Professional Documents
Culture Documents
Brain Arteriovenous Malformations
Uploaded by
Tony NgOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Brain Arteriovenous Malformations
Uploaded by
Tony NgCopyright:
Available Formats
PRIMER
Brain arteriovenous malformations
Michael T. Lawton1, W. Caleb Rutledge1, Helen Kim2, Christian Stapf3,
Kevin J. Whitehead4, Dean Y. Li4, Timo Krings5, Karel terBrugge5, Douglas Kondziolka6,
Michael K. Morgan7, Karam Moon8 and Robert F. Spetzler8
Abstract | An arteriovenous malformation is a tangle of dysplastic vessels (nidus) fed by arteries and drained
by veins without intervening capillaries, forming a high-flow, low-resistance shunt between the arterial and
venous systems. Arteriovenous malformations in the brain have a low estimated prevalence but are an
important cause of intracerebral haemorrhage in young adults. For previously unruptured malformations,
bleeding rates are approximately 1% per year. Once ruptured, the subsequent risk increases fivefold,
depending on associated aneurysms, deep locations, deep drainage and increasing age. Recent findings
from novel animal models and genetic studies suggest that arteriovenous malformations, which were long
considered congenital, arise from aberrant vasculogenesis, genetic mutations and/or angiogenesis after
injury. The phenotypical characteristics of arteriovenous malformations differ among age groups, with
fistulous lesions in children and nidal lesions in adults. Diagnosis mainly involves imaging techniques,
including CT, MRI and angiography. Management includes observation, microsurgical resection,
endovascular embolization and stereotactic radiosurgery, alone or in any combination. There is little
consensus on how to manage patients with unruptured malformations; recent studies have shown that
patients managed medically fared better than those with intervention at short-term follow‑up. By contrast,
interventional treatment is preferred following a ruptured malformation to prevent rehaemorrhage.
Management continues to evolve as new mechanistic discoveries and reliable animal models raise the
possibility of developing drugs that might prevent the formation of arteriovenous malformations, induce
obliteration and/or stabilize vessels to reduce rupture risk. For an illustrated summary of this Primer, visit:
http://go.nature.com/TMoAdn
The four major types of vascular malformations include and/or stereotactic radiosurgery, alone or in any combi-
venous malformations, cavernous malformations, nation. Microsurgery aims to produce curative resection,
telangiectases and arteriovenous malformations. An with transarterial embolization used as a preoperative
arteriovenous malformation is a tangle of dysplastic ves- adjunct. Stereotactic radiosurgery delivers radiation that
sels comprising a nidus fed by arteries, drained by veins leads to obliteration of the arteriovenous malformation
and without intervening capillaries, forming a high- over a 2–3 year latency period. Diagnosis mainly involves
flow, low-resistance conduit that shunts blood from the medical imaging such as CT, MRI and angiography.
arterial to the venous system (FIG. 1). They are the most
spectacular type of vascular malformation, with dilated Epidemiology
arteries converging from all directions and engorged On the basis of large-scale imaging data from seemingly
veins twisting and throbbing from the turbulence of healthy volunteers, one brain arteriovenous malforma-
shunted blood flow. This Primer will focus only on tion is found in every 2,000 MRI scans, which adds up
Correspondence to M.T.L.
brain arteriovenous malformations but will not address to an estimated prevalence of approximately 50 cases
e-mail: michael.lawton@
ucsf.edu
dural arteriovenous fistulas, cavernous malformations or per 100,000 (95% confidence interval (CI) 10–100)1.
Department of Neurological other vascular malformations in the brain. The crude annual detection rate or incidence is esti-
Surgery, University of Arteriovenous malformations are highly varied in mated at 1.3 per 100,000 patient years with relatively
California, 505 Parnassus size, shape and location, making each malformation dif- stable detection rates across populations. Improved
Avenue, M780,
San Francisco,
ferent, but patterns emerge and recognizable subtypes access to diagnostic MRI might explain the increasing
California 94143, USA. with definable anatomy appear that enable a certain detection rates of unruptured arteriovenous malforma-
degree of classification. In addition, their character tions, whereas the incidence of ruptured arteriovenous
Article number: 15008
doi:10.1038/nrdp.2015.8
istics vary with patients’ age, and so do the imaging and malformations seems remarkably stable over time2–5
Published online treatment options. In addition to conservative observa- (TABLE 1). Arteriovenous malformations in the brain
28 May 2015 tion, management includes microsurgery, embolization are usually found in young adults between the ages of
NATURE REVIEWS | DISEASE PRIMERS VOLUME 1 | 2015 | 1
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
Author addresses
is that these tend to be associated with a higher risk
of stroke and neurological deficits during short-term
1
Department of Neurological Surgery, University of California, 505 Parnassus Avenue, (3 years) follow‑up13,23,24. For patients with arteriovenous
M780, San Francisco, California 94143, USA. malformation-associated epilepsy, population-based
2
Department of Anesthesia and Perioperative Care, University of California, data do not confirm a long-term benefit of arteriovenous
San Francisco, USA.
malformation eradication on future seizure occurrence25.
3
Department of Neurology, APHP Hôpital Lariboisière, Paris, France, and DHU Neurovasc,
Université Paris Diderot, Paris, France.
4
Department of Internal Medicine, University of Utah, Salt Lake City, Utah, USA. Mechanisms/pathophysiology
5
Department of Medical Imaging, University of Toronto, Ontario, Canada. The pathogenesis of brain arteriovenous malformations
6
Neurological Surgery, University of Pittsburgh, Pennsylvania, USA. remains unclear. They have long been considered con-
7
Clinical Medicine, Macquarie University, Sydney, Australia. genital, despite a lack of supporting evidence. Possible
8
Division of Neurological Surgery, Barrow Neurological Institute, Phoenix, Arizona, USA. causes might be miscues or miscommunications dur-
ing embryogenesis at the time that arteries and veins are
in direct contact without intervening capillaries. If this
20 and 40 years6. Approximately half of patients present phenomenon persists after birth, instead of maturing into
with intracranial haemorrhage; the remaining patients a normal vascular architecture, arteriovenous malforma-
have focal or generalized seizures (20–25%), headaches, tions arise. They might also develop as a result of under-
focal neurological deficits or no symptoms (15%)7–11. lying genetic abnormalities that produce signalling errors
For previously unruptured arteriovenous malforma- and structural defects. Another possibility is that arterio-
tions, the rate of haemorrhage is low (approximately 1% venous malformations are not congenital but acquired
per year) but increases fivefold once ruptured12–15 (TABLE 1). after an injury, similar to dural arteriovenous fistulas26.
Additional risk factors for future bleeding include increas-
ing patient age, Hispanic ethnicity, exclusively deep Artery and vein formation
venous drainage, deep location and radiological evidence To support the increased metabolic demands of a large,
of previous haemorrhage. By contrast, the independent active organism, vertebrates evolved a closed circulatory
effects of the nidus size, infratentorial location, associ- system. Blood vessels emerged as distinct anatomical
ated unruptured aneurysms and venous dilatations have conduits to transport nutrients to (arteries) and remove
not been confirmed in a prospective follow‑up study of waste from (veins) tissues. Arteries are thick-walled ves-
untreated patients12,16–18. Women do not show higher rup- sels that are built to withstand the high-pressure flow
ture rates during pregnancy and puerperium, although needed to supply target tissues. By contrast, veins are
reports in the literature differ on this issue. In addition, larger, thin-walled, low-pressure vessels that convey
very low prevalence of brain arteriovenous malforma- blood back to the heart, aided by valves that establish
tions within families justifies that systematic screening of directional flow and that combat gravity. Arteries and
first‑degree family members is not needed19,20. veins often follow a parallel and counter-current course
Overall, the clinical consequences of a rupture of an but do not communicate directly. In fact, they are separ
arteriovenous malformation in the brain are more benign ated by capillary networks in target tissues, and speci
than intracranial haemorrhage attributed to other causes. fic control systems exist to prevent the formation of
However, patients with a prior rupture show increased premature arteriovenous connections during develop-
long-term mortality rates compared with healthy con- ment and to maintain homeostasis of the vasculature
trols if left untreated21,22. A drawback for preventive inter- (FIG. 1). Arteriovenous malformations probably occur as
ventions for unruptured arteriovenous malformations a consequence of a failure in this control system.
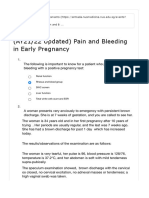
a Normal b AVM
Rupture with local
damage and
Steal haemorrhage
phemonema
Arteries Veins
Capillary network Low resistance = High flow
Figure 1 | Schematic representation of normal vasculature and an arteriovenous malformation.
Nature Reviews |aDisease
| In normal
Primers
circumstances, arteries and veins maintain strict distinctions and communicate only at the capillary bed.
b | Arteriovenous malformations (AVMs) are the result of direct connections between high-flow arterial vessels and
low-resistance venous capacitance vessels. Clinical consequences result from the direct and indirect effects of flow
disturbances and rupture-associated haemorrhage. Blood flow around an AVM prefers the low-resistance shunt
through the malformation over the surrounding capillary networks, thereby ‘stealing’ blood flow from adjacent brain
(the steal phenomenon).
2 | 2015 | VOLUME 1 www.nature.com/nrdp
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
Table 1 | Detection and spontaneous rupture rates of brain AVMs in untreated patients
Detection rates Spontaneous rupture rates
Number per 100,000 per year (95% CI) Observed crude annual percentages (95% CI)
Study Ruptured Unruptured Total Ruptured Unruptured Total
Prospective population-based data sets
New York Islands 0.51 0.83 1.34 NA NA NA
AVM Study2 (0.41–0.61) (0.77–0.88) (1.18–1.49)
NOMASS3 0.55 NA NA NA NA NA
(0.11–1.61)
SIVMS4 0.51 0.61 1.12 NA NA NA
(0.37–0.69) (0.52–0.68) (0.90–1.37)
Retrospective population-based data sets
KPNC5 0.70 0.72 1.42 3.3% 0.7% 4.0%
(0.60–0.80) (0.63–0.83) (1.29–1.57) (2.9–3.6) (0.4–1.0) (3.8–4.2)
Finland15 NA NA NA 2.8 1.6 2.4
(2.4–3.2) (1.1–2.0) (1.9–2.8)
Patient-level meta-analysis, randomized data
MARS12 NA NA NA 4.8% 1.3% 2.3%
(3.9–5.9) (1.0–1.7) (2.0–2.7)
ARUBA13 NA NA NA NA 2.2% NA
(0.9–4.5)
ARUBA, A Randomized Trial for Unruptured Brain AVMs; AVM, arteriovenous malformation; KPNC, Kaiser Permanente of Northern
California; MARS, Multicenter AVM Research Study; NA, not analysed; NOMASS, Northern Manhattan Stroke Study; SIVMS,
Scottish Intracranial Vascular Malformation Study.
The circulatory system develops through the dif- distinctive molecular profile. Venous endothelial cell fate
ferentiation of pluripotent angioblasts into endocardial was once thought to be the default pathway that occurred
and endothelial cells in a process called vasculogenesis27. when arterial specification factors were absent. However,
The network of interconnected endothelial cells forms a development of the venous phenotype now seems to be
lumen and communicates with paired heart tubes, which influenced directly by the retinoic acid-activated receptor
are lined by endocardial cells and are equipped to pres- COUP-transcription factor 2 (COUP‑TF2)36. Expression
surize the system with rhythmic contraction. Primitive of COUP‑TF2 suppresses the expression of artery-
vascular beds are converted into arteries, capillaries and specific genes and promotes expression of the venous
veins through a remodelling process (angiogenesis) marker EPH receptor B4 (EPHB4)37.
in response to molecular signals (angiogenic factors).
Angiogenic factors regulate the proliferation, migra- Arteriovenous malformation syndromes
tion and organization of endothelial cells, as well as the Most arteriovenous malformations are observed as
growth and maturation of vessels. Different angiogenic single, isolated or sporadic lesions in individuals, with-
factors, as well as different expression levels of various out a clear genetic basis. The cause for the failure of
factors, ensure a distinct arterial or venous identity. Even arteriovenous separation in these sporadic events is
when the morphology of arteries and veins seem to be unclear. Occasionally, multiple lesions in individuals
similar early on in development, distinct genetic and with genetic arteriovenous malformation syndromes are
molecular differences are present28,29. observed, which has provided insight into some of the
Vascular endothelial growth factor (VEGF) is an crucial signalling pathways that govern arteriovenous
important regulator of angiogenesis and vasculogenesis patterning (FIG. 2b).
(FIG. 2a). Its activity is mediated by VEGF receptors Hereditary haemorrhagic telangiectasia, also referred
(VEGFR1 and VEGFR2) and modulated by a series of to as Osler–Weber–Rendu syndrome, is an autosomal
additional co‑receptors27,28,30. The VEGF co‑receptor dominant disorder characterized by microscopic vascu-
neuropilin 1 (NRP1) is expressed on arterial endo lar malformations (known as telangiectases) at muco
thelial cells and regulates arterial differentiation31,32. cutaneous surfaces and by macroscopic arteriovenous
Ephrin B2 and Notch family members are also expressed malformations in internal organs, predominantly the liver,
by the arterial endothelium. Notch signalling, which is lungs and brain38. Hereditary haemorrhagic telangiectasia
important for maintaining arterial identity 33, is activated most commonly presents as epistaxis (nose bleed) owing
by sonic hedgehog (SHH)-stimulated expression of to ruptured telangiectases of the nasal mucosa, but bleed-
VEGF34. Forkhead transcription factors such as FOXC1 ing in the brain also occurs and is an important cause of
and FOXC2 interact with the Notch signalling pathway premature morbidity and mortality. This genetic condi-
to regulate Notch target gene expression35. Similar to tion revealed new genetic pathways governing arterio-
arterial endothelial cells, venous endothelial cells have a venous distinction. The causative genes in this condition
NATURE REVIEWS | DISEASE PRIMERS VOLUME 1 | 2015 | 3
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
are members of the transforming growth factor‑β (TGFβ) that interacts with endoglin on the endothelial cell sur-
family. For example, endoglin is a TGFβ co-receptor with- face to bind ligands and to stimulate kinase activity 41.
out a clear signalling function, and mutations in the gene Ligand binding results in the activation of SMAD pro-
encoding endoglin (ENG) causes hereditary haemor teins in the cytoplasm that ultimately leads to nuclear
rhagic telangiectasia type 1 (REF. 39). Mutations in the translocation and activation of SMAD4. Mutations in
gene encoding activin receptor-like kinase 1 (ALK1; also SMAD4 result in a combined syndrome of hereditary
known as ACVRL1) cause type 2 hereditary haemor- haemorrhagic telangiectasia with juvenile polyposis42.
rhagic telangiectasia40. ALK1 is a type 1 TGFβ receptor Bone morphogenetic proteins (BMP9 and BMP10) bind
ALK1 with high affinity and induce downstream SMAD
a signalling 43. The above-normal serum concentrations
SHH of BMP9 observed in patients with hereditary haemor-
rhagic telangiectasia suggest that BMP9 is involved in
VEGF
angiogenesis, although it is not otherwise considered as
a participant in this process44. Recent studies have shown
NRP1 that patients with an overlap syndrome characterized
by arteriovenous malformations and telangiectases har-
VEGFR EPHB4 EPHB2 boured mutations in BMP9, which further implicates this
EPHB2 factor in the formation of arteriovenous malformations45.
