
Relationship, Social Support, and Personality As Psychosocial Determinants of The Risk For Postpartum Blues
Relationship, Social Support, and Personality As Psychosocial Determinants of The Risk For Postpartum Blues
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Códigos HammDocument20 pagesCódigos HammFelipeMercuri56% (16)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- StarAlmanac 2019 PDFDocument104 pagesStarAlmanac 2019 PDFAfif FarhanNo ratings yet
- Input Output MatrixDocument1 pageInput Output MatrixAlvaro Altamirano100% (2)
- Gladiator Flight ManualDocument84 pagesGladiator Flight ManualJuan Pablo Quintana AmievaNo ratings yet
- Z Score Girls PDFDocument15 pagesZ Score Girls PDFDio Pratama0% (1)
- DS - TLSR8251-E - Datasheet For Telink BLE SoC TLSR8251Document150 pagesDS - TLSR8251-E - Datasheet For Telink BLE SoC TLSR8251毛增No ratings yet
- Learning Autodesk Inventor 2010 Sheet Metal DesignDocument2 pagesLearning Autodesk Inventor 2010 Sheet Metal DesignHazem AlsharifNo ratings yet
- Using Quality Models For Assessing COTS SelectionDocument15 pagesUsing Quality Models For Assessing COTS SelectionAndreea VescanNo ratings yet
- Yade FL KhobDocument47 pagesYade FL Khobsadeq behbehanianNo ratings yet
- CAFCO 300 HS Short Form - Sept 2016Document2 pagesCAFCO 300 HS Short Form - Sept 2016Salman ShaikhNo ratings yet
- ASSIGNMENT - DISCRIBING DIMENSION Bisma Agung Sahputra 3 MCDocument3 pagesASSIGNMENT - DISCRIBING DIMENSION Bisma Agung Sahputra 3 MCEyes BlueNo ratings yet
- Grayloc Installation and Maintenance Bulletin Rev. JDocument4 pagesGrayloc Installation and Maintenance Bulletin Rev. JMax BeeksNo ratings yet
- Day 4 AnswersDocument3 pagesDay 4 AnswersQamar ShahzadNo ratings yet
- EDAF3 AMC Check ListDocument7 pagesEDAF3 AMC Check ListtranhoachbnNo ratings yet
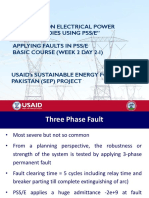
- W-2-Day-2-I - Applying Fault in PSSEDocument9 pagesW-2-Day-2-I - Applying Fault in PSSEKASHIF0% (1)
- Web Services Repeating Groups DataStageDocument32 pagesWeb Services Repeating Groups DataStageCarlosO0% (1)
- BrazingDocument16 pagesBrazingbalamurugan_me100% (3)
- Rectifier SystemDocument20 pagesRectifier SystemDjebali MouradNo ratings yet
- 1 Soft ComputingDocument8 pages1 Soft ComputingSumit KumarNo ratings yet
- Templates in CPPDocument4 pagesTemplates in CPPElango PerumalNo ratings yet
- Anti-Aliasing Filters: Justin Romberg Stephen KruzickDocument3 pagesAnti-Aliasing Filters: Justin Romberg Stephen Kruzickmosco_scridbNo ratings yet
- EcosDocument16 pagesEcosGuruprasad ChoukimathNo ratings yet
- Mcset 1-2-3: MV Distribution Factory Built Assemblies at Your Service AnglaisDocument26 pagesMcset 1-2-3: MV Distribution Factory Built Assemblies at Your Service AnglaisUsman SaeedNo ratings yet
- Ibm Power HaDocument37 pagesIbm Power HaYasmine BoudhinaNo ratings yet
- Viva Questions - CS LabDocument2 pagesViva Questions - CS LabpoornimaNo ratings yet
- ODB++ Output Options: The ODB++ Setup DialogDocument4 pagesODB++ Output Options: The ODB++ Setup DialoghakimNo ratings yet
- Parallel Keys Is.2048.1983Document9 pagesParallel Keys Is.2048.1983sbalajimNo ratings yet
- AWS Inspector's Pocket Hand Book PDFDocument40 pagesAWS Inspector's Pocket Hand Book PDFsamado100% (1)
- Metasploit FrameworkDocument1 pageMetasploit FrameworkPAUL VINCENT FAJARDONo ratings yet
