- LA in DentistryDocument10 pagesLA in DentistrybubledewanNo ratings yet
- PER1 1aDocument8 pagesPER1 1aFri FardyNo ratings yet
- Prosthodonticprinciplesin Dentalimplantology: Adjustments in A Coronavirus Disease-19 Pandemic-Battered EconomyDocument31 pagesProsthodonticprinciplesin Dentalimplantology: Adjustments in A Coronavirus Disease-19 Pandemic-Battered Economyramya bodepudiNo ratings yet
- Guideline On Dental Management of Pediatric Patients Receiving Chemotherapy, Hematopoietic Cell Transplantation, And/or RadiationDocument7 pagesGuideline On Dental Management of Pediatric Patients Receiving Chemotherapy, Hematopoietic Cell Transplantation, And/or RadiationMariele Pototski AmenabarNo ratings yet
- Uhns Guidelines 2010Document187 pagesUhns Guidelines 2010varrakesh100% (1)
- Airway and The NurseDocument7 pagesAirway and The NursecarmenbuleandraNo ratings yet
- FumigationDocument6 pagesFumigationmd kaleemNo ratings yet
- DiffairwayDocument54 pagesDiffairwayJim HoffmanNo ratings yet
- Medical Emergencies in Dental PracticeDocument201 pagesMedical Emergencies in Dental PracticeIoana100% (1)
- Nasolaryngoscopy: Scott E. MoserDocument5 pagesNasolaryngoscopy: Scott E. Moserriski novitaNo ratings yet
- Boyce, 2021Document32 pagesBoyce, 2021Matheus Souza Campos CostaNo ratings yet
- Final Hospital TrainingDocument41 pagesFinal Hospital Trainingakaarya123456789No ratings yet
- ME and Resus Standards Resus Council UKDocument41 pagesME and Resus Standards Resus Council UKklopine1234No ratings yet
- Anaesthesia For Paediatric Dentistry: Lola Adewale MBCHB DCH FrcaDocument8 pagesAnaesthesia For Paediatric Dentistry: Lola Adewale MBCHB DCH FrcaJavier Farias VeraNo ratings yet
- Code of Practice Regarding Medical Emergencies May 2023Document24 pagesCode of Practice Regarding Medical Emergencies May 2023Saman ArshadNo ratings yet
- Dental Management For Patient With Asthmatic Attack: Supervision By: DR Ahmed Maky (M.SC Oral Surgeon)Document12 pagesDental Management For Patient With Asthmatic Attack: Supervision By: DR Ahmed Maky (M.SC Oral Surgeon)Mustafa AlobaidiNo ratings yet
- Hospital Training AmitDocument23 pagesHospital Training AmitajayNo ratings yet
- COP EmergencyDocument15 pagesCOP EmergencyOyinlola EbenezerNo ratings yet
- Dental Settings: Key ConceptsDocument7 pagesDental Settings: Key ConceptsVigneshvar SreekanthNo ratings yet
- Autoclaving ProtocolsDocument25 pagesAutoclaving ProtocolsSerene KennyNo ratings yet
- Organization of Occupational Health ServicesDocument54 pagesOrganization of Occupational Health ServicesJake MillerNo ratings yet
- Preparation For General AnesthesiaDocument3 pagesPreparation For General AnesthesiaWinda WidhyastutiNo ratings yet
- Sop - KSDCDocument12 pagesSop - KSDCRevan JoshiNo ratings yet
- Bdaguidanceconscious Sedation - Nov 11 PDFDocument13 pagesBdaguidanceconscious Sedation - Nov 11 PDFvishali sethiNo ratings yet
- P1337425217053 (Annisaa Sittatunnikmah) Tugas EpidDocument4 pagesP1337425217053 (Annisaa Sittatunnikmah) Tugas EpidannisaaNo ratings yet
- First AidDocument20 pagesFirst AidDurchessNo ratings yet
- Pediatric Dentistry: The Use of Nitrous Oxide Inhalation Sedation For Dental Treatment in Agitated ChildrenDocument15 pagesPediatric Dentistry: The Use of Nitrous Oxide Inhalation Sedation For Dental Treatment in Agitated ChildrenmahmoodNo ratings yet
- Symposium Papers: Emergency Airway ManagementDocument10 pagesSymposium Papers: Emergency Airway Managementdewin21No ratings yet
- Dental Laboratory Infection ControlDocument6 pagesDental Laboratory Infection ControlDrShweta SainiNo ratings yet
- Use of Local Anesthesia For Pediatric Dental PatientsDocument11 pagesUse of Local Anesthesia For Pediatric Dental PatientsAtirah AchmadNo ratings yet
- Pediatrics 1998 E13Document20 pagesPediatrics 1998 E13Jelai ParaisoNo ratings yet
- International JournalDocument5 pagesInternational JournalPutri Nur HandayaniNo ratings yet
- Medical Emergencies in The Pediatric Dental Patient: Stephen J. Goepferd, D.D.S., M.SDocument7 pagesMedical Emergencies in The Pediatric Dental Patient: Stephen J. Goepferd, D.D.S., M.SAGUNG PRASETYONo ratings yet
- CDPH Guidelines Dental Antibiotic UseDocument5 pagesCDPH Guidelines Dental Antibiotic UseAMVTNo ratings yet