MAPK HEY COUP-TF2 Clinical improvements in symptoms have been observed
EPHB4
in patients with hereditary haemorrhagic telangiectasia
ERK Notch PI3K/AKT Notch treated with VEGF signalling inhibitors46,47.
pathway pathway Both endoglin and ALK1 are essential for vascular
development. Systemic inactivation of Eng and Alk1 in
FOXC1/2? MAPK
mice results in arteriovenous malformations and embry-
onic lethality 48,49. Regional or tissue-specific conditional
gene deletion of either Eng or Alk1 only produced arterio
Arterial endothelium Venous endothelium
venous malformations when de novo angiogenesis was
stimulated by VEGF in mice50,51 (FIG. 3a). This finding is
b BMP9* consistent with observations in patients with hereditary
ALK1* haemorrhagic telangiectasia: the tissues most prone to
ENG*
1 2 3 developing telangiectases are those subjected to repeti-
TGFβ tive injury, damage and repair, such as the face, lips and
EPHB4
receptor fingers. This ‘response-to-injury’ hypothesis suggests that
the arteriovenous malformations phenotype includes an
? Gα Gβγ active angiogenic and inflammatory component in addi-
SMAD1/5/8 GNAQ* GDP tion to a genetic predisposition, typically an inherited
RASA1* allele loss of the responsible gene (ENG or ALK1) plus a
SMAD4* GTP later loss of heterozygosity (FIG. 3b).
Nucleus
The capillary malformation–arteriovenous malfor-
GTP GDP
Ras mation syndrome is another genetic syndrome result-
MAPK
ing in cerebral arteriovenous malformations and is
caused by mutations in RASA1 (REF. 52). The ensuing
Nature Reviews
Figure 2 | Molecular mechanism of artery and vein differentiation | Disease Primers
in homeostasis Ras GTPase protein inactivates Ras by hydrolysing GTP
and pathology. a | Several mechanisms have been shown to define the separate arterial to GDP; loss of RASA1 activity, therefore, results in the
and venous phenotypes. Arteries express ephrin receptor B2 (EPHB2), whereas venous excessive activation of Ras and downstream pathways
endothelium expresses its ligand EPHB4. The arterial programme is maintained by
(FIG. 2b). Mechanistically, RASA1 might function down-
activation of the vascular endothelial growth factor (VEGF), neuropilin 1 (NRP1) and the
Notch pathway. Venous endothelial cells that lack NRP1 respond to VEGF with a different stream from EPHB4 in arteriovenous patterning to cause
programme that suppresses Notch signalling and favours EPHB4 expression. The arteriovenous malformation53. Vascular phenotypes in
transcription factor COUP‑TF2 that is expressed in venous endothelial cells suppresses zebrafish morphants were enhanced in the setting of
the arterial programme and favours venous markers. b | Molecular pathways involved in increased mTOR complex 1 (mTORC1) activity, which
arteriovenous malformation syndromes are depicted. (1) Hereditary haemorrhagic might indicate that mTOR inhibition may be a therapeu-
telangiectasia is a syndrome that results from impaired transforming growth factor-β tic approach for capillary malformation–arteriovenous
(TGFβ) signalling. Mutations have been observed in many members of this pathway, malformation syndrome53.
including the ligand bone morphogenetic protein 9 (BMP9), the TGFβ co‑receptors In addition, somatic mutations in GNAQ were found
activin receptor-like kinase 1 (ALK1) and endoglin (ENG), and SMAD signalling molecules. in the vascular malformations taken from patients with
(2) Capillary malformation–arteriovenous malformation syndrome is also associated with
Sturge–Weber syndrome, a condition characterized
arteriovenous malformations. Increased RAS activity due to missense mutations in
RASA1, which encodes a GTPase that might function downstream of EPHB4, are probably by port wine stains on the face and underlying lepto
involved. (3) Malformations associated with Sturge–Weber syndrome result from meningeal angiomatosis54. GNAQ is a G protein α‑subunit
mutations in GNAQ that lead to increased G protein signalling. Vascular malformations involved in mediating signalling from G protein-coupled
have been observed in patients with mutations in each of the genes encoding proteins receptors; mutations in GNAQ decrease GTPase activity
with an asterisk. FOXC, Forkhead box protein C; SHH, Sonic hedgehog. and increase signalling of associated G proteins, leading
4 | 2015 | VOLUME 1 www.nature.com/nrdp
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
a been reported between brain arteriovenous malformations
and genetic variations at chromosome 9p21 (REF. 67), a
genomic locus that is associated with various cardio-
vascular phenotypes, including aortic and intracranial
aneurysms68,69, which might explain the link between
arteriovenous malformations and aneurysms70.
Whether genetic risk factors render individuals more
susceptible to developing arteriovenous malformations
remains to be determined. However, it is well established
that genetic modifiers can influence disease severity, clini
cal course or response to treatment by modulating bio-
logical mechanisms such as inflammation, angiogenesis
b or response to injury 71–73. Predictors of disease course and
Homozygous loss of function Angiogenesis response to therapy would have clinical use, and the need
(response to injury) for biomarkers of haemorrhage risk in both unruptured
and/or untreatable brain arteriovenous malformations is
particularly urgent. Candidate gene studies of sporadic
Somatic endothelial cell Bone-marrow-derived cell
brain arteriovenous malformations have reported com-
mon polymorphisms in interleukin‑6 (IL6)74, IL1B60 and
EPHB4 (REF. 75), which are associated with increased
Initation of AVM haemorrhagic risk. The apolipoprotein E (APOE)
Inflammation Haemodynamic changes
ε2 allele76 and the TNFA‑238G>A allele77 were associ-
ated with increased risk of recurrent rupture, in both
AVM progression untreated78 and treated79 patients. Finally, the Val66Met
variant of brain-derived neurotrophic factor (BDNF),
Figure 3 | Hypotheses of arteriovenous malformationNature pathogenesis
Reviews and the role
| Disease Primers which has been implicated in cerebrovascular disease
of ALK1. a | Images of the brain of a mouse model of brain arteriovenous malformations outcomes, has also been shown to influence the out-
(AVMs) are shown. The mouse model was generated using regional conditional gene comes after resection surgery 80–82. More specifically, this
deletion of activin receptor-like kinase 1 (Alk1) combined with stimulation of variant was associated with worse functional outcomes
angiogenesis via stereotactical injected adeno-associated viral vectors expressing
after resection in patients with unruptured arteriovenous
vascular endothelial growth factor (VEGF). Alk1 was conditionally deleted in the basal
ganglia of the brain by stereotactically delivering adenoviral vector with the gene malformations83. Several lines of evidence, including
expressing Cre recombinase to transgenic mice with Alk1 flanked by loxP sites. Vessel genetic, tissue and imaging studies of arteriovenous
casting shows AVMs in the injected region of the brain of Alk1‑deficient mice (left panel, malformations in patients and animal models, argue that
arrow) with tangled dilated vessels (right panel). b | Hypotheses for AVM pathogenesis inflammation participates in the pathophysiology and
and progression are summarized. Part a adapted with permission from REF. 200, Wiley. clinical course of this condition, possibly in the context
of response-to‑injury mechanisms.
Some of the reported associations are with single-
to increased MAPK activity 54 (FIG. 2b). MAPK expression nucleotide polymorphisms (SNPs) that tag a particular
is suppressed by the PI3K–AKT pathway to promote group of genetic variants in the genome (haplotype-
the venous cell fate, suggesting that this is a possible tagging variants). Although the molecular function of
mechanism for arteriovenous malformations55. most these SNPs remains to be determined, such mark-
ers can still be used as risk predictors. Additional studies
Genetic factors are needed to replicate these associations and identify
Inspired by the genetic component of these specific the functional relevance of these findings in independ-
arteriovenous malformation syndromes, candidate-gene ent cohorts. The future goal of clinical management of
and genome-wide association studies (GWASs) have brain arteriovenous malformations is to develop a pre-
been performed to investigate genetic influences on the diction score for specific clinical courses and therapeutic
more common, sporadically occurring arteriovenous outcomes that will incorporate genotypes of common
malformations. A common non-coding polymorphism polymorphisms alongside epidemiological and morpho-
in ALK1 (ALK1 IVS3‑35A>G) was associated with spora logical risk factors (including type of presentation, size,
dic brain arteriovenous malformations in two independ- location, age, sex and ethnicity). The advent of personal
ent cohorts56–58. Polymorphisms in ENG56, integrin β8 genome sequencing will increase the future availability of
(ITGB8) 59, interleukin‑1β (IL1B) 60, angiop oietin- genotype information for screening and risk assessment.
like 4 (ANGPTL4)61, G protein-coupled receptor 124
(GPR124)62, VEGF63 and matrix metallopeptidase 3 Pathophysiology
(MMP3)64 have also been found to be associated with In addition to the consequences of a rupture of the arterio
this condition. These associations have not yet been repli venous malformation, the presence of an arteriovenous
cated65, and none of the genetic variants linked to the malformation alone can affect the surrounding brain
known familial syndromes has shown strong associations tissue. Perilesional hypoperfusion can, over a period of
with sporadic arteriovenous malformations in the brain, time, lead to the dilation of the perinidal capillary net-
except for the ALK1 variant66. However, an association has work and the recruitment of leptomeningeal collaterals.
NATURE REVIEWS | DISEASE PRIMERS VOLUME 1 | 2015 | 5
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
a Ultrasonography b MRI Cerebral proliferative angiopathy is an extreme
phenotypic variant of classical arteriovenous malforma-
tions. Cerebral proliferative angiopathy occurs in young
adult women and is characterized by seizures. On MRI,
these patients have abnormal vascularity intertwined
with normal brain tissue. There is a discrepancy between
the nidus, which is often diffuse and large in size, and the
relatively normal size of feeding arteries and draining
veins, with only slightly increased transit times. The pres-
ence of gliosis suggests ischaemia in the adjacent brain
tissue, which in turn might induce sprouting angiogenesis
AVM and the recruitment of dural arterial supply to the region.
The natural course of cerebral proliferative angiopathy
c Before embolization d During and after embolization seems to be benign compared with the typical arterio-
PICA venous malformations, but the risk of bleeding increases
feeder after the first rupture. It is important to recognize this
AVM PICA Convexity entity because any type of intervention, including surgery
AVM and radiosurgery, will have increased risk of neurological
AVM Occluded deficits owing to the intervening normal brain tissue87.
AVM
Figure 4 | Prenatal and postnatal diagnosis of an intracranial pial arteriovenous
Nature Reviews | Disease Primers Diagnosis, screening and prevention
fistula. Fetus with a fistulous pial arteriovenous malformation in the brain, diagnosed Age-dependent diagnosis
in utero by the presence of a high-flow shunt on colour-Doppler ultrasonography, is The phenotypical characteristics of brain arteriovenous
shown (part a). The infant presented at birth with severe heart failure. MRI scans show a
malformations differ among age groups and, con
large posterior fossa arteriovenous malformation (AVM; part b, left image) as well as a
smaller sized convexity AVM associated with brain volume loss (part b, right image). sequently, symptoms and diagnostic tools also vary with
Digital subtraction angiography shows the left vertebral artery before embolization. age. In neonates and infants, brain arteriovenous mal-
The posterior fossa AVM is a single artery-to‑vein fistula fed by the posterior inferior formations are rare. Imaging in these patients invariably
cerebellar artery (PICA; part c). The image on the left shows the venous phase, whereas shows evidence of arteriovenous fistulas, which are large
the image on the right shows the arterial phase. After selectively catheterizing the and demonstrate direct communications between arter-
feeding PICA vessel (part d; left image) and embolizing it with coils (part d; right image), ies and veins without an intervening vascular network
the posterior fossa AVM was occluded and the distal basilar circulation was visualized. or nidus (FIG. 4). They can easily be detected by MRI
Notably, the convexity AVM (part d; right image) was filling through the posterior and magnetic resonance angiography (MRA), which
communicating arteries, which are also seen on this angiogram. might also show brain volume loss in the parenchyma
adjacent to the lesion, which is an indication for urgent
The formation of these new blood vessels (in a process treatment 88. CT and CT angiography are performed
termed perinidal angiogenesis) results in a separate net- when haemorrhage is suspected and the precise source
work that is different from the true arteriovenous mal- of bleeding is sought. Catheter angiography by means of
formation nidus84. Similarly, in superficially located digital subtraction angiography is typically performed
malformations, hypoxia can elicit angiogenesis using the at the time of endovascular treatment or in prepara-
dural arteries as a source; thus, a complete arteriovenous tion for surgery. High-flow arteriovenous fistulas might
malformation obliteration must include closure of con- result in systemic symptoms, including congestive heart
tributing arteries from the external carotid system. The failure, and neurological symptoms from arterial steal,
surrounding brain tissue might also be affected by venous regional brain ischaemia, focal neurological deficits and
congestion owing to high input of blood or reduced out- seizures. The presence of multiple arteriovenous fistulas
flow (secondary to stenosis of the draining veins). This should raise the possibility of a hereditary haemorrhagic
pathology can be associated with cognitive decline, epi- telangiectasia disorder 89.
lepsy and neurological deficit85. A long pial course of the In children and young adults, true nidal arteriovenous
draining vein might indicate that normal venous drainage malformations with artery-to‑vein communications
is restricted over a large cortical area, which increases the through an abnormal vascular network occur in addi-
risk of developing seizures85. Conversely, a short vein that tion to the arteriovenous fistulas. Imaging with MRA, CT
drains directly into a dural sinus is unlikely to interfere angiography or digital subtraction angiography shows
with the normal regional drainage and cause seizures, but enlarged feeding arteries and draining veins, as well as
it could result in hydrocephalus and cognitive decline from the intervening nidus.
global venous hypertension and decreased absorption of In adults, nidal arteriovenous malformations are
cerebrospinal fluid86. Patients with venous congestion observed almost exclusively. Diagnosis should include a
might also demonstrate a pseudophlebitic pattern on digi- detailed analysis of both the nidus and the adjacent brain
tal subtraction angiography with an increased number and parenchyma. CT angiography or digital subtraction
calibre of corkscrew-like draining veins remote from the angiography are used to determine the point of rupture
arteriovenous malformations. The interaction between in patients with bleeding, whereas MRI is the preferred
the malformations and the brain is not static but can imaging modality for patients with non-haemorrhagic
change over time in a host- and time-dependent manner85. symptoms. Digital subtraction angiography continues to
6 | 2015 | VOLUME 1 www.nature.com/nrdp
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
be the gold standard for the characterization of the feed- volume with increased mean transit time in the brain
ing arteries, nidus angioarchitecture and draining veins, parenchyma owing to indirect collateral flow to the shunt
and is essential for accurate arteriovenous malformation from adjacent arteries. These patients most commonly
grading and treatment planning 90. present with a focal neurological deficit. The third abnor-
mality is venous congestion, which is characterized by
Imaging techniques increased cerebral blood volume and mean transit time in
CT and related techniques. CT scans are performed in remote parts of the brain due to high-pressure flow in the
patients with suspected intracranial bleeding; when draining veins of the arteriovenous malformation. These
haemorrhage is confirmed, CT angiography is performed patients present with progressive neurological deficits.
to rapidly diagnose the underlying arteriovenous mal-
formations. This technique might also pinpoint the site MRI and related techniques. To screen or electively inves-
of bleeding from feeding artery aneurysms, intranidal tigate the presence of arteriovenous malformations, MRI
aneurysms or venous varices (FIG. 5). Modern CT scan- is the imaging modality of choice because it depicts the
ners can image brain perfusion and show three distinct shunt and assesses perinidal brain parenchyma. MRA
patterns of extranidal parenchymal perfusion abnormali- shows varying degrees of dilatation of the arterial feed-
ties91. The first is functional steal, which is a redirection ers depending on the shunt volume. Flow-induced
of the blood flow from surrounding brain tissue through aneurysms might occur along the feeding arteries. It is
the arteriovenous malformation that disrupts the normal important to look for signs of prior haemorrhage, such
functioning of the brain tissue. It shows on a CT scan as a as signal dephasing on gradient-recalled echo imaging
reduction in cerebral blood flow, cerebral blood volume and perinidal gliosis characterized by an increased signal
and mean transit time due to a sump effect from the artery on T2‑weighted and fluid-attenuated inversion recovery
supplying the arteriovenous malformation. Patients with imaging. Most arteriovenous malformations have minimal
this abnormality commonly present with seizures. The or no mass effect, unless there are large venous pouches
second pattern is termed ischaemic steal and is character- that compress adjacent brain parenchyma and cerebro
ized by decreased cerebral blood flow and cerebral blood spinal fluid drainage pathways. In patients with symptoms
other than haemorrhage, the presence of perinidal brain
oedema is an important finding that is often associated
a b with partial venous outlet thrombosis causing progressive
neurological deficits, headaches and/or seizures. Magnetic
* resonance venography depicts venous outlet obstruction,
venous ectasia and sinus thrombosis. A long pial course of
a draining vein is associated with a higher incidence
of chronic venous ischaemia and seizures90. The absence of
cortical venous drainage in a superficially located brain
c d arteriovenous malformation might indicate thrombosis
* of the superficial outlets with subsequent rerouting into
* the deep system, possibly suggesting a less stable lesion.
