You might also like
- The Difference Between Absolute Neutrophils, Neutrophil/ Lymphocyte Ratio and Platelet/Lymphocyte Ratio in Normal, Nstemi, Stemi PatientsDocument6 pagesThe Difference Between Absolute Neutrophils, Neutrophil/ Lymphocyte Ratio and Platelet/Lymphocyte Ratio in Normal, Nstemi, Stemi PatientsansariadistaNo ratings yet
- Manual Aspiration Thrombectomy in Acute Myocardial Infarction: A Clinical ExperienceDocument9 pagesManual Aspiration Thrombectomy in Acute Myocardial Infarction: A Clinical ExperienceArdiana FirdausNo ratings yet
- Management of No-Re Ow Phenomenon in The Catheterization LaboratoryDocument9 pagesManagement of No-Re Ow Phenomenon in The Catheterization LaboratoryRajendra ChavanNo ratings yet
- Becattini 2018Document25 pagesBecattini 2018Snezana MihajlovicNo ratings yet
- Acute Myocardial InfarctionDocument12 pagesAcute Myocardial InfarctionRoberto López Mata100% (1)
- Iam NejmDocument13 pagesIam NejmEduardo GálvezNo ratings yet
- Acute Myocardial Infarction: Review ArticleDocument12 pagesAcute Myocardial Infarction: Review ArticleNoel Saúl Argüello SánchezNo ratings yet
- MNJ ToastDocument4 pagesMNJ ToastRichard SuherlimNo ratings yet
- Dogan 2012Document7 pagesDogan 2012Davy JonesNo ratings yet
- Dolor Toracico Evaluacion CORONARIO Med Clin North Am 2015 JulioDocument13 pagesDolor Toracico Evaluacion CORONARIO Med Clin North Am 2015 Juliojavier ariasNo ratings yet
- Clinical Problems in Stroke PatientsDocument28 pagesClinical Problems in Stroke PatientsYusriyaniNo ratings yet
- 2017 - 05 - 25 NEJM Acute Myocardial InfarctionDocument12 pages2017 - 05 - 25 NEJM Acute Myocardial InfarctionPedro SanchezNo ratings yet
- THE Difference Between Absolute Neutrophils, Neutrophil/ Lymphocyte Ratio and Platelet/Lymphocyte Ratio in Normal, Nstemi, Stemi PatientsDocument9 pagesTHE Difference Between Absolute Neutrophils, Neutrophil/ Lymphocyte Ratio and Platelet/Lymphocyte Ratio in Normal, Nstemi, Stemi PatientsibnusinaNo ratings yet
- Ischemic 39!Document6 pagesIschemic 39!Adina Alexandra CNo ratings yet
- Cetin 2016Document10 pagesCetin 2016Della Puspita SariNo ratings yet
- Original Research Abstract AFCC ASMIHA 2019Document82 pagesOriginal Research Abstract AFCC ASMIHA 2019Program Studi Kardiologi100% (1)
- Acute Myocardial Infarction: Review ArticleDocument12 pagesAcute Myocardial Infarction: Review ArticleKathryn LevineNo ratings yet
- Art 3A10.1007 2Fs00415 016 8189 XDocument7 pagesArt 3A10.1007 2Fs00415 016 8189 XIrmagian PaleonNo ratings yet
- Acute Coronary Syndromes: Unstable Angina and Non-ST Elevation Myocardial InfarctionDocument18 pagesAcute Coronary Syndromes: Unstable Angina and Non-ST Elevation Myocardial InfarctionLOZANO GARCIA PAOLA ALEJADRANo ratings yet
- 1071 4385 1 PBDocument8 pages1071 4385 1 PBsarahNo ratings yet
- Stroke Prevention and Treatment in Sickle Cell Disease: Robert J. Adams, MS, MDDocument4 pagesStroke Prevention and Treatment in Sickle Cell Disease: Robert J. Adams, MS, MDMeshaki MbarukaNo ratings yet
- Jurnal 1Document10 pagesJurnal 1fitri juliantiNo ratings yet
- Higher Prevalence of Diabetes in Pontine Infarction Than inDocument8 pagesHigher Prevalence of Diabetes in Pontine Infarction Than inMarshall ThompsonNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofahmadto80No ratings yet
- Anderson 2017Document24 pagesAnderson 2017muh.fitrah ramadanNo ratings yet
- Brain Arteriovenous MalformationsDocument20 pagesBrain Arteriovenous MalformationsTony NgNo ratings yet
- DIABtunismedv100i2-143-148 18Document6 pagesDIABtunismedv100i2-143-148 18marsim92No ratings yet
- LIMA As A Graft For CABG in Polyarteritis NodosaDocument3 pagesLIMA As A Graft For CABG in Polyarteritis Nodosavam buddhaNo ratings yet
- Chest Pain Evaluation in ERDocument13 pagesChest Pain Evaluation in ERirmaNo ratings yet