- Computer Networks Homework HelpDocument8 pagesComputer Networks Homework HelpassignmentpediaNo ratings yet




































































You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Códigos HammDocument20 pagesCódigos HammFelipeMercuri56% (16)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- StarAlmanac 2019 PDFDocument104 pagesStarAlmanac 2019 PDFAfif FarhanNo ratings yet
- Input Output MatrixDocument1 pageInput Output MatrixAlvaro Altamirano100% (2)
- Gladiator Flight ManualDocument84 pagesGladiator Flight ManualJuan Pablo Quintana AmievaNo ratings yet
- Z Score Girls PDFDocument15 pagesZ Score Girls PDFDio Pratama0% (1)
- DS - TLSR8251-E - Datasheet For Telink BLE SoC TLSR8251Document150 pagesDS - TLSR8251-E - Datasheet For Telink BLE SoC TLSR8251毛增No ratings yet
- Learning Autodesk Inventor 2010 Sheet Metal DesignDocument2 pagesLearning Autodesk Inventor 2010 Sheet Metal DesignHazem AlsharifNo ratings yet
- Using Quality Models For Assessing COTS SelectionDocument15 pagesUsing Quality Models For Assessing COTS SelectionAndreea VescanNo ratings yet
- Yade FL KhobDocument47 pagesYade FL Khobsadeq behbehanianNo ratings yet
- CAFCO 300 HS Short Form - Sept 2016Document2 pagesCAFCO 300 HS Short Form - Sept 2016Salman ShaikhNo ratings yet
- ASSIGNMENT - DISCRIBING DIMENSION Bisma Agung Sahputra 3 MCDocument3 pagesASSIGNMENT - DISCRIBING DIMENSION Bisma Agung Sahputra 3 MCEyes BlueNo ratings yet
- Grayloc Installation and Maintenance Bulletin Rev. JDocument4 pagesGrayloc Installation and Maintenance Bulletin Rev. JMax BeeksNo ratings yet
- Day 4 AnswersDocument3 pagesDay 4 AnswersQamar ShahzadNo ratings yet
- EDAF3 AMC Check ListDocument7 pagesEDAF3 AMC Check ListtranhoachbnNo ratings yet
- W-2-Day-2-I - Applying Fault in PSSEDocument9 pagesW-2-Day-2-I - Applying Fault in PSSEKASHIF0% (1)
- Web Services Repeating Groups DataStageDocument32 pagesWeb Services Repeating Groups DataStageCarlosO0% (1)
- BrazingDocument16 pagesBrazingbalamurugan_me100% (3)
- Rectifier SystemDocument20 pagesRectifier SystemDjebali MouradNo ratings yet
- 1 Soft ComputingDocument8 pages1 Soft ComputingSumit KumarNo ratings yet
- Templates in CPPDocument4 pagesTemplates in CPPElango PerumalNo ratings yet
- Anti-Aliasing Filters: Justin Romberg Stephen KruzickDocument3 pagesAnti-Aliasing Filters: Justin Romberg Stephen Kruzickmosco_scridbNo ratings yet
- EcosDocument16 pagesEcosGuruprasad ChoukimathNo ratings yet
- Mcset 1-2-3: MV Distribution Factory Built Assemblies at Your Service AnglaisDocument26 pagesMcset 1-2-3: MV Distribution Factory Built Assemblies at Your Service AnglaisUsman SaeedNo ratings yet
- Ibm Power HaDocument37 pagesIbm Power HaYasmine BoudhinaNo ratings yet
- Viva Questions - CS LabDocument2 pagesViva Questions - CS LabpoornimaNo ratings yet
- ODB++ Output Options: The ODB++ Setup DialogDocument4 pagesODB++ Output Options: The ODB++ Setup DialoghakimNo ratings yet
- Parallel Keys Is.2048.1983Document9 pagesParallel Keys Is.2048.1983sbalajimNo ratings yet
- AWS Inspector's Pocket Hand Book PDFDocument40 pagesAWS Inspector's Pocket Hand Book PDFsamado100% (1)
- Metasploit FrameworkDocument1 pageMetasploit FrameworkPAUL VINCENT FAJARDONo ratings yet
- Computer Networks Homework HelpDocument8 pagesComputer Networks Homework HelpassignmentpediaNo ratings yet