Patients with longstanding venous hypertension might
show bilateral, symmetric parenchymal calcifications
within the basal ganglia and subcortical white matter
owing to chronic venous ischaemia.
Angiography. Angiographic analysis of arteriovenous
e f malformation architecture specifically addresses
the nature and number of the feeding arteries, as well
as the presence of flow-related aneurysms. In addition,
angiography can reveal the number of separate compart-
ments within the malformation, any intranidal or peri
nidal arterial aneurysms, and the nature of the venous
drainage, as well as associated varices and stenoses. All
Nature artery
Figure 5 | Imaging of a feeding | Disease Primers
Reviewspseudoaneurysm of these elements are best assessed by digital subtraction
with haemorrhage. An axial CT scan shows angiography. The two basic types of feeding arteries are
intraparenchymal and intraventricular haemorrhage direct arterial feeders, which end in the arteriovenous
(marked by arrowheads; part a). Coronal CT malformation, and indirect arterial feeders, which supply
angiographical image shows the pseudoaneurysm the arteriovenous malformation via small branches that
(part b). Digital subtraction angiography of the vertebral
arise from the involved artery but also continue ‘en pas-
artery shows diagnosis of pseudoaneurysm (asterisks),
seen in anterior-posterior (part c) and lateral (part d) sage’ to normal brain tissue distal to the malformation.
views; selective catheterization of the parent artery Direct feeders might be large cortical arteries or smaller
(part e; arrow); and therapeutic embolization and perforators coursing through white matter or ventri-
occlusion of the pseudoaneurysm, which protect against cles. Flow-related aneurysms along the feeding arteries
future bleedings (part f). are caused by increased shear stress and can indicate
NATURE REVIEWS | DISEASE PRIMERS VOLUME 1 | 2015 | 7
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
Table 2 | Grading systems for brain arteriovenous malformations* 45 years. Surveillance MRI may be less frequent in other
countries. In patients with sporadic arteriovenous mal-
Variables Parameters Points formations managed conservatively, MRI examinations
Spetzler–Martin grading (total score = 5) are recommended every 5 years until the age of 65 years
Size <3 cm 1
to detect silent haemorrhages, unless new symptoms
necessitate an earlier examination94. CT angiography
3–6 cm 2 and digital subtraction angiography have no role in the
>6 cm 3 routine follow‑up care of patients who are clinically
stable. Follow‑up imaging after treatment of a sporadic
Venous Superficial drainage in cortical veins and convexity sinuses 0
drainage arteriovenous malformation is performed to confirm
Deep drainage in the vein of Galen 1 complete obliteration and is essential after embolization
Eloquence No 0 and radiosurgery. This surveillance can also identify the
delayed impact of the treatment, which is particularly
Yes (located in sensorimotor cortex, language areas, 1
visual cortex, hypothalamus, internal capsule, brain stem,
important after radiosurgery. MRI is the optimal initial
cerebellar peduncle or deep cerebellar nuclei) method, but angiography is necessary to confirm com-
plete obliteration. Angiograms at 5‑year intervals are
Lawton–Young grading (total score = 5)
also recommended in paediatric patients after complete
Age <20 years 1 resection of the malformation because of the reported
20–40 years 2 recurrence risks in this population.
>40 years 3
Management
Bleeding Yes 0 Grading and classification
No 1 Grading systems are an important method to describe
arteriovenous malformations. In their efforts to avoid
Compactness Yes 0 surgical complications and poor neurological out-
No 1 comes with microsurgical resection of brain arterio-
*Table reproduced from Kim, H. et al. Validation of the supplemented Spetzler–Martin grading venous malformations, neurosurgeons have identified
system for brain arteriovenous malformations in a multicenter cohort of 1009 surgical patients. factors that determine operative risks and developed
Neurosurgery 76, 25–33 (2015), with permission from Wolters Kluwer Health. criteria that transform complex management decisions
into algorithms. These grading systems have become
more than predictors of surgical risks; they are short-
increased vascular fragility and haemorrhage risk. The hand descriptions of the pathology itself and a part of
aneurysms might resolve following curative treatment the language of brain arteriovenous malformations. The
of the arteriovenous malformation92. Intranidal arterial Spetzler–Martin grading system is the predominant
aneurysms (FIG. 5) represent an angioarchitectural weak classification scheme because it is simple, applicable at
point and are often pseudoaneurysms without a wall and the bedside and accurate. It uses size, eloquence (critical
project into a haematoma. They are usually small (<3 mm) function of surrounding brain parenchyma) and venous
and can be treated by embolization93. The arteriovenous drainage patterns95 (TABLE 2).
malformation nidus can have both fistulous and glomeru Not all factors important to surgical selection and
lar compartments, the former being high-flow shunts outcome are part of the Spetzler–Martin system. Age,
amenable to endovascular therapy and the latter being haemorrhagic presentation and compactness are also
an intervening network of pathological vessels that might critical. Compact arteriovenous malformations with
not be as easy to treat by embolization. Evaluation of the tightly woven arteries and veins have distinct borders
venous portion of the arteriovenous malformation should that separate cleanly from the adjacent brain tissue,
consider the anatomy of drainage (superficial, deep or whereas diffuse malformations have ragged borders and
mixed) and characteristics of the venous outflow, such as are intermixed with brain matter. The Lawton–Young
focal stenosis, venous pouches and associated sinus steno grading system incorporates these other factors (TABLE 2).
sis or occlusion. Drainage into the deep venous system Points are assigned for the ABC’s of arteriovenous mal-
carries a high risk of haemorrhage and indicates deep formations: age, bleeding and compactness. This grading
location that might make surgery difficult. system supplements rather than replaces the traditional
Spetzler–Martin system. The sum of the Spetzler–
Screening and monitoring Martin and Lawton–Young grades, or the supplemented
Evidence supporting the use of imaging to screen and Spetzler–Martin grade, provides clinicians with the
monitor patients with brain arteriovenous malforma- highest predictive accuracy of any grading system and
tions is lacking, even for relatives of patients with spora establishes boundaries for arteriovenous malformation
dic arteriovenous malformations. Screening of patients operability 96–98 (TABLE 3).
and family members suspected of hereditary haemor- In addition, a new classification of arteriovenous mal-
rhagic telangiectasia is performed differently in different formations has been proposed, whereby seven types have
countries, with many North American centres recom- been described depending on their location in the brain:
mending screening with MRI in infancy to be followed by frontal, temporal and parieto-occipital lobes, ventricles,
repeated MRIs at 5‑year intervals at least until the age of deep central core, brainstem and cerebellum99 (TABLE 4).
8 | 2015 | VOLUME 1 www.nature.com/nrdp
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
Table 3 | Neurological outcomes by grade after microsurgical resection* Microsurgery. From a microsurgical perspective, every
arteriovenous malformation can be thoroughly deci-
Worse Improved or unchanged phered and methodically treated in eight steps: exposure,
Grade n Percentage n Percentage subarachnoid dissection, defining the draining vein,
Spetzler–Martin grade
defining the feeding arteries, pial dissection, parenchy-
mal dissection, ependymal or deep dissection, and finally
I 17 7 218 93 resection (FIG. 6). The surgery begins by a craniotomy to
II 80 21 295 79 expose the cortical surface on which the arteriovenous
malformation is based. Craniotomies are large and are
III 84 29 209 71
not considered minimally invasive because some periph-
IV 37 38 61 62 ery is needed to survey the course of feeding arteries and
V 4 50 4 50 draining veins as they travel to and from the arteriovenous
malformations. Furthermore, room is needed to dissect
Supplementary grade
the subarachnoid spaces and accommodate brain shifts.
I 5 6 84 94 Subarachnoid dissection involves surveying the arterio-
II 30 16 161 84 venous malformation under the microscope, and opening
the labyrinth of subarachnoid spaces, and deconstruct-
III 70 18 314 82 ing arachnoid membranes, disconnecting interlobular
IV 92 32 196 68 trabeculae and intercommunicating cisternal compart-
V 25 44 32 56
ments. Subarachnoid dissection is a translation of angio-
graphical anatomy onto the surgical field, and abnormal
Supplemented Spetzler–Martin grade feeding arteries and distorted draining veins are inspected
2 0 0 24 100 for clues to their angiographical identity.
The most important feature underlying successful
3 1 2 59 98
arteriovenous malformation surgery is that the draining
4 21 10 182 90 vein must be preserved until the very end of the resection.
5 54 19 237 81 Although placing efferent veins at the centre of dissection
strategy might seem counterintuitive in the presence of
6 56 24 176 76
ferocious arterial afferents, intraoperative ruptures occur
7 54 39 84 61 when outflow is obstructed, leading to increased intra-
8 30 63 18 38 nidal pressure and distension of the malformation, fol-
lowed by rupture and bleeding in the surgical field. No
9 6 55 5 45 predefined strategy to manage the bleeding for arterio
10 0 0 2 100 venous malformation ruptures exists as for aneurysm
*Table reproduced from Kim, H. et al. Validation of the supplemented Spetzler–Martin grading rupture. Tamponade or holding pressure is ineffective for
system for brain arteriovenous malformations in a multicenter cohort of 1009 surgical patients. managing bleeding because there are multiple bleeding
Neurosurgery 76, 25–33 (2015), with permission from Wolters Kluwer Health. sites, suction might not clear the field and afferent arter-
ies are too numerous to control quickly or completely.
Preservation of the efferent vein is, therefore, of utmost
Within each type, the brain surface on which the arterio importance during surgery. In addition, the vein guides
venous malformation is based (for example, lateral, the dissection to the nidus. Indeed, one-third of malfor-
medial or basal) or other specific anatomical regions mations are beneath the cortical surface and two-thirds
(such as midbrain, pons and medulla) further categor have superficial venous drainage, which means that many
ize them in 4–6 subtypes. Using this classification, the only have an arterialized vein on the surface. Draining
range of brain arteriovenous malformations is simplified veins also visually illustrate the progress of the resection
to a finite number of different subtypes, each character- as their colour changes from red to purple to blue as the
ized by its own arterial supply, draining veins, eloquent dissection proceeds.
structures, surgical approach and management strategy. Another important principle is that arteries are occlu
Categorization helps to guide management, facilitate ded as close as possible to their point of contact with the
learning and sharpen the language of brain arteriovenous arteriovenous malformation. More proximal occlusion
malformations encountered in practice99. can sacrifice normal branches and might lead to infarcts
in the adjacent brain tissue. However, more distal occlu-
Treatment sion can elicit bleeding from the nidus or preserve proxi-
Patients with brain arteriovenous malformations are mal feeding branches. Several types of afferent arteries
managed by non-interventional follow‑up (conserva- are found proximal to the arteriovenous malformations:
tive management) or invasive treatment. Currently, no terminal or direct feeding artery; transit or indirect artery;
drugs are available to treat arteriovenous malforma- perforating artery; choroidal artery; and bystander artery
tions or to prevent haemorrhage, but the associated that does not supply the arteriovenous malformation. Each
seizures can be managed with anticonvulsant medica- arteriovenous malformation has its unique set of arterial
tions and recurrent headaches with preventive or acute feeders that determine its ‘fingerprint’; complete closure
symptomatic treatment. of these arterial feeders is central to successful treatment.
NATURE REVIEWS | DISEASE PRIMERS VOLUME 1 | 2015 | 9
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
Dissection of the pia mater of the brain is directed involved brain tissue — must be respected by maintain-
at feeding arteries on the cortical surfaces, also called ing a close distance to the arteriovenous malformation.
arterial fronts, where these superficial inputs intersect Parenchymal dissection detaches the arteriovenous
the arteriovenous malformations. During this surgi- malformation from the brain and comprises two-
cal step, eloquence — or functional importance of the thirds of the circumdissection. Every converging artery
supplying the arteriovenous malformation is closed and
secondary draining veins are trimmed. Most arterio
Table 4 | Classification and prevalence of brain AVMs* venous malformations are compact, have distinct
Type n Percentage‡ margins and are easily separated from adjacent brain
tissue, all of which facilitate parenchymal dissection.
Frontal AVMs §
A diffuse arteriovenous malformation, however, is
Lateral frontal 48 8 wound loosely, as if unravelled, with indistinct margins,
Medial frontal 21 4 intermixed brain and poor separability. They are diffi-
Paramedian frontal 24 4 cult to dissect and force the neurosurgeon to establish
Basal frontal 21 4 the plane of separation between the malformation and
brain. The interplay of eloquence and haemostasis pull
Sylvian frontal 21 4
in and push back the circumdissection, and challenge
Temporal AVMs|| the neurosurgeon to find the right dissection distance.
Lateral temporal 76 13 Finally, ependymal dissection takes place at the
Basal temporal 12 2 tip of the classical arteriovenous malformation cone,
which is tapered to the ependyma. Ependymal dissec-
Medial temporal 17 3
tion might be a confusing term because many arterio-
Sylvian temporal 7 1 venous malformations do not reach a ventricle, but it
Parieto-occipital AVMs ¶
describes the deep dissection that comes at the end of
Lateral parieto-occipital 52 9 the surgery. This dissection is diametrically opposed
Medial parieto-occipital 17 3 to the neurosurgeon and is inherently difficult to see
because it is physically blocked by the malformation
Paramedian parieto-occipital 29 5
nidus. This plane receives perforating and choroidal
Basal occipital 10 2 artery supply, which can be difficult to coagulate. The
(Peri)ventricular AVMs# arteriovenous malformation can be resected when the
Callosal 23 4 sides of the malformation have all been circumferen-
Ventricular body 5 1 tially dissected, the arterial supply is disconnected and
the draining vein turns blue. Expected outcomes after
Atrial 9 2
microsurgical resection in patients with favourable
Temporal horn 5 1 grades are generally excellent 95,100–109 (TABLE 5).
Deep AVMs**
Pure Sylvian 8 1 Embolization. Endovascular management of arterio
Insular 25 4 venous malformations varies with a patient’s age. It has
a major role in the treatment of neonates and infants
Basal ganglial 10 2
with arteriovenous fistulas and major cardiac symptoms
Thalamic 13 2 or progressive brain ischaemia, who require immediate
Brainstem AVMs‡‡ intervention. The transarterial closure with polymeric
Anterior midbrain 1 0 glue is the most efficient method in this age group88. In
Posterior midbrain 6 1
addition, treatment at centres with experienced teams
and skilled experts equipped to handle the complexities
Anterior pontine 6 1
of care is highly recommended. In children and young
Lateral pontine 7 1 adults, endovascular management is typically performed
Anterior medullary 1 0 as an adjunct to microsurgery because these individuals
Lateral medullary 5 1 more frequently present with bleeding than older adults
and often require life-saving removal of the haematoma.