- 58-63 DallAra JIC 2020 Feb WMDocument6 pages58-63 DallAra JIC 2020 Feb WMJose Manuel Ornelas-AguirreNo ratings yet
- Thesis Acute Coronary SyndromeDocument8 pagesThesis Acute Coronary Syndromeaflpcdwfunzfed100% (2)
- Nikus 2006Document5 pagesNikus 2006Robby Paguh TariganNo ratings yet
- Different Clinical Phenotypes of Embolic Stroke of Undetermined Source: A Subgroup Analysis of 86 PatientsDocument9 pagesDifferent Clinical Phenotypes of Embolic Stroke of Undetermined Source: A Subgroup Analysis of 86 PatientsSuryati HusinNo ratings yet
- Cryptogenic Stroke 2016Document10 pagesCryptogenic Stroke 2016tatukyNo ratings yet
- Factores para FNRDocument10 pagesFactores para FNRPOMYNo ratings yet
- Cryptogenic Stroke: Clinical PracticeDocument10 pagesCryptogenic Stroke: Clinical PracticenellieauthorNo ratings yet
- Clinical and Applied Thrombosis/HemostasisDocument8 pagesClinical and Applied Thrombosis/HemostasisPicha PichiNo ratings yet
- Spontaneous Coronary Artery Dissection With Clinical Presentation of Acute Myocardial InfarctionDocument3 pagesSpontaneous Coronary Artery Dissection With Clinical Presentation of Acute Myocardial InfarctionSabrina JonesNo ratings yet
- Prevalence, Clinical Features, and Prognosis of Acute Myocardial Infarction Attributable To Coronary Artery EmbolismDocument10 pagesPrevalence, Clinical Features, and Prognosis of Acute Myocardial Infarction Attributable To Coronary Artery EmbolismNoel Saúl Argüello SánchezNo ratings yet
- Diagnosis and Management of Splanchnic Ischemia: Ioannis E Koutroubakis, MD, PHD, Assistant Professor of MedicineDocument12 pagesDiagnosis and Management of Splanchnic Ischemia: Ioannis E Koutroubakis, MD, PHD, Assistant Professor of MedicineIgorCotagaNo ratings yet
- Jurnal Coronary Angiography Findings in Patients at Robert Wolter Monginsidi Hospital-ManadoDocument4 pagesJurnal Coronary Angiography Findings in Patients at Robert Wolter Monginsidi Hospital-ManadoRettyNo ratings yet
- Diagnosis of Myocardial Infarction at Autopsy: AECVP Reappraisal in The Light of The Current Clinical ClassificationDocument16 pagesDiagnosis of Myocardial Infarction at Autopsy: AECVP Reappraisal in The Light of The Current Clinical ClassificationFernanda GarcíaNo ratings yet
- AnatolJCardiol 15 8 640 647Document8 pagesAnatolJCardiol 15 8 640 647Pangestu DhikaNo ratings yet
- J Interven Cardiol. 2017 1-7.: Presented By: Dr. Yusrina BR Saragih Supervisor: DR - Dr. Zulfikri Mukhtar, Sp. JP (K)Document24 pagesJ Interven Cardiol. 2017 1-7.: Presented By: Dr. Yusrina BR Saragih Supervisor: DR - Dr. Zulfikri Mukhtar, Sp. JP (K)Yusrina Njoes SaragihNo ratings yet
- Natural History of Asymptomatic Severe Aortic StenosisDocument11 pagesNatural History of Asymptomatic Severe Aortic StenosisGaal PinNo ratings yet
- Carotid StentDocument9 pagesCarotid StentCut FadmalaNo ratings yet
- 0102 7638 RBCCV 37 06 0829Document7 pages0102 7638 RBCCV 37 06 0829dr.baristimurNo ratings yet
- 10.1038@s41572 019 0090 3Document20 pages10.1038@s41572 019 0090 3sari100% (1)
- Ekg STDocument23 pagesEkg STisaNo ratings yet
- 2359 4802 Ijcs 34 05 s01 0012.x98175Document10 pages2359 4802 Ijcs 34 05 s01 0012.x98175Suryati HusinNo ratings yet
- Practneurol 2020 002763Document12 pagesPractneurol 2020 002763Fitri ainun MalahayatiNo ratings yet
- Minoca - Are We Doing It Wrong?Document6 pagesMinoca - Are We Doing It Wrong?khusnulNo ratings yet
- Ajc 16 12 980 989Document10 pagesAjc 16 12 980 989Maria Goretty L. TobingNo ratings yet
- 10 1056@NEJMra1503884 PDFDocument10 pages10 1056@NEJMra1503884 PDFmarselamgeNo ratings yet
- AggarwalDocument7 pagesAggarwalSuryaNo ratings yet
- Scientific Report Journal 22 NovDocument6 pagesScientific Report Journal 22 Novnaresh kotraNo ratings yet
- Cerebral Venous Thrombosis: J.M.CoutinhoDocument7 pagesCerebral Venous Thrombosis: J.M.CoutinhoWilliam ReinaldyNo ratings yet