- 16 Complications in Anaesthesia PDFDocument0 pages16 Complications in Anaesthesia PDFjuniorebindaNo ratings yet
- Emergency CareDocument3 pagesEmergency CaremollyNo ratings yet
- Postlaryngectomy voice rehabilitation with voice prosthesesFrom EverandPostlaryngectomy voice rehabilitation with voice prosthesesNo ratings yet
- The Bromley Trust: 1. Organisation DetailsDocument6 pagesThe Bromley Trust: 1. Organisation DetailsFranziska TeşcanNo ratings yet
- Adequation Outil Demande en Supervision Collective 2016 Research ConferenceDocument17 pagesAdequation Outil Demande en Supervision Collective 2016 Research ConferenceGabriel ClericoNo ratings yet
- Nove Farmakološke Strategije U Lečenju Nesitnoćelijskog Karcinoma PlućaDocument8 pagesNove Farmakološke Strategije U Lečenju Nesitnoćelijskog Karcinoma PlućaMomcilo Moca DjurovicNo ratings yet
- Woman Burned by Acid in Random Subway Attack Has 16th SurgeryDocument1 pageWoman Burned by Acid in Random Subway Attack Has 16th Surgeryed2870winNo ratings yet
- Safety Legislation, Regulation and PolicyDocument110 pagesSafety Legislation, Regulation and PolicyNichoNo ratings yet
- Periodic Test 2 Eco Class-12Document4 pagesPeriodic Test 2 Eco Class-12amandeep malikNo ratings yet
- Jawaharlal Nehru Engineering College: Laboratory ManualDocument58 pagesJawaharlal Nehru Engineering College: Laboratory ManualKrishna Vasishta KavuturuNo ratings yet
- A Sample Hospital Business Plan Template - ProfitableVentureDocument15 pagesA Sample Hospital Business Plan Template - ProfitableVentureMacmilan Trevor Jamu100% (1)
- Accredited BAI Laboratory Animal Shelters 2018Document8 pagesAccredited BAI Laboratory Animal Shelters 2018ShanaiaNo ratings yet
- Raw Milk or Packaged Milk?Document2 pagesRaw Milk or Packaged Milk?Marriam TariqNo ratings yet
- HIIT Academy Total Body Blast Phase 1 PDFDocument33 pagesHIIT Academy Total Body Blast Phase 1 PDFAndre ChinassoNo ratings yet
- M.P. Jain Administrative Law - Simran Sabharwal PDFDocument2,247 pagesM.P. Jain Administrative Law - Simran Sabharwal PDFAyush Pandey94% (17)
- Full Download Essentials of Psychiatric Mental Health Nursing 7th Edition Test Bank PDF Full ChapterDocument36 pagesFull Download Essentials of Psychiatric Mental Health Nursing 7th Edition Test Bank PDF Full Chapterdiodontmetacism.0jw2al100% (16)
- Postpartum Depression in Primigravida WomenDocument22 pagesPostpartum Depression in Primigravida WomenMrs RehanNo ratings yet
- RobsurgDocument34 pagesRobsurghotviruNo ratings yet
- Midwives and Nutrition Education During Pregnancy - A Literature RDocument23 pagesMidwives and Nutrition Education During Pregnancy - A Literature RSuredaNo ratings yet
- Intussusception: DR Phillipo Leo ChalyaDocument19 pagesIntussusception: DR Phillipo Leo ChalyaSibabaong'ombe MasakaNo ratings yet
- Villa La Paws Operations Manual-Detail 03-26-2014Document167 pagesVilla La Paws Operations Manual-Detail 03-26-2014Anonymous JKqvy986U100% (1)
- Block Learning Guide (BLG) : Block II Hematoimmunology System (HIS)Document6 pagesBlock Learning Guide (BLG) : Block II Hematoimmunology System (HIS)ASTAGINA NAURAHNo ratings yet
- Amber Sewell: Professional SummaryDocument4 pagesAmber Sewell: Professional Summaryapi-383979726No ratings yet
- Level 2 Unit 39 Assist in The Administration of MedicationDocument7 pagesLevel 2 Unit 39 Assist in The Administration of MedicationSzabolcs LehotaNo ratings yet
- A CDDocument54 pagesA CDDoc QueenieNo ratings yet
- Industrial Counseling HWDocument3 pagesIndustrial Counseling HWJoyce SisonNo ratings yet
- Appendix 26 - SSG Prejoining Ship Check ListDocument1 pageAppendix 26 - SSG Prejoining Ship Check ListEliza's Soothing SoundsNo ratings yet
- Nov Art IsDocument6 pagesNov Art IsSaran KuttyNo ratings yet
- Funda Rle Reviewer - (Prelims)Document8 pagesFunda Rle Reviewer - (Prelims)Jhaztene Mae BaniquedNo ratings yet
- Lions Club Membership Application 111Document2 pagesLions Club Membership Application 111Bolina, Pauline N.No ratings yet
- GHP557 - Fundamentals of Global Health - Syllabus - 28aug2021 - FinalDocument32 pagesGHP557 - Fundamentals of Global Health - Syllabus - 28aug2021 - Finalps.harsha2004No ratings yet
- The ConsulDocument4 pagesThe ConsulPrince Adesina HaastrupNo ratings yet
- Stress MGMT in Call CentersDocument70 pagesStress MGMT in Call CentersJayesh Kambli100% (1)