Cerebellar AVMs §§
Preoperative embolization aims to obliterate the bleeding
Suboccipital cerebellar 18 3 source, such as a pseudoaneurysm, and/or to eliminate
Tentorial cerebellar 16 3 deep feeding arteries that might not be surgically accessi-
Vermian cerebellar 25 4 ble until late in the dissection. In a small and select group
Tonsillar cerebellar 7 1 of adults, embolization can be performed as a curative
intervention. However, curing brain arteriovenous mal-
Petrosal cerebellar 16 3
formations solely by endovascular means might only be
Mixed AVMs 39 7 possible in approximately 20% of malformations, particu-
*Types of brain arteriovenous malformations (AVMs) identified during surgery of 600 patients. larly those that are small, and have a single direct feeder
‡
Percentage of patients identified with a specific subtype. §23%. ||19%. ¶18%; #7%. **9%; ‡‡4%;
§§
14%. Table adapted from Table p.1 Lawton, Michael T.: Seven AVM’s Tenets and Techniques for and a single compartment110. Palliative embolization aims
Resection, with permission from Thieme Medical Publishers. to eliminate the largest fistulas in the malformations and
10 | 2015 | VOLUME 1 www.nature.com/nrdp
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
a b traditional glue (20–40%)111–113 but is also associated with
Draining vein
increased complication risks. Indeed, the rate of perma-
nent neurological deficit and death is 8–15% with Onyx
versus 3–7% with glue114. Embolization with both types
of liquid embolic materials is safe through direct arterial
feeders, as long as the catheter tip is positioned beyond
AVM an artery supplying normal brain tissue and potential
reflux of embolic material, which might block such arter-
ies, is avoided. Indirect or ‘en passage’ feeding arteries
1 are considered to be unsafe because embolic material will
Feeding artery migrate to distal arteries88. Arteriovenous fistulas and fis-
c d
tulous communications in arteriovenous malformations
PreFrA PreFrA are best treated by transarterial injection of glue (FIG. 7).
Frontal A drawback of the use of glue is the potential propaga-
lobe 3 tion of glue into veins, which might subsequently lead
to secondary venous occlusion and increased haemor-
rhage risk. Coils might be safer to use in these fistulous
AVM AVM
PreCenA subtypes. In some cases, coils can also be used to reduce
flow before glue embolization. Small- and medium-sized
Draining 2 arteriovenous malformations with multiple arterial feed-
Draining
vein PreCenA ers have an improved chance of cure with Onyx emboli-
vein
zation, but with the understanding that such cure may be
e f associated with manifest complication risk.
Draining vein
When arteriovenous malformations are associated
with aneurysms, the symptomatic lesion is always treated
AVM 4 first, even when embolization is the method of treatment.
In an analysis of 662 patients with brain arteriovenous
AVM
malformations, 305 patients had associated aneu-
PreCenA rysms, and the incidence of rebleeding was significantly
increased in those harbouring intranidal aneurysms
Draining
(P < 0.002)115. In another series of 678 patients with brain
PreFrA vein arteriovenous malformations, the presence of associated
aneurysms raised the annual risk of future bleeding from
Nature Reviews
Figure 6 | Resection strategy of arteriovenous malformations. | Disease Primers
a | Angiogram 3.9% per year (without aneurysms) to 6.9% (with associ
(carotid artery dye injection, lateral view) of an arteriovenous malformation (AVM; ated aneurysms) (P = 0.01)116. Thus, these associated
supplemented Spetzler–Martin Grade 6) is shown. b | To conduct microsurgical aneurysms require attention, and endovascular therapy
resection of the AVM, (1) an orbital-pterional craniotomy was performed (dashed line). is considered when it lies beyond the surgical field. The
c | The surgeon sees the arterial inputs from the precentral artery (PreCenA) and the role of embolization therapy will continue to increase as
prefrontal artery (PreFrA), both branches from the middle cerebral artery, the AVM and newer embolic agents and delivery systems are devel-
the draining vein. d | A schematic representation of the photograph in part c is shown. oped that have improved obliteration rates and fewer
Surgery continues by identifying (2) the draining veins and (3) the cortical arterial associated complications.
feeders. e | Schematic representation of the AVM in part c as seen in a coronal
cross-sectional slice through the frontal lobes is shown. Next, (4) the inferior front of
arteries near the middle frontal gyrus is interrupted, taking care to preserve en passage
Radiosurgery. Stereotactic radiosurgery involves the
flow in transit arteries. Finally, the frontal parenchyma is circumdissected, and the AVM precise, image-guided delivery of a radiation dose to a
is mobilized to expose lenticulostriate artery feeders on the inferior side. f | After defined target. The aim is to close the lumen of an involved
complete circumdissection, the AVM darkened. vessel and to obliterate the arteriovenous malformation.
Stereotactic radiosurgery has become an increasingly
attractive option for patients with arteriovenous malfor-
is performed in patients presenting with progressive mations, as it can produce excellent results with a modest
neurological deficits or seizures, and it can result in risk117–124. The main risks of stereotactic radiosurgery are
stabilization or improvement of clinical symptoms. twofold. First, a latency period exists before maximum
The techniques and approaches used for emboli- obliteration after the procedure, in which haemorrhage
zation therapy are highly variable and include differ- risk remains and obliteration can typically take up to
ent agents and devices, such as n‑butyl cyanoacrylate 4 years. Second, the process can affect or damage adja-
(NBCA) glue, liquid embolic agents (such as Onyx, cent neural structures, leading to neurological morbidity.
Covidien, USA) and coils, and a variety of approaches These adverse radiation effects are typically inflamma-
including transarterial, transvenous or combinations tory but can also be haemodynamic125. Complete oblit-
thereof. The transarterial route is the most frequently eration rates vary between 50% and 90% depending on
used approach and liquid glue is the classic embolic the arteriovenous malformation volume117,119,126–130. Once
agent. Onyx is a newer liquid agent with very different complete obliteration is confirmed by angiography, the
properties; it has higher obliteration rates (40–80%) than lesion can be considered cured with <1% remaining
NATURE REVIEWS | DISEASE PRIMERS VOLUME 1 | 2015 | 11
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
Table 5 | Summary of microsurgical results in patients with low-grade arteriovenous malformations
Study Year n Morbidity (%) Mortality (%) Cure rate (%) Haemorrhage (%)
Spetzler, Martin 95
1986 44 2.3 0 NA NA
Heros103 1990 47 2.2 2.2 100 0
Sundt 109
1991 84 2.2 0 100 0
Sisti, Stein108 1993 67 1.5 0 94 0
Hamilton, Spetzler 101
1994 40 0.0 0 100 NA
Schaller, Schramm106 1997 50 3.2 0 98 2
Schaller, Schramm107 1998 81 0.0 0 NA NA
Harbaugh105 1998 26 3.8 0 100 0
Hartmann102 2000 48 6.6 0 NA NA
Morgan104 2004 220 0.9 0.5 100 0
Davidson, Morgan 100
2010 296 0.7 0 97 NA
Lawton110 2015 232 2.4 0.5 98 0
Total – 1,235 2.2 0.3 98.5 0.3
NA, not analysed.
risk of subsequent haemorrhage127. Successful oblitera- radiosurgical devices; a higher central dose might lead to
tion after stereotactic radiosurgery depends directly on a better obliteration response when using selective confor-
the amount of radiation delivered and on the accurate mal radiotherapy140,152. If post-radiosurgery adverse effects
identification of the arteriovenous malformation shunt. occur, several medical strategies can be used to treat the
The morbidity of stereotactic radiosurgery is a function effects. Such strategies include the use of corticosteroids,
of the radiation dose and the total volume treated. Blood vitamin E, pentoxifylline (a phosphodiesterase inhibitor)
flow in the arteriovenous malformation might also cor- and bevacizumab153 (a VEGF inhibitor); anticoagulation
relate with the obliterative response, but to date this has or hyperbaric oxygen are rarely used.
been difficult to measure and study. As such, a balance Complex and large arteriovenous malformations that
must be struck between maintaining efficacy of the are not suitable for resection might be considered for
treatment and minimizing risk127,131–141. endovascular embolization followed by stereotactic radio
Preclinical and human clinical data have been used surgery. The goal of embolization is to reduce the volume
to create both dose–response and dose–complication of the malformation and to facilitate radiosurgery119,154–171.
curves. The goal was to achieve a low permanent risk However, sometimes embolization reduces the blood
of injury to the adjacent brain tissue. The lower doses flow rather than the volume, which might not facilitate
needed to achieve this risk inevitably lead to lower radiosurgery. Indeed, some authors report that emboli-
obliteration rates, especially in large-volume arterio- zation before stereotactic radiosurgery can lead to worse
venous malformations. However, a number of new con- overall outcomes. Multiple case series have shown that
cepts have been proposed to overcome the biological stereotactic radiosurgery obliteration rates for patients
drawbacks of low doses142,143, including staged volume who receive prior embolization are significantly lower
or staged dose approaches144–146. With volume-staged than those who are not embolized112,129,161,172–179. This
radiosurgery, large malformations are divided into finding might, however, be an artefact of patient selec-
smaller portions and treated separately with safe doses tion. Some hypothesize that embolic agents can act as
in multiple sessions, as if each portion was an indivi radioprotectants, others hypothesize that embolization
dual malformation. With dose-staged radiosurgery, large promotes angiogenesis or that dose planning becomes
malformations are treated with hypofractionated stereo- more difficult as the nidus becomes less well defined172,180.
tactic radiosurgery or with repeat radiosurgery months Because of this evidence, one option would be to consider
or years later if there is no evidence of obliteration. embolization following radiosurgery. In addition, because
Arteriovenous malformations targeting is dependent arteriovenous malformations might have associated
on high-resolution imaging (FIG. 8). Typically, this includes aneurysms that constitute an additional risk of haemor
both stereotactic volumetric axial plane imaging (usually rhage, one should consider repairing the aneurysm by
MRI or CT) in conjunction with digital subtraction angio microsurgical or endovascular means. However, a flow-
graphy 147–151. The imaging is used to identify the nidus or related aneurysm might regress spontaneously follow-
arteriovenous shunt. Quantification of blood flow might ing closure of the arteriovenous malformation. Another
assist nidus definition but this is not yet readily avail- consideration is to resect part of the irradiated arterio-
able. Once the target is defined, a margin dose is selected venous malformation that did not completely obliterate
(a range of 16–25 Gy in a single procedure is common; angiographically. Arteriovenous malformations that are
obliteration rates seem to drop at doses below 16 Gy). more amenable to resection have little vascularity and
A margin isodose line of 50–80% is used with most are easily accessible.
12 | 2015 | VOLUME 1 www.nature.com/nrdp
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
Multimodal approach. Treatment of arteriovenous mal- Recurrence is rare, but young patients with deep venous
formations often consists of a multimodal approach that drainage are at increased risk182. Patients with residual
includes microsurgical resection, endovascular emboli- arteriovenous malformations undergo re‑operation for
zation and stereotactic radiosurgery, either alone or in complete resection if feasible and safe. Patients who
combination176. The aim is to target the vessels involved receive a deliberate incomplete resection are considered
in the arteriovenous malformation from all sides: resec- for radiosurgery as part of triple modality therapy.
tion on the outside, embolization on the inside and When patients are poor surgical candidates (supple-
radiosurgery to the vessel wall. A multidisciplinary mented Spetzler–Martin grade >6 points), radiosurgery
team will determine which approach might be opti- is performed. Small- and medium-sized arteriovenous
mal for a given patient. The primary goal of treatment malformations are treated with conventional stereotactic
is complete arteriovenous malformations obliteration, radiosurgery and large malformations are treated with
thereby completely eliminating any risk of rupture10. If volume-staged radiosurgery, both without emboliza-
lesions are only partially treated, patients remain at risk. tion. Patients are monitored for 3 years and those with
That is, non-curative treatment of arteriovenous mal- incompletely obliterated arteriovenous malformations
formations, independent of approach, exposes patients are reconsidered for microsurgery 183. Criteria evalu-
to treatment risks but does not lower or eliminate the ated in the arteriovenous malformations grading scale
haemorrhage risk22,116,181. might have changed in the meantime, particularly size,
The development of management plans is chal- haemorrhage status and diffuseness, which possibly
lenging owing to the variety of ways that embolization, downgrades a malformation and renders a patient newly
microsurgery and radiosurgery can be used alone or in eligible for microsurgery. In such cases, embolization is
combination. Typically, microsurgery is favoured as it considered as a preoperative adjunct.
has superior cure rates and acceptable rates of associ- In addition, many candidates for microsurgery can
ated morbidity and mortality. The Spetzler–Martin and also be candidates for radiosurgery, in which case radio-
Lawton–Young grading systems provide rapid, bed- surgery is considered a viable alternative. Analyses to
side assessments, and a supplemented Spetzler–Martin compare microsurgical and radiosurgical treatment
grade ≤6 points makes microsurgery a viable option98. alternatives enable comparison of risks, advantages and
If patients would further benefit from embolization disadvantages, with particular emphasis on technical
and if the risk is acceptable, double modality therapy is differences, surgical morbidity, radiosurgical morbidity,
appropriate. If the risk of embolization is too high — for haemorrhage risk during the latency period and relative
example, due to a haematoma or elevated intracranial efficacies of therapy.
pressure — only microsurgery should be performed. Conservative observation involves close monitoring
After microsurgical treatment, an angiography is per- of potential aneurysms on feeding arteries, both intra-
formed to determine the adequacy of resection. Only nidally and in the circle of Willis. Aneurysms ≥7 mm
complete angiographical obliteration is considered cura- in diameter that are associated with high-flow arterio-
tive or protective against future haemorrhage22,116,181. venous malformations or with dysplastic morphology
need to be treated. Untreated aneurysms are monitored
Before surgery 3 years after surgery Transarterial glue injection with serial imaging and are only treated if they enlarge.
a b c d
Evidence from clinical studies
Anteroposterior view
Many studies have confirmed that microsurgery is
superior in treating low-grade arteriovenous malforma-
tions (Spetzler–Martin grade I and II) compared with no
treatment, embolization or radiosurgery 184. In a study
conducted to assess the outcome of surgical treatment
at the University of California, San Francisco, USA,
232 patients were selected with a mean age of 38 years,
Lawton–Young grades of ≤III (69% of patients) and few
(<4%) arteriovenous malformations in deep locations.
Lateral view
Embolization was used as a preoperative adjunct in just
43% of patients and did not result in complications.
Postoperative angiography confirmed that all patients
were cured by the surgical intervention. 78% of all
patients and 91% of patients with unruptured arterio
venous malformations experienced good outcomes
Figure 7 | Arteriovenous malformation occlusion through Nature radiosurgery andPrimers
Reviews | Disease (mRS (modified Rankin Scale) scores 0–1). These sur-
transarterial glue embolization. Carotid angiograms show a left parietal
gical results are consistent with other reports in the lit-
arteriovenous malformation (AVM) fed mainly by one large middle cerebral artery feeder
(marked by arrows; part a). The patient was treated with Gamma Knife radiosurgery,
erature. For example, in a review of 1,235 patients with
which failed to obliterate this fistulous AVM, seen on carotid angiograms 3 years later low-grade arteriovenous malformations, the average sur-
(part b). The malformation was cured with transarterial glue injection, as seen on the skull gical morbidity and mortality rates were 2.2% and 0.3%,
X‑rays showing the cast of glue (part c) and carotid angiograms with no further filling of respectively, with an average cure rate of 98.5% and a
the malformation (part d). postoperative or delayed haemorrhage rate of 0.3%110.
NATURE REVIEWS | DISEASE PRIMERS VOLUME 1 | 2015 | 13
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
a surgery still offers the best cure rate, lowest risk profile
and greatest protection against haemorrhage for low-
AVM AVM
grade arteriovenous malformations. Surgery cannot
compete with the minimally invasive appeal of these
other modalities, but this issue remains secondary to
functional outcome.
Controversy arose following a 2014 randomized con-
trolled clinical trial showing that interventional therapy
* increased the risk of stroke or death in patients with
*
arteriovenous malformations compared with medical
treatment. The randomized trial of unruptured brain
b arteriovenous malformations (ARUBA) 13 involved
223 patients and was designed to compare pharmacologi-
cal therapy for neurological symptoms (as needed; control
group) with an interventional group of patients under-
going neurosurgical, endovascular or radiotherapy pro-
cedures (alone or in combination; experimental group).