- Practical Management of Systemic Sclerosis in Clinical PracticeFrom EverandPractical Management of Systemic Sclerosis in Clinical PracticeNo ratings yet
- Microcirculation in Cardiovascular DiseasesFrom EverandMicrocirculation in Cardiovascular DiseasesEnrico Agabiti-RoseiNo ratings yet
- Microcirculation: From Bench to BedsideFrom EverandMicrocirculation: From Bench to BedsideMaria DorobantuNo ratings yet
- Pneumonics For AclsDocument2 pagesPneumonics For Aclskrishnaprasadm7100% (2)
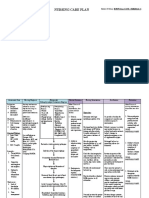
- NCP Mugar Icu3 Batch2 GRP3Document2 pagesNCP Mugar Icu3 Batch2 GRP3FRANZI ALYANNA MUGARNo ratings yet
- ACLS Algorithms 3Document1 pageACLS Algorithms 3frankie-jay paicotNo ratings yet
- Transportation in Animals and PlantsDocument2 pagesTransportation in Animals and PlantsHimanshi JainNo ratings yet
- CHD ModuleDocument204 pagesCHD ModuleKellie RollinsNo ratings yet
- Xducers & P-MonitorsDocument22 pagesXducers & P-MonitorschanlalNo ratings yet
- International Journal of Scientific Research: General MedicineDocument4 pagesInternational Journal of Scientific Research: General MedicineTriple ANo ratings yet
- Corazon AnatomiaDocument10 pagesCorazon AnatomiaMariaAndreaRuizVelásquezNo ratings yet
- Diagnosis and Treatment of Shock: Dr. Refli Hasan SPPD, SPJP (K) FihaDocument37 pagesDiagnosis and Treatment of Shock: Dr. Refli Hasan SPPD, SPJP (K) FihaWinson ChitraNo ratings yet
- Angiography and ArteriographyDocument64 pagesAngiography and ArteriographyRyBone95100% (1)
- Answer Diagnosis: 1. RhythmDocument2 pagesAnswer Diagnosis: 1. RhythmSuggula Vamsi KrishnaNo ratings yet
- Left Atrial Function: Physiology, Assessment, and Clinical ImplicationsDocument10 pagesLeft Atrial Function: Physiology, Assessment, and Clinical ImplicationsfitriasyrofianaNo ratings yet
- C70 Modular Monitor Product SpecificationsDocument15 pagesC70 Modular Monitor Product SpecificationsDayani Gomez Escobar100% (1)
- Tetralogy of Fallot CASE STUDYDocument12 pagesTetralogy of Fallot CASE STUDYMaricel Agcaoili GallatoNo ratings yet
- ArticolsssaDocument11 pagesArticolsssaCosmin GabrielNo ratings yet
- 6th HEAD & NECK ANATOMICAL LAB D.NASSR ALHUTBANY BLOOD SUPPLY OF HEAD & NECK 2024Document47 pages6th HEAD & NECK ANATOMICAL LAB D.NASSR ALHUTBANY BLOOD SUPPLY OF HEAD & NECK 2024Dr.NASSR AL-HUTBANYNo ratings yet
- Insuficienta Venoasa CronicaDocument84 pagesInsuficienta Venoasa CronicaIulyaNo ratings yet
- 382-Article Text-2683-5-10-20191027Document14 pages382-Article Text-2683-5-10-20191027Nanda NovitaNo ratings yet
- Jurnal JantungDocument5 pagesJurnal JantungFileo AdisonNo ratings yet
- Approach To Diagnosis of Congenital Heart DiseasesDocument85 pagesApproach To Diagnosis of Congenital Heart DiseasesNirav CHOVATIYANo ratings yet
- Spontaneous Coronary Artery Dissection With Clinical Presentation of Acute Myocardial InfarctionDocument3 pagesSpontaneous Coronary Artery Dissection With Clinical Presentation of Acute Myocardial InfarctionSabrina JonesNo ratings yet
- Programme Gulfpcr2023Document21 pagesProgramme Gulfpcr2023Abid KhanNo ratings yet
- Hospital and Critical CareDocument16 pagesHospital and Critical CareMarivy GalonNo ratings yet
- iGA BioMonitor Mul-14 394120-E 2014-03-03 enDocument152 pagesiGA BioMonitor Mul-14 394120-E 2014-03-03 enFatema IsmatiNo ratings yet
- Cardiac Output 2019Document17 pagesCardiac Output 2019crappy blue angelNo ratings yet
- Circle of VillisDocument17 pagesCircle of VillisAradhana SamuelNo ratings yet
- EECP Clinical ResultsDocument44 pagesEECP Clinical ResultsAryadhi TevataqsaNo ratings yet
- Film-Coated Tablet 5mg & 7.5mg: CH O OCH CH N N ODocument2 pagesFilm-Coated Tablet 5mg & 7.5mg: CH O OCH CH N N ObadrhashmiNo ratings yet
- The Cardiovascular SystemDocument23 pagesThe Cardiovascular Systemrobhel740% (2)
- Comparison of Inflammatory Markers in HTNDocument6 pagesComparison of Inflammatory Markers in HTNDan JohnstonNo ratings yet