Unexpectedly, the trial showed that the control group had
better outcomes than those assigned to interventional
therapy, with stroke and death rates of 10.1% and 30.7%,
Figure 8 | Tectal arteriovenous malformations treated with Gamma
Nature | Disease Primers
Reviews Knife respectively 13. A planned interim analysis even showed
stereotactic radiosurgery. a | Targeting is based on digital subtraction angiography, that the risk of death and symptomatic stroke was 73%
which visualizes the basilar artery (marked by an asterisk), the feeding arteries and nidus lower for patients allocated to non-intervention com-
(arrows). b | MRI is also used to increase precision. Yellow and green lines around the pared with the experimental group (HR in the popula-
arteriovenous malformation (AVM) mark the isodose lines, which are contoured to limit tion as randomized 0.27; 95% CI: 0.14–0.54; HR in the
radiation to surrounding brain structures. population as actually treated 0.19; 95% CI: 0.09–0.38). In
addition, the risk of neurological impairment (mRS ≥2)
The management of arteriovenous malformations decreased by 60% after 12 months (relative risk (RR) 0.4;
outside the United States is diverging from the micro 95%: CI 0.1–0.8) and by 80% after 2 years (RR 0.2; 95% CI
surgical approach. In some European countries, for 0.1–0.6) for the non-interventional group compared with
example, treatment is often limited to ruptured arterio- the interventional group. Similar results were reported in
venous malformations and involves aggressive emboli- a 12‑year prospective observational study in a Scottish
zation, frequently adding radiosurgery when the latter cohort of unruptured brain arteriovenous malforma-
was incomplete. However, cure rates with Onyx embo- tions24. In this study, the risk of stroke and neurological
lization are still low and are associated with increased deficits remained 63% lower for unruptured brain arterio-
complications, such as the occlusion of critical draining venous malformations managed conservatively (HR: 0.37;
veins and adverse imaging findings, such as ischaemia 95% CI: 0.19–0.72) compared with surgical intervention24.
or infarctions, in as many as 40% of patients. In a review Despite its evident results, the ARUBA study received
of 1,297 patients with mostly low-grade arteriovenous profound criticism. Defenders of the trial results argue
malformations, the average endovascular morbidity and that patients enrolled were representative of population-
mortality rates were 6.2% and 1.6%, respectively, with based cohorts, that arteriovenous malformations had
an average cure rate of only 29% and a postoperative or profiles favouring treatment (62% being <3 cm in dia
delayed haemorrhage rate of 8.0%. These figures show meter), that an interim analysis only provides an interim
that aggressive embolization has higher procedural distribution of treatment modalities, and that the study
risks, lower cure rates and increased haemorrhage risks was not powered to evaluate neurosurgical outcome
compared with microsurgery. alone185. However, the study had a number of weaknesses.
Radiosurgery also ranks below microsurgery in the First, a considerable number of neurosurgical investiga-
management protocol of low-grade arteriovenous mal- tors did not consider arteriovenous malformations with
formations. Although these lesions are ideal for radio- low Spetzler–Martin grades (low treatment risk) to be in
surgery because of their lower target volumes and higher equipoise with observational management alone owing
obliteration rates, the 2–3 year latency period between to the high haemorrhage risk and treated the patients
treatments and obliteration opens the possibility for regardless, thereby excluding these patients from enrol-
haemorrhage and associated complications. Radiation- ment. Furthermore, patients with intermediate- and
induced complications are low, but in a review of 1,051 high-grade arteriovenous malformations that are gen-
patients with low-grade arteriovenous malformations, erally considered to have a benign natural history, but
7.2% of patients haemorrhaged after treatment, result- are at high risk for any treatment, were included in the
ing in morbidity and mortality rates of 6.5% and 1.2%, trial, which might have diminished the interventional
respectively 110. The 75.2% cure rate for radiosurgery was results186. Second, with its bias towards non-surgical
superior to the cure rate for endovascular interventions therapy, the number of incompletely obliterated arterio
but was still lower than microsurgery. Thus, despite the venous malformations that remained after treatment
advances in endovascular and radiosurgical therapy, was probably substantial and resulted in ruptures during
14 | 2015 | VOLUME 1 www.nature.com/nrdp
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
the study period. Thus, the adverse events in the inter- reflects a neurological deficit that interferes with usual
ventional group reflected the procedural morbidity activities but not with self-care, progressing to mRS of 6,
of the therapies during the trial compounded with the death. More detailed health-related quality of life instru-
delayed morbidity of latent haemorrhages associated with ments, such as the SF‑36 and EuroQoL187, have been
radiosurgery and incomplete embolization in the past. established in arteriovenous malformation research as
The outcomes of such a group with many incompletely part of the ARUBA trial protocol, and their widespread
treated malformations could never be superior to those use would be desirable even though the complexity of
of an observational group whose only morbidity was the their administration might negatively influence com-
natural history risk. Third, non-surgical preferences in pliance of patients and clinicians. The little evidence
the ARUBA trial are apparent. Two-thirds of patients that exists suggests that following microsurgery, a mRS
in the interventional group had low-grade, surgical score <2 correlates with good neuropsychological and
arteriovenous malformations and yet only 18% under- psychosocial outcomes188.
went surgery, whereas 32% were treated with emboliza- For arteriovenous malformations presenting without
tion alone, 33% with radiosurgery alone and 16% with haemorrhage and managed conservatively, approxi-
a combination of both. Thus, the threefold increase in mately 98% and 80–90% will remain haemorrhage-free
death or stroke in the interventional group potentially after 12 months and 10 years, respectively. Following
reflects the risks associated with embolization and radio- rupture, 96% and 65% will remain haemorrhage-free
surgery therapies, rather than microsurgery. Indeed, the after 12 months and 10 years, respectively, when left
rates of stroke and death in this trial do not match other untreated12,14,189,190 (FIG. 9). The risk of subsequent bleeding
reported surgical outcomes. In addition, centres were further increases in the presence of ruptured-associated
required to manage ten patients with arteriovenous mal- aneurysms, deep location, exclusively deep venous drain-
formations per year, but there were no minimum require- age and increasing patient age12,15,17,191. However, initial
ments for neurosurgeons; arteriovenous malformation haemorrhage remains the strongest predictor 12,14, and
resection is among the most challenging neurosurgical some of the additional factors might be biased by dif-
cases, and high-volume surgeons typically perform ferential censoring owing to differences in the degree
>25 resections annually. of surgical difficulty (deep venous drainage is likely to
These critiques were validated in an analysis of be managed conservatively) or long-term benefit (older
ARUBA-eligible patients managed outside the trial. As patients are likely to be managed conservatively). Some
a participating ARUBA site, the University of California, prospective population data suggest the 12‑month case-
San Francisco, screened 473 patients for eligibility but fatality after haemorrhage is 12% overall, with increasing
enrolled only 4 patients in the trial; 74 eligible patients patient age and initial haematoma volume as independent
were managed outside the trial. Of these 74 patients, predictors21. In arteriovenous malformations diagnosed
43 patients (71% of treated patients) were treated surgi- unruptured, the 12‑year risk of death was not different
cally, 15 patients (25% of treated patients) were treated for conservatively managed patients compared with those
radiosurgically and 13 patients (18% overall) were with intervention (adjusted HR: 1.62; 95% CI: 0.72–
observed. The risk of stroke and death among treated 3.65)24. Several studies showed that clinical outcome after
patients was lower than in ARUBA, with primary out- rupture is better than after hypertension-related haemor
come rates of 11%, 27% and 8% for surgery, radiosurgery rhage, independent of patient age and other known
and observation, respectively. The threefold difference in predictors of intracerebral haemorrhage outcome21,192.
primary outcome reported in ARUBA disappeared with In addition to haemorrhage, health-related quality
a different management strategy and a different surgical of life might be affected by seizures, neurological defi-
expertise, leaving no significant difference in the rate of cits unrelated to seizure (that is, hemiparesis and homo
stroke or death between treated and observed patients. nymous haemianopia) and headaches. Generalized
Thus, results in ARUBA-eligible patients managed out- seizures unrelated to haemorrhage occur in 30% of
side that trial led to an entirely different conclusion about patients with arteriovenous malformations; focal seizures
intervention in arteriovenous malformations manage- occur in 10%6. For patients with seizures, the 5‑year
ment, owing to the primary role of surgery, judicious chance of achieving a seizure-free period of 2 years with
surgical selection with established outcome predictors antiepileptic drugs is 40–80%, but the success is indepen
and technical expertise developed at a high-volume dent of interventional therapy 25,193,194. Neurological defi-
arteriovenous malformation centre184. cits can also be caused by alterations in regional brain
blood flow, which are caused by the variable interaction
Quality of life between regional pressure reduction in arteries and eleva-
Although health-related quality of life measures are tion in veins, and they can be progressive (4–6% of new
increasingly used as part of neurological treatment trials arteriovenous malformations), persistent (6–9% of
and large observational studies, scant data are available in new cases) or transient (6–10% of new cases)6. Headaches
relation to the management of arteriovenous malforma- unrelated to haemorrhage occur in 12–16% of patients6.
tions. The most prevalent outcome scale used to reflect The headache types can vary and include migraine,
neurological impairment in neurovascular research is the tension-type headaches and other subtypes. In cases
mRS, which is scored from 0 to 6, where a mRS score of 0 of migraine, the arteriovenous malformation usually
is normal, mRS of 1 reflects symptoms without physi has an external carotid supply and is more commonly
cal deficit or interference with usual activities, mRS of 2 located posteriorly 6.
NATURE REVIEWS | DISEASE PRIMERS VOLUME 1 | 2015 | 15
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
70 areas95,97. Endovascular results have also improved over
time, perhaps even more dramatically. Onyx represents
Cumulative risk of rupture (%)
60 Kim et al. (2014) Previously ruptured
Gross et al. (2014) AVMs a quantum leap in liquid embolysates over polyvinyl
50 alcohol (PVA) and NBCA glue. The higher viscosity of
40 Onyx enables it to slowly reach draining veins, its non-
adherence causes less catheter retention and its slow
30 Unruptured AVMs solidification deepens nidal penetration. Advances in
20 liquid embolysates are anticipated to increase penetra-
tion and durability over time. Improved microcatheters
10 are also expected, such as one with a detachable break
0 away tip for more aggressive embolization with reduced
0 5 10 15 20 complications from retained catheters. Transvenous
Years approaches to embolization have been introduced for
Figure 9 | Hypothetical cumulative risk of rupture in patients
Nature with| arteriovenous
Reviews Disease Primers some arteriovenous malformations (small, deep, unrup-
malformations. The graph shows the cumulative risks of ruptures of arteriovenous tured and refractory to radiosurgical obliteration). They
malformations (AVMs) with and without a previous haemorrhage. Percentage include navigating against flow into the nidus by way
cumulative risk of rupture was calculated as (1 – e−annual rate × years) × 100. Kim et al.12
of its dilated draining veins and using systemic hypo-
reported a 4.8% risk of rupture for previously ruptured AVMs and a 1.3% risk for tension or balloon occlusion of large feeding arteries to
unruptured AVMs, respectively, whereas Gross et al.196 reported a 4.5% and 2.2% of reduce antegrade flow through the nidus. This technique
risk for previously ruptured and unruptured AVMs, respectively. carries a risk of perforating the draining vein, premature
occlusion and intraprocedural haemorrhage, making it
Although living with an untreated brain arterio- an experimental technique that remains to be proven.
venous malformation carries the potential risks cited However, it exemplifies the type of innovation that is
above, treatment can also be associated with manifest possible with endovascular techniques. Improvements
adverse effects. A systematic meta-analysis incorporat- in endovascular management will hopefully decrease
ing 13,698 patients with arteriovenous malformations its complication rate and increase its cure rate, and
including 46,314 patient-years of follow‑up data suggest will make it a competitive, less invasive alternative to
that interventional therapy remains associated with con- open microsurgery.
siderable risks and incomplete efficacy. Severe complica-
tion and complete obliteration rates of 6.6% and 13%, Advances in drug development
respectively, were associated with endovascular therapy; Drug development for the pharmacological manage-
rates of 5.1% and 38%, respectively, were associated with ment of arteriovenous malformations has been slower
stereotactic radiosurgery; and rates of 7.4% and 96%, than advances in the surgical and endovascular arenas.
respectively, were associated with microsurgery 195. To date, there are no specific or approved therapies;
Another consideration relates to the risk of haemor- however, drug development has been envisioned in
rhage during pregnancy. Some retrospective cohort case several forms, including preventing the formation of
series suggest an increased rate of haemorrhage, lead- arteriovenous malformations, inducing obliteration
ing to recommendations of arteriovenous malforma- and stabilizing vessels to reduce rupture risk199. These
tion obliteration before pregnancy, avoidance of vaginal therapies depend on improved understanding of the the
delivery or pregnancy avoidance8,196. However, other underlying mechanisms of arteriovenous malforma-
reports suggest no increased risk of arteriovenous mal- tion development. Walker et al.200 recently developed
formation rupture during pregnancy 19,197,198. Thus, this the first credible adult mouse model of arteriovenous
issue remains controversial and we do not recommend malformations using angiogenic stimulation with
deviation from normal obstetric practice. VEGF in combination with conditional deletion of Alk1
to induce severe vascular dysplasia with arteriovenous
Outlook shunting in a nidus-like lesion in the brain (FIG. 3a).
Advances in surgical techniques A similar model with conditional deletion of Eng also
The management of brain arteriovenous malformations produced an arteriovenous lesion in the mouse brain
continues to evolve with advances in microsurgical, mimicking an arteriovenous malformation. These
radiosurgical and endovascular techniques and tech- developments validate the genetic mechanisms respon-
nology. Microsurgical results have improved over time sible for the formation of arteriovenous malformations
with the creation of newer grading systems to select in patients with hereditary haemorrhagic telangiectasia
patients likely to experience optimal outcomes. Other and also have implications for sporadic arteriovenous
improvements include the following: the development malformations. Furthermore, these models support the
of instruments such as bipolar forceps and microclips response-to-injury hypothesis and, importantly, provide
that coagulate or occlude feeding arteries effectively; the an experimental system for testing new pharmacological
recognition of arteriovenous malformation subtypes that interventions. For example, VEGFR1 (encoded by FLT1)
help to decipher the anatomy of the malformation; the has anti-angiogenic properties. Expression of soluble
refinement of surgical approaches, strategies and dissec- VEGFR1 has been shown to abolish VEGF-induced
tion techniques that facilitate safe resection; and the use angiogenesis and the formation of arteriovenous mal-
of functional MRI to better identify and protect eloquent formations in mice, suggesting a novel treatment.
16 | 2015 | VOLUME 1 www.nature.com/nrdp
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
Similarly, bevacizumab has been demonstrated to pre- and prostate. Now, the identification of molecular and
vent or halt the progression of both cutaneous and brain genetic pathways for cancer has shifted focus to the geno
arteriovenous malformations in animal models200,201. typical causes. Any single genetic signature or signalling
Tetracycline and doxycycline inhibit matrix metallo- pathway in cancer can be relevant for multiple organ-
proteinases, which might stabilize arteriovenous mal- specific cancer phenotypes. For example, activated muta-
formations and reduce vascular degradation202,203. These tions in GNAQ were first described in uveal melanoma
common antibiotics are taken up in malformations and but have been observed in multiple additional tumour
might provide some reduction in haemorrhage risk in types206–208, and now also in Sturge–Weber syndrome54.
patients whose arteriovenous malformations are man- As research advances our understanding of the
aged conservatively. These experimental studies remain pathophysiology of arteriovenous malformations, grad-
in their infancy and have yet to progress to clinical trials, ing systems must evolve and incorporate these advances,
but they signal that translational research is advancing such as genetic information and biological markers.
for the first time. Genetic studies and the discovery of Haemodynamic data might also become a defining ele-
genes involved in sporadic arteriovenous malformations ment of rupture risk and future grading scales. Thus,
might offer additional insight into their biology and the work of developing new grading systems should be
inform the the design of future therapies that obliterate, viewed as an ongoing process that will refine and reshape
stabilize or regress the malformations. existing grading systems.
Optimization of classification criteria Advances in clinical studies
Although the Spetzler–Martin grading scale is well Finally, it will be important for investigators to continue
established to evaluate the risks of microsurgery, it to perform robust clinical studies and randomized trials
is not a relevant predictor of the risks associated with to further refine indications for treatment. The ARUBA
embolization or radiosurgery. These observations have trial and the controversy surrounding it has reminded
led to the development of endovascular and radio- the community of its obligation to continue question-
surgical grading systems204,205. Interventional grading ing best practices. For example, some critics of the
systems need individualized predictors of the natural ARUBA trial have suggested that another trial is needed
history of arteriovenous malformations. The current to re‑establish the role of surgery in management called
grading systems are generally useful but are imperfect BARBADOS (Beyond ARUBA — Randomized low-
and evolving. grade Brain AVM stuDy, Observation versus Surgery)209.
In addition, mutations in arteriovenous malforma- Other critics have begun organizing prospective regis-
tions and other vascular malformations might have tries of patients with arteriovenous malformations for
overlapping genetic signatures, and these canonical detailed outcome analyses. The future of arteriovenous
molecular pathways may be relevant to several types malformation research, whether at the bench or bed-
of vascular malformations. Analogously, the oncology side, will depend on well-defined and objective efforts
field initially focused on phenotypical descriptions of to better understand and manage this fascinating disease
cancers in the organs of origin such as the breast, lungs and prevent its potentially devastating complications.
1. Morris, Z. et al. Incidental findings on brain magnetic A study of haemorrhage rates associated with 15. Hernesniemi, J. A. et al. Natural history of brain
resonance imaging: systematic review and untreated arteriovenous malformations in a arteriovenous malformations: a long-term follow‑up
meta‑analysis. BMJ 339, b3016 (2009). controlled population in Finland, establishing study of risk of hemorrhage in 238 patients.
2. Stapf, C. et al. The New York Islands AVM Study: some of the best natural history data on Neurosurgery 63, 823–829; discussion 829–831
design, study progress, and initial results. Stroke 34, this condition. (2008).
e29–e33 (2003). 10. Englot, D. J. et al. Seizure predictors and control after 16. Kim, H. et al. Racial/ethnic differences in longitudinal
3. Stapf, C. et al. Incidence of adult brain arteriovenous microsurgical resection of supratentorial arteriovenous risk of intracranial hemorrhage in brain arteriovenous
malformation hemorrhage in a prospective malformations in 440 patients. Neurosurgery 71, malformation patients. Stroke 38, 2430–2437 (2007).
population‑based stroke survey. Cerebrovasc. Dis. 13, 572–580; discussion 580 (2012). 17. Stapf, C. et al. Predictors of hemorrhage in patients
43–46 (2002). 11. Fults, D. & Kelly, D. L. Jr. Natural history of with untreated brain arteriovenous malformation.
4. Al‑Shahi, R. et al. Prospective, population-based arteriovenous malformations of the brain: a clinical Neurology 66, 1350–1355 (2006).
detection of intracranial vascular malformations study. Neurosurgery 15, 658–662 (1984). This study showed that arteriovenous
in adults: the Scottish Intracranial Vascular 12. Kim, H., Al‑Shahi Salman, R., McCulloch, C. E., malformations in deep locations, with deep venous
Malformation Study (SIVMS). Stroke 34, 1163–1169 Stapf, C. & Young, W. L. Untreated brain arteriovenous drainage and presenting with previous
(2003). malformation: patient-level meta-analysis of haemorrhage could have rupture rates as high
5. Gabriel, R. A. et al. Ten-year detection rate of brain hemorrhage predictors. Neurology 83, 590–597 as 35% per year.
arteriovenous malformations in a large, multiethnic, (2014). 18. Guo, Y. et al. Silent intralesional microhemorrhage
defined population. Stroke 41, 21–26 (2010). This paper combined four separate cohorts to as a risk factor for brain arteriovenous malformation
6. Hofmeister, C. et al. Demographic, morphological, show that increasing age and presentation with rupture. Stroke 43, 1240–1246 (2012).
and clinical characteristics of 1289 patients with brain bleeding were predictors of arteriovenous 19. Liu, X. J. et al. Risk of cerebral arteriovenous
arteriovenous malformation. Stroke 31, 1307–1310 malformation haemorrhage. malformation rupture during pregnancy and
(2000). 13. Mohr, J. P. et al. Medical management with or without puerperium. Neurology 82, 1798–1803 (2014).
7. ApSimon, H. T., Reef, H., Phadke, R. V. & Popovic, E. A. interventional therapy for unruptured brain 20. van Beijnum, J. et al. Prevalence of brain arteriovenous
A population-based study of brain arteriovenous arteriovenous malformations (ARUBA): a multicentre, malformations in first-degree relatives of patients with
malformation: long-term treatment outcomes. Stroke non-blinded, randomised trial. Lancet 383, 614–621 a brain arteriovenous malformation. Stroke 45,
33, 2794–2800 (2002). (2014). 3231–3235 (2014).
8. Crawford, P. M., West, C. R., Chadwick, D. W. & This randomized clinical trial compared various 21. van Beijnum, J. et al. Outcome after spontaneous and
Shaw, M. D. Arteriovenous malformations of the brain: therapeutic interventions to medical management arteriovenous malformation-related intracerebral
natural history in unoperated patients. J. Neurol. and its results have stirred worldwide debate about haemorrhage: population-based studies. Brain 132,
Neurosurg. Psychiatry 49, 1–10 (1986). arteriovenous malformation management. 537–543 (2009).
9. Ondra, S. L., Troupp, H., George, E. D. & Schwab, K. 14. Halim, A. X. et al. Longitudinal risk of intracranial 22. Laakso, A. et al. Long-term excess mortality in
The natural history of symptomatic arteriovenous hemorrhage in patients with arteriovenous 623 patients with brain arteriovenous malformations.
malformations of the brain: a 24‑year follow‑up malformation of the brain within a defined population. Neurosurgery 63, 244–253; discussion 253–255
assessment. J. Neurosurg. 73, 387–391 (1990). Stroke 35, 1697–1702 (2004). (2008).
NATURE REVIEWS | DISEASE PRIMERS VOLUME 1 | 2015 | 17
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
23. Wedderburn, C. J. et al. Outcome after interventional 45. Wooderchak-Donahue, W. L. et al. BMP9 mutations J. Neurol. Neurosurg. Psychiatry 84, 1059–1062
or conservative management of unruptured brain cause a vascular-anomaly syndrome with phenotypic (2013).
arteriovenous malformations: a prospective, overlap with hereditary hemorrhagic telangiectasia. 68. Holdt, L. M. & Teupser, D. Recent studies of the
population-based cohort study. Lancet Neurol. 7, Am. J. Hum. Genet. 93, 530–537 (2013). human chromosome 9p21 locus, which is associated
223–230 (2008). 46. Dupuis-Girod, S. et al. Bevacizumab in patients with with atherosclerosis in human populations.
24. Al‑Shahi Salman, R. et al. Outcome after conservative hereditary hemorrhagic telangiectasia and severe Arterioscler. Thromb. Vasc. Biol. 32, 196–206
management or intervention for unruptured brain hepatic vascular malformations and high cardiac (2012).
arteriovenous malformations. JAMA 311, 1661–1669 output. JAMA 307, 948–955 (2012). 69. Helgadottir, A. et al. The same sequence variant on
(2014). 47. Flieger, D., Hainke, S. & Fischbach, W. Dramatic 9p21 associates with myocardial infarction, abdominal
This study of a cohort in Scotland corroborated improvement in hereditary hemorrhagic telangiectasia aortic aneurysm and intracranial aneurysm.
findings from the ARUBA trial, adding to the after treatment with the vascular endothelial growth Nat. Genet. 40, 217–224 (2008).
controversy relating to the management of factor (VEGF) antagonist bevacizumab. Ann. Hematol. 70. Bendjilali, N. et al. Genetic variants on 9p21.3 are
arteriovenous malformation. 85, 631–632 (2006). associated with brain arteriovenous malformations
25. Josephson, C. B. et al. Seizure risk with AVM treatment 48. Sorensen, L. K., Brooke, B. S., Li, D. Y. & Urness, L. D. with associated arterial aneurysms. Stroke 44,
or conservative management: prospective, population- Loss of distinct arterial and venous boundaries in mice abstr. TMP30 (2013).
based study. Neurology 79, 500–507 (2012). lacking endoglin, a vascular-specific TGFβ coreceptor. 71. Emond, M. J. et al. Exome sequencing of extreme
26. Lawton, M. T., Jacobowitz, R. & Spetzler, R. F. Dev. Biol. 261, 235–250 (2003). phenotypes identifies DCTN4 as a modifier of chronic
Redefined role of angiogenesis in the pathogenesis of 49. Urness, L. D., Sorensen, L. K. & Li, D. Y. Arteriovenous Pseudomonas aeruginosa infection in cystic fibrosis.
dural arteriovenous malformations. J. Neurosurg. 87, malformations in mice lacking activin receptor-like Nat. Genet. 44, 886–889 (2012).
267–274 (1997). kinase‑1. Nat. Genet. 26, 328–331 (2000). 72. Wright, F. A. et al. Genome-wide association and
27. Risau, W. Mechanisms of angiogenesis. Nature 386, 50. Park, S. O. et al. Real-time imaging of de novo linkage identify modifier loci of lung disease severity in
671–674 (1997). arteriovenous malformation in a mouse model of cystic fibrosis at 11p13 and 20q13.2. Nat. Genet. 43,
28. Kume, T. Specification of arterial, venous, and lymphatic hereditary hemorrhagic telangiectasia. J. Clin. Invest. 539–546 (2011).
endothelial cells during embryonic development. 119, 3487–3496 (2009). 73. Drumm, M. L. et al. Genetic modifiers of lung disease
Histol. Histopathol. 25, 637–646 (2010). 51. Garrido-Martin, E. M. et al. Common and distinctive in cystic fibrosis. N. Engl. J. Med. 353, 1443–1453
29. Gerety, S. S. & Anderson, D. J. Cardiovascular pathogenetic features of arteriovenous malformations (2005).
ephrinB2 function is essential for embryonic in hereditary hemorrhagic telangiectasia 1 and 74. Pawlikowska, L. et al. Polymorphisms in genes
angiogenesis. Development 129, 1397–1410 (2002). hereditary hemorrhagic telangiectasia 2 animal involved in inflammatory and angiogenic pathways
30. Swift, M. R. & Weinstein, B. M. Arterial-venous models — brief report. Arterioscler. Thromb. Vasc. and the risk of hemorrhagic presentation of brain
specification during development. Circ. Res. 104, Biol. 34, 2232–2236 (2014). arteriovenous malformations. Stroke 35, 2294–2300
576–588 (2009). 52. Boon, L. M., Mulliken, J. B. & Vikkula, M. RASA1: (2004).
31. Mukouyama, Y. S., Shin, D., Britsch, S., Taniguchi, M. variable phenotype with capillary and arteriovenous 75. Weinsheimer, S. et al. EPHB4 gene polymorphisms
& Anderson, D. J. Sensory nerves determine the malformations. Curr. Opin. Genet. Dev. 15, 265–269 and risk of intracranial hemorrhage in patients with
pattern of arterial differentiation and blood vessel (2005). brain arteriovenous malformations. Circ. Cardiovasc.
branching in the skin. Cell 109, 693–705 (2002). 53. Kawasaki, J. et al. RASA1 functions in EPHB4 Genet. 2, 476–482 (2009).
32. Moyon, D., Pardanaud, L., Yuan, L., Breant, C. signaling pathway to suppress endothelial mTORC1 76. Pawlikowska, L. et al. Apoliprotein E epsilon2 is
& Eichmann, A. Plasticity of endothelial cells during activity. J. Clin. Invest. 124, 2774–2784 (2014). associated with new hemorrhage risk in brain
arterial-venous differentiation in the avian embryo. 54. Shirley, M. D. et al. Sturge–Weber syndrome and arteriovenous malformation. Neurosurgery 58,
Development 128, 3359–3370 (2001). port‑wine stains caused by somatic mutation in GNAQ. 838–843; discussion 838–843 (2006).
33. Sorensen, I., Adams, R. H. & Gossler, A. N. Engl. J. Med. 368, 1971–1979 (2013). 77. Achrol, A. S. et al. TNFα‑238G>A promoter
DLL1‑mediated Notch activation regulates endothelial 55. Hong, C. C., Peterson, Q. P., Hong, J. Y. & polymorphism is associated with increased risk of new
identity in mouse fetal arteries. Blood 113, Peterson, R. T. Artery/vein specification is governed hemorrhage in the natural course of patients with
5680–5688 (2009). by opposing phosphatidylinositol‑3 kinase and MAP brain arteriovenous malformations. J. Neurosurg.
34. Lawson, N. D., Vogel, A. M. & Weinstein, B. M. sonic kinase/ERK signaling. Curr. Biol. 16, 1366–1372 Anesthesiol. 17, 217–218 (2005).
hedgehog and vascular endothelial growth factor act (2006). 78. Sturiale, C. L. et al. Single nucleotide polymorphisms
upstream of the Notch pathway during arterial 56. Pawlikowska, L. et al. Polymorphisms in transforming associated with sporadic brain arteriovenous
endothelial differentiation. Dev. Cell 3, 127–136 growth factor-B‑related genes ALK1 and ENG are malformations: where do we stand? Brain 136,
(2002). associated with sporadic brain arteriovenous 665–681 (2013).
35. Hayashi, H. & Kume, T. Foxc transcription factors malformations. Stroke 36, 2278–2280 (2005). 79. Achrol, A. S. et al. Association of tumor necrosis
directly regulate Dll4 and Hey2 expression by 57. Young, W. L. et al. Arteriovenous malformation. factor-α‑238G>A and Apolipoprotein E2
interacting with the VEGF–Notch signaling pathways J. Neurosurg. 106, 731–732 (2007). polymorphisms with intracranial hemorrhage after
in endothelial cells. PLoS ONE 3, e2401 (2008). 58. Simon, M. et al. Association of a polymorphism brain arteriovenous malformation treatment.
36. Shoemaker, L. D. et al. Human brain arteriovenous of the ACVRL1 gene with sporadic arteriovenous Neurosurgery 61, 731–739; discussion 740 (2007).
malformations express lymphatic-associated genes. malformations of the central nervous system. 80. McAllister, T. et al. Polymorphisms in the brain derived
Ann. Clin. Transl. Neurol. 1, 982–995 (2014). J. Neurosurg. 104, 945–949 (2006). neurotrophic factor (BDNF) gene influence memory
37. You, L. R. et al. Suppression of Notch signalling by the 59. Su, H. et al. Reduced expression of integrin αvβ8 is and processing speed one month after brain injury.
COUP-TFII transcription factor regulates vein identity. associated with brain arteriovenous malformation J. Neurotrauma 29, 1111–1118 (2012).
Nature 435, 98–104 (2005). pathogenesis. Am. J. Pathol. 176, 1018–1027 81. Qin, L., Kim, E., Ratan, R., Lee, F. S. & Cho, S. Genetic
38. Faughnan, M. E. et al. International guidelines for the (2010). variant of BDNF (Val66Met) polymorphism attenuates
diagnosis and management of hereditary haemorrhagic 60. Kim, H. et al. Common variants in interleukin‑1‑β gene stroke-induced angiogenic responses by enhancing
telangiectasia. J. Med. Genet. 48, 73–87 (2011). are associated with intracranial hemorrhage and anti-angiogenic mediator CD36 expression.
39. McAllister, K. A. et al. Endoglin, a TGF-β susceptibility to brain arteriovenous malformation. J. Neurosci. 31, 775–783 (2011).
bindinG protein of endothelial cells, is the gene Cerebrovasc. Dis. 27, 176–182 (2009). 82. Siironen, J. et al. The Met allele of the BDNF
for hereditary haemorrhagic telangiectasia type 1. 61. Mikhak, B. et al. Angiopoietin-like 4 (ANGPTL4) gene Val66Met polymorphism predicts poor outcome
Nat. Genet. 8, 345–351 (1994). polymorphisms and risk of brain arteriovenous among survivors of aneurysmal subarachnoid
This paper describes the genetic basis of malformations. Cerebrovasc. Dis. 31, 338–345 hemorrhage. Stroke 38, 2858–2860 (2007).
arteriovenous malformations in hereditary (2011). 83. Westbroek, E. M. et al. Brain-derived neurotrophic
haemorrhagic telangiectasia. 62. Weinsheimer, S. et al. G protein-coupled receptor 124 factor Val66Met polymorphism predicts worse
40. Johnson, D. W. et al. Mutations in the activin (GPR124) gene polymorphisms and risk of brain functional outcome after surgery patients with
receptor‑like kinase 1 gene in hereditary haemorrhagic arteriovenous malformation. Transl. Stroke Res. 3, unruptured brain arteriovenous malformation. Stroke
telangiectasia type 2. Nat. Genet. 13, 189–195 418–427 (2012). 43, 2255–2257 (2012).
(1996). 63. Chen, H. et al. Polymorphisms of the vascular 84. Sato, S., Kodama, N., Sasaki, T., Matsumoto, M.
This manuscript established the genetic basis endothelial growth factor A gene and susceptibility to & Ishikawa, T. Perinidal dilated capillary networks in
for arteriovenous malformations in hereditary sporadic brain arteriovenous malformation in a cerebral arteriovenous malformations. Neurosurgery
haemorrhagic telangiectasia and guided the Chinese population. J. Clin. Neurosci. 18, 549–553 54, 163–168; discussion 168–170 (2004).
development of animal models. (2011). 85. Shankar, J. J. et al. Angioarchitecture of brain AVM
41. Govani, F. S. & Shovlin, C. L. Hereditary haemorrhagic 64. Zhao, Y. et al. The rs522616 polymorphism in determines the presentation with seizures: proposed
telangiectasia: a clinical and scientific review. the matrix metalloproteinase‑3 (MMP‑3) gene is scoring system. AJNR Am. J. Neuroradiol. 34,
Eur. J. Hum. Genet. 17, 860–871 (2009). associated with sporadic brain arteriovenous 1028–1034 (2013).
42. Gallione, C. J. et al. A combined syndrome of juvenile malformation in a Chinese population. J. Clin. 86. Geibprasert, S. et al. Hydrocephalus in unruptured
polyposis and hereditary haemorrhagic telangiectasia Neurosci. 17, 1568–1572 (2010). brain arteriovenous malformations: pathomechanical
associated with mutations in MADH4 (SMAD4). Lancet 65. Weinsheimer, S. et al. Genome-wide association study considerations, therapeutic implications, and clinical
363, 852–859 (2004). of brain arteriovenous malformation patients. Stroke course. J. Neurosurg. 110, 500–507 (2009).
43. David, L., Mallet, C., Mazerbourg, S., Feige, J. J. 42, abstr. #W MP85 (2011). 87. Lasjaunias, P. L. et al. Cerebral proliferative
& Bailly, S. Identification of BMP9 and BMP10 as 66. Weinsheimer, S. et al. Common polymorphisms in angiopathy: clinical and angiographic description
functional activators of the orphan activin receptor-like familial vascular malformation genes do not show of an entity different from cerebral AVMs. Stroke 39,
kinase 1 (ALK1) in endothelial cells. Blood 109, association with sporadic brain arteriovenous 878–885 (2008).
1953–1961 (2007). malformation. Stroke 43, abstr. A3666 (2012). 88. Krings, T., Geibprasert, S. & Terbrugge, K.
44. David, L. et al. Bone morphogenetic protein‑9 is a 67. Sturiale, C. L. et al. Association between the Classification and endovascular management of
circulating vascular quiescence factor. Circ. Res. 102, rs1333040 polymorphism on the chromosomal 9p21 pediatric cerebral vascular malformations.
914–922 (2008). locus and sporadic brain arteriovenous malformations. Neurosurg. Clin. N. Am. 21, 463–482 (2010).
18 | 2015 | VOLUME 1 www.nature.com/nrdp
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
89. Bharatha, A. et al. Brain arteriovenous malformation 108. Sisti, M. B., Kader, A. & Stein, B. M. Microsurgery for 130. Shin, M. et al. Analysis of nidus obliteration rates after
multiplicity predicts the diagnosis of hereditary 67 intracranial arteriovenous malformations less than Gamma Knife surgery for arteriovenous malformations
hemorrhagic telangiectasia: quantitative assessment. 3 cm in diameter. J. Neurosurg. 79, 653–660 (1993). based on long-term follow‑up data: the University of
Stroke 43, 72–78 (2012). 109. Sundt, T. M. Jr, Piepgras, D. G. & Stevens, L. N. Tokyo experience. J. Neurosurg. 101, 18–24 (2004).
90. Geibprasert, S. et al. Radiologic assessment of brain Surgery for supratentorial arteriovenous 131. Aoyama, H. et al. Treatment outcome of single or
arteriovenous malformations: what clinicians need to malformations. Clin. Neurosurg. 37, 49–115 (1991). hypofractionated single-isocentric stereotactic
know. Radiographics 30, 483–501 (2010). 110. Potts, M. B. et al. Current surgical results with low- irradiation (STI) using a linear accelerator for
This article summarizes the imaging features of brain grade brain arteriovenous malformations. intracranial arteriovenous malformation.
arteriovenous malformations. J. Neurosurg. 122, 912–920 (2015). Radiother. Oncol. 59, 323–328 (2001).
91. Kim, D. J. & Krings, T. Whole-brain perfusion CT patterns This article summarizes current opinion on 132. Hadjipanayis, C. G. et al. Stereotactic radiosurgery
of brain arteriovenous malformations: a pilot study in the role of surgery in the treatment of brain for motor cortex region arteriovenous malformations.
18 patients. AJNR Am. J. Neuroradiol. 32, 2061–2066 arteriovenous malformations. Neurosurgery 48, 70–76; discussion 76–77 (2001).
(2011). 111. Valavanis, A. & Yasargil, M. G. The endovascular 133. Nakamura, J. L. et al. Dose conformity of Gamma
92. Redekop, G., TerBrugge, K., Montanera, W. & treatment of brain arteriovenous malformations. Knife radiosurgery and risk factors for complications.
Willinsky, R. Arterial aneurysms associated with cerebral Adv. Tech. Stand. Neurosurg. 24, 131–214 (1998). Int. J. Radiat. Oncol. Biol. Phys. 51, 1313–1319
arteriovenous malformations: classification, incidence, 112. Yu, S. C., Chan, M. S., Lam, J. M., Tam, P. H. & (2001).
and risk of hemorrhage. J. Neurosurg. 89, 539–546 Poon, W. S. Complete obliteration of intracranial 134. Levegrun, S., Hof, H., Essig, M., Schlegel, W.
(1998). arteriovenous malformation with endovascular & Debus, J. Radiation-induced changes of brain tissue
93. Krings, T., Hans, F. J., Geibprasert, S. & Terbrugge, K. cyanoacrylate embolization: initial success and rate after radiosurgery in patients with arteriovenous
Partial “targeted” embolisation of brain arteriovenous of permanent cure. AJNR Am. J. Neuroradiol. 25, malformations: dose/volume-response relations.
malformations. Eur. Radiol. 20, 2723–2731 (2010). 1139–1143 (2004). Strahlenther. Onkol. 180, 758–767 (2004).
94. Abla, A. A. et al. Silent arteriovenous malformation 113. Katsaridis, V., Papagiannaki, C. & Aimar, E. Curative 135. Pollock, B. E., Gorman, D. A. & Brown, P. D.
hemorrhage and the recognition of “unruptured” embolization of cerebral arteriovenous malformations Radiosurgery for arteriovenous malformations of the
arteriovenous malformation patients who benefit (AVMs) with Onyx in 101 patients. Neuroradiology 50, basal ganglia, thalamus, and brainstem. J. Neurosurg.
from surgical intervention. Neurosurgery 76, 592–600 589–597 (2008). 100, 210–214 (2004).
(2015). 114. Taylor, C. L. et al. Complications of preoperative 136. Inoue, H. K. Long-term results of gamma knife surgery
95. Spetzler, R. F. & Martin, N. A. A proposed grading embolization of cerebral arteriovenous malformations. for arteriovenous malformations: 10- to 15‑year follow
system for arteriovenous malformations. J. Neurosurg. J. Neurosurg. 100, 810–812 (2004). up in patients treated with lower doses. J. Neurosurg.
65, 476–483 (1986). 115. Meisel, H. J. et al. Effect of partial targeted N‑butyl- 105 (Suppl.), 64–68 (2006).
The grading system proposed in this paper has cyano-acrylate embolization in brain AVM. 137. Sirin, S. et al. Prospective staged volume radiosurgery
become an established predictor of risk associated Acta Neurochir. 144, 879–887; discussion 888 (2002). for large arteriovenous malformations: indications and
with brain surgery to eliminate arteriovenous 116. da Costa, L. et al. The natural history and predictive outcomes in otherwise untreatable patients.
malformations. The paper also describes the features of hemorrhage from brain arteriovenous Neurosurgery 58, 17–27; discussion 17–27 (2006).
anatomy of brain arteriovenous malformations. malformations. Stroke 40, 100–105 (2009). 138. Liscak, R. et al. Arteriovenous malformations after
96. Kim, H. et al. Evaluating performance of the Spetzler– 117. Karlsson, B., Lindquist, C. & Steiner, L. Prediction of Leksell Gamma Knife radiosurgery: rate of obliteration
Martin supplemented model in selecting patients with obliteration after Gamma Knife surgery for cerebral and complications. Neurosurgery 60, 1005–1014;
brain arteriovenous malformation for surgery. Stroke arteriovenous malformations. Neurosurgery 40, discussion 1015–1016 (2007).
43, 2497–2499 (2012). 425–430; discussion 430–431 (1997). 139. Ganz, J. C., Reda, W. A. & Abdelkarim, K. Adverse
97. Lawton, M. T., Kim, H., McCulloch, C. E., Mikhak, B. & 118. Kemeny, A. A., Dias, P. S. & Forster, D. M. Results radiation effects after Gamma Knife surgery in relation
Young, W. L. A supplementary grading scale for selecting of stereotactic radiosurgery of arteriovenous to dose and volume. Acta Neurochir.151, 9–19
patients with brain arteriovenous malformations for malformations: an analysis of 52 cases. J. Neurol. (2009).
surgery. Neurosurgery 66, 702–713; discussion 713 Neurosurg. Psychiatry 52, 554–558 (1989). 140. Lunsford, L. D., Niranjan, A., Kano, H. & Kondziolka, D.
(2010). 119. Lunsford, L. D. et al. Stereotactic radiosurgery The technical evolution of Gamma Knife radiosurgery
The grading system proposed in this paper increased for arteriovenous malformations of the brain. for arteriovenous malformations. Prog. Neurol. Surg.
the predictive accuracy of the Spetzler–Martin J. Neurosurg. 75, 512–524 (1991). 27, 22–34 (2013).
grading system and has become an important tool 120. Dwenger, A., Funck, M., Lueken, B., Schweitzer, G. 141. Huang, P. P. et al. Long-term outcomes after staged-
for selecting patients for surgery. & Lehmann, U. Effect of ascorbic acid on neutrophil volume stereotactic radiosurgery for large
98. Kim, H. et al. Validation of the supplemented Spetzler– functions and hypoxanthine/xanthine oxidase- arteriovenous malformations. Neurosurgery 71,
Martin grading system for brain arteriovenous generated, oxygen-derived radicals. Eur. J. Clin. Chem. 632–643; discussion 643–644 (2012).
malformations in a multicenter cohort of 1009 surgical Clin. Biochem. 30, 187–191 (1992). 142. Barker, F. G. et al. Dose-volume prediction of radiation-
patients. Neurosurgery 76, 25–33 (2015). 121. Steiner, L. et al. Clinical outcome of radiosurgery for related complications after proton beam radiosurgery
This study validated the Lawton–Young grading cerebral arteriovenous malformations. J. Neurosurg. for cerebral arteriovenous malformations.
system in a multicentre cohort of more than 1,000 77, 1–8 (1992). J. Neurosurg. 99, 254–263 (2003).
patients, demonstrating that methods to select 122. Yamamoto, M., Jimbo, M., Hara, M., Saito, I. & 143. Kjellberg, R. N., Hanamura, T., Davis, K. R., Lyons, S. L.
patients for surgery are evolving and improving. Mori, K. Gamma Knife radiosurgery for arteriovenous & Adams, R. D. Bragg-peak proton-beam therapy
99. Lawton, M. Seven AVMs: Tenets and Techniques for malformations: long-term follow‑up results focusing for arteriovenous malformations of the brain. N. Engl.
Resection. xiii–xiv (Thieme Medical Publishers, 2014). on complications occurring more than 5 years after J. Med. 309, 269–274 (1983).
100. Davidson, A. S. & Morgan, M. K. How safe is irradiation. Neurosurgery 38, 906–914 (1996). 144. Pollock, B. E., Kondziolka, D., Lunsford, L. D.,
arteriovenous malformation surgery? A prospective, 123. Yamamoto, M. et al. Long-term follow‑up of Bissonette, D. & Flickinger, J. C. Repeat stereotactic
observational study of surgery as first-line treatment for radiosurgically treated arteriovenous malformations radiosurgery of arteriovenous malformations: factors
brain arteriovenous malformations. Neurosurgery 66, in children: report of nine cases. Surg. Neurol. 38, associated with incomplete obliteration. Neurosurgery
498–504; discussion 504–505 (2010). 95–100 (1992). 38, 318–324 (1996).
101. Hamilton, M. G. & Spetzler, R. F. The prospective 124. Yamamoto, M. et al. Long-term results of radiosurgery 145. Flickinger, J. C. An integrated logistic formula
application of a grading system for arteriovenous for arteriovenous malformation: neurodiagnostic for prediction of complications from radiosurgery.
malformations. Neurosurgery 34, 2–6; discussion 6–7 imaging and histological studies of angiographically Int. J. Radiat. Oncol. Biol. Phys. 17, 879–885 (1989).
(1994). confirmed nidus obliteration. Surg. Neurol. 37, 146. Kano, H. et al. Stereotactic radiosurgery for
102. Hartmann, A. et al. Determinants of neurological 219–230 (1992). arteriovenous malformations, Part 6: multistaged
outcome after surgery for brain arteriovenous 125. Monaco, E. A. et al. Management of adverse radiation volumetric management of large arteriovenous
malformation. Stroke 31, 2361–2364 (2000). effects after radiosurgery for arteriovenous malformations. J. Neurosurg. 116, 54–65 (2012).
103. Heros, R. C., Korosue, K. & Diebold, P. M. Surgical malformations. Prog. Neurol. Surg. 27, 107–118 147. Zhang, X. Q. et al. Clinical significance of 3D
excision of cerebral arteriovenous malformations: late (2013). reconstruction of arteriovenous malformation using
results. Neurosurgery 26, 570–577; discussion 126. Kano, H. et al. Stereotactic radiosurgery for digital subtraction angiography and its modification
577–578 (1990). arteriovenous malformations, Part 3: outcome with CT information in stereotactic radiosurgery. Int. J.
104. Morgan, M. K., Rochford, A. M., Tsahtsarlis, A., Little, N. predictors and risks after repeat radiosurgery. Radiat. Oncol. Biol. Phys. 57, 1392–1399 (2003).
& Faulder, K. C. Surgical risks associated with the J. Neurosurg. 116, 21–32 (2012). 148. Maitz, A. H. et al. Tube angulation improves
management of grade I and II brain arteriovenous 127. Kano, H. et al. Stereotactic radiosurgery for angiographic targeting of arteriovenous malformations
malformations. Neurosurgery 54, 832–837; discussion arteriovenous malformations, Part 1: management during stereotactic radiosurgery. Comput. Aided Surg.
837–839 (2004). of Spetzler–Martin grade I and II arteriovenous 6, 225–229 (2001).
105. Pikus, H. J., Beach, M. L. & Harbaugh, R. E. malformations. J. Neurosurg. 116, 11–20 (2012). 149. Bednarz, G., Downes, B., Werner-Wasik, M.
Microsurgical treatment of arteriovenous malformations: 128. Plasencia, A. R. & Santillan, A. Embolization and & Rosenwasser, R. H. Combining stereotactic
analysis and comparison with stereotactic radiosurgery. radiosurgery for arteriovenous malformations. Surg. angiography and 3D time‑of‑flight magnetic resonance
J. Neurosurg. 88, 641–646 (1998). Neurol. Int. 3, S90–S104 (2012). angiography in treatment planning for arteriovenous
106. Schaller, C. & Schramm, J. Microsurgical results for 129. Pollock, B. E., Flickinger, J. C., Lunsford, L. D., Maitz, A. malformation radiosurgery. Int. J. Radiat. Oncol.
small arteriovenous malformations accessible for & Kondziolka, D. Factors associated with successful Biol. Phys. 46, 1149–1154 (2000).
radiosurgical or embolization treatment. Neurosurgery arteriovenous malformation radiosurgery. 150. Colombo, F. et al. Three-dimensional angiography
40, 664–672; discussion 672–674 (1997). Neurosurgery 42, 1239–1244; discussion for radiosurgical treatment planning for arteriovenous
107. Schaller, C., Schramm, J. & Haun, D. Significance of 1244–1247 (1998). malformations. J. Neurosurg. 98, 536–543 (2003).
factors contributing to surgical complications and to late This article demonstrates that analyses of 151. Hamm, K. D. et al. Special aspects of diagnostic
outcome after elective surgery of cerebral arteriovenous radiosurgical results lead to predictors of outcome imaging for radiosurgery of arteriovenous
malformations. J. Neurol. Neurosurg. Psychiatry 65, and grading systems that guide clinical malformations. Neurosurgery 62, A44–A52;
547–554 (1998). decision-making. discussion A52 (2008).
NATURE REVIEWS | DISEASE PRIMERS VOLUME 1 | 2015 | 19
© 2015 Macmillan Publishers Limited. All rights reserved
PRIMER
152. Flickinger, J. C., Kano, H., Niranjan, A., Kondziolka, D. 175. Miyawaki, L. et al. Five year results of LINAC 195. van Beijnum, J. et al. Treatment of brain arteriovenous
& Lunsford, L. D. Dose selection in stereotactic radiosurgery for arteriovenous malformations: malformations: a systematic review and meta-analysis.
radiosurgery. Prog. Neurol. Surg. 27, 49–57 (2013). outcome for large AVMS. Int. J. Radiat. Oncol. JAMA 306, 2011–2019 (2011).
153. Boothe, D. et al. Bevacizumab as a treatment for Biol. Phys. 44, 1089–1106 (1999). This meta-analysis compiled data comparing
radiation necrosis of brain metastases post stereotactic 176. Ogilvy, C. S. et al. AHA Scientific Statement: the morbidity, mortality and efficacy of surgery,
radiosurgery. Neuro Oncol. 15, 1257–1263 (2013). recommendations for the management of intracranial radiosurgery and endovascular embolization
154. Alexander, M. J. & Tolbert, M. E. Targeting cerebral arteriovenous malformations: a statement for in more than 13,000 patients.
arteriovenous malformations for minimally invasive healthcare professionals from a special writing group 196. Gross, B. A. & Du, R. Hemorrhage from arteriovenous
therapy. Neurosurgery 59, S178–183; discussion of the Stroke Council, American Stroke Association. malformations during pregnancy. Neurosurgery 71,
S3–S13 (2006). Stroke 32, 1458–1471 (2001). 349–355; discussion 355–356 (2012).
155. Bollet, M. A. et al. Efficacy and morbidity of arc-therapy This article summarizes management 197. Bateman, B. T. et al. Intracerebral hemorrhage
radiosurgery for cerebral arteriovenous malformations: recommendations for brain arteriovenous in pregnancy: frequency, risk factors, and outcome.
a comparison with the natural history. Int. J. Radiat. malformations from a panel of experts. Neurology 67, 424–429 (2006).
Oncol. Biol. Phys. 58, 1353–1363 (2004). 177. Pan, H. C., Sheehan, J., Stroila, M., Steiner, M. & 198. Horton, J. C., Chambers, W. A., Lyons, S. L.,
156. Chang, S. D. et al. Multimodality treatment of giant Steiner, L. Late cyst formation following Gamma Knife Adams, R. D. & Kjellberg, R. N. Pregnancy and
intracranial arteriovenous malformations. Neurosurgery surgery of arteriovenous malformations. J. Neurosurg. the risk of hemorrhage from cerebral arteriovenous
53, 1–11; discussion 11–13 (2003). 102 (Suppl.), 124–127 (2005). malformations. Neurosurgery 27, 867–871;
157. Dawson, R. C. et al. Treatment of arteriovenous 178. Paulsen, R. D., Steinberg, G. K., Norbash, A. M., discussion 871–872 (1990).
malformations of the brain with combined embolization Marcellus, M. L. & Marks, M. P. Embolization of basal 199. Lawton, M. T. et al. Radiation arteriopathy in the
and stereotactic radiosurgery: results after 1 and ganglia and thalamic arteriovenous malformations. transgenic arteriovenous fistula model. Neurosurgery
2 years. AJNR Am. J. Neuroradiol. 11, 857–864 Neurosurgery 44, 991–996; discussion 996–997 62, 1129–1138; discussion 138–139 (2008).
(1990). (1999). 200. Walker, E. J. et al. Arteriovenous malformation in
158. Deruty, R., Pelissou-Guyotat, I., Morel, C., 179. Sinclair, J., Kelly, M. E. & Steinberg, G. K. Surgical the adult mouse brain resembling the human disease.
Bascoulergue, Y. & Turjman, F. Reflections on the management of posterior fossa arteriovenous Ann. Neurol. 69, 954–962 (2011).
management of cerebral arteriovenous malformations. malformations. Neurosurgery 58 (Suppl. 2), This experimental model for brain arteriovenous
Surg. Neurol. 50, 245–255; discussion 255–256 ONS‑189–201; discussion ONS–201 (2006). malformations was the first of its kind and provided
(1998). 180. Andrade-Souza, Y. M. et al. Liquid embolisation a method for the pathogenesis and regression of
159. Deruty, R., Pelissou-Guyotat, I., Mottolese, C., material reduces the delivered radiation dose: a this condition.
Bascoulergue, Y. & Amat, D. The combined management physical experiment. Acta Neurochir. 150, 161–164; 201. Han, C. et al. VEGF neutralization can prevent and
of cerebral arteriovenous malformations. Experience discussion 164 (2008). normalize arteriovenous malformations in an animal
with 100 cases and review of the literature. 181. Miyamoto, S. et al. Posttreatment sequelae of model for hereditary hemorrhagic telangiectasia 2.
Acta Neurochir. 123, 101–112 (1993). palliatively treated cerebral arteriovenous Angiogenesis 14, 823–830 (2014).
160. Fiorella, D., Albuquerque, F. C., Woo, H. H., malformations. Neurosurgery 46, 589–594; 202. Frenzel, T. et al. Feasibility of minocycline and
McDougall, C. G. & Rasmussen, P. A. The role of discussion 594–595 (2000). doxycycline use as potential vasculostatic therapy for
neuroendovascular therapy for the treatment of brain 182. Morgan, M. K., Patel, N. J., Simons, M., Ritson, E. A. brain vascular malformations: pilot study of adverse
arteriovenous malformations. Neurosurgery 59, & Heller, G. Z. Influence of the combination of patient events and tolerance. Cerebrovasc. Dis. 25, 157–163
S163–S177; discussion S3–13 (2006). age and deep venous drainage on brain arteriovenous (2008).
161. Gobin, Y. P. et al. Treatment of brain arteriovenous malformation recurrence after surgery. J. Neurosurg. This study demonstrated that brain arteriovenous
malformations by embolization and radiosurgery. 117, 934–941 (2012). malformations might be stabilized and
J. Neurosurg. 85, 19–28 (1996). 183. Abla, A. A. et al. A treatment paradigm for high-grade haemorrhage rates reduced with medical therapy.
162. Guo, W. Y. et al. Combined embolization and Gamma brain arteriovenous malformations: volume-staged 203. Hashimoto, T., Matsumoto, M. M., Li, J. F.,
Knife radiosurgery for cerebral arteriovenous radiosurgical downgrading followed by microsurgical Lawton, M. T. & Young, W. L. Suppression of MMP‑9
malformations. Acta Radiol. 34, 600–606 (1993). resection. J. Neurosurg. 122, 419–432 (2015). by doxycycline in brain arteriovenous malformations.
163. Haw, C. S., terBrugge, K., Willinsky, R. & Tomlinson, G. 184. Rutledge, W. C. et al. Treatment and outcomes BMC Neurol. 5, 1 (2005).
Complications of embolization of arteriovenous of ARUBA-eligible patients with unruptured brain 204. Feliciano, C. E. et al. Provocative test with propofol:
malformations of the brain. J. Neurosurg. 104, arteriovenous malformations at a single institution. experience in patients with cerebral arteriovenous
226–232 (2006). Neurosurg. Focus 37, E8 (2014). malformations who underwent neuroendovascular
164. Henkes, H. et al. Endovascular therapy of brain AVMs 185. Stapf, C., Parides, M. K., Moskowitz, A. J. & Mohr, J. P. procedures. AJNR Am. J. Neuroradiol. 31, 470–475
prior to radiosurgery. Neurol. Res. 20, 479–492 Management of brain arteriovenous malformations (2010).
(1998). — authors’ reply. Lancet 383, 1635–1636 (2014). 205. Starke, R. M. et al. Adjuvant embolization with N‑butyl
165. Killer, M. et al. Radiosurgery following embolisation and/ 186. Han, P. P., Ponce, F. A. & Spetzler, R. F. Intention- cyanoacrylate in the treatment of cerebral
or surgery of brain AVM’s. Interv. Neuroradiol. 2, 27–33 to‑treat analysis of Spetzler–Martin grades IV and V arteriovenous malformations: outcomes, complications,
(1996). arteriovenous malformations: natural history and and predictors of neurologic deficits. Stroke 40,
166. Mathis, J. A. et al. The efficacy of particulate treatment paradigm. J. Neurosurg. 98, 3–7 (2003). 2783–2790 (2009).
embolization combined with stereotactic radiosurgery 187. Dorman, P. J., Slattery, J., Farrell, B., Dennis, M. S. 206. Mann, K. M. et al. Sleeping Beauty mutagenesis
for treatment of large arteriovenous malformations of & Sandercock, P. A. A randomised comparison of reveals cooperating mutations and pathways in
the brain. AJNR Am. J. Neuroradiol. 16, 299–306 the EuroQol and Short Form‑36 after stroke. pancreatic adenocarcinoma. Proc. Natl Acad. Sci. USA
(1995). United Kingdom Collaborators in the International 109, 5934–5941 (2012).
167. Miyachi, S. et al. Embolization of arteriovenous Stroke Trial. BMJ 315, 461 (1997). 207. O’Hayre, M. et al. The emerging mutational landscape
malformations prior to radiosurgery. Interv. Neuroradiol. 188. Marshall, G. A., Jonker, B. P., Morgan, M. K. & of G proteins and G‑protein-coupled receptors in
6 (Suppl. 1), 131–137 (2000). Taylor, A. J. Prospective study of neuropsychological cancer. Nat. Rev. Cancer 13, 412–424 (2013).
168. Mizoi, K. et al. Multimodality treatment for large and psychosocial outcome following surgical excision 208. Forbes, S. A. et al. COSMIC: mining complete cancer
and critically located arteriovenous malformations. of intracerebral arteriovenous malformations. J. Clin. genomes in the Catalogue of Somatic Mutations in
Neurol. Med. Chir. 38 (Suppl.), 186–192 (1998). Neurosci. 10, 42–47 (2003). Cancer. Nucleic Acids Res. 39, D945–D950 (2011).
169. Soderman, M., Andersson, T., Karlsson, B., 189. Brown, R. D. Jr et al. The natural history of unruptured 209. Lawton, M. T. The role of AVM microsurgery in the
Wallace, M. C. & Edner, G. Management of patients intracranial arteriovenous malformations. aftermath of a randomized trial of unruptured brain
with brain arteriovenous malformations. Eur. J. Radiol. J. Neurosurg. 68, 352–357 (1988). arteriovenous malformations. AJNR Am.
46, 195–205 (2003). 190. Gross, B. A. & Du, R. Natural history of cerebral J. Neuroradiol. 36, 617–619 (2015).
170. Soderman, M., Rodesch, G., Karlsson, B., Lax, I. arteriovenous malformations: a meta-analysis.
& Lasjaunias, P. Gamma Knife outcome models as J. Neurosurg. 118, 437–443 (2013). Acknowledgements
a reference standard in the embolisation of cerebral References 189 and 190 provide reviews This primer cites research that was supported in part by US
arteriovenous malformations. Acta Neurochir. 143, of the natural history of brain arteriovenous National Institutes of Health grants: R01 NS034949 (H.K.)
801–810 (2001). malformations. and U54 NS065075 (M.T.L.). The Brain Vascular Malformation
171. Wikholm, G., Lundqvist, C. & Svendsen, P. The Goteborg 191. Bervini, D., Morgan, M. K., Ritson, E. A. & Heller, G. Consortium (U54NS065075) is part of the Rare Diseases
cohort of embolized cerebral arteriovenous Surgery for unruptured arteriovenous malformations Clinical Research Network (RDCRN), an initiative of the Office
malformations: a 6‑year follow‑up. Neurosurgery 49, of the brain is better than conservative management of Rare Diseases Research (ORDR) that is funded through
799–805; discussion 805–806 (2001). for selected cases: a prospective cohort study. co llaboration between National Center for Advancing
172. Andrade-Souza, Y. M. et al. Embolization before J. Neurosurg. 121, 878–890 (2014). Translational Sciences (NCATS) and the National Institute of
radiosurgery reduces the obliteration rate of 192. Choi, J. H. et al. Clinical outcome after first and Neurological Disorders and Stroke (NINDS).
arteriovenous malformations. Neurosurgery 60, recurrent hemorrhage in patients with untreated brain
443–451; discussion 451–452 (2007). arteriovenous malformation. Stroke 37, 1243–1247 Author contributions
173. Back, A. G., Vollmer, D., Zeck, O., Shkedy, C. & (2006). Introduction (M.T.L.); Epidemiology (W.C.R., H.K. and C.S.);
Shedden, P. M. Retrospective analysis of unstaged 193. Baranoski, J. F. et al. Seizure control for intracranial Mechanisms/pathophysiology (K.J.W., D.Y.L. and H.K.);
and staged Gamma Knife surgery with and without arteriovenous malformations is directly related to Diagnosis, screening and prevention (T.K. and K.T.B.);
preceding embolization for the treatment of treatment modality: a meta-analysis. J. Neurointerv. Management (M.T.L., T.K., K.T.B. and D.K.); Quality of life
arteriovenous malformations. J. Neurosurg. 109 Surg. 6, 684–690 (2014). (M.K.M.); Outlook (K.M., R.F.S., M.T.L. and H.K.); overview of
(Suppl.), 57–64 (2008). 194. Thorpe, M. L., Cordato, D. J., Morgan, M. K. & Primer (M.T.L.).
174. Kano, H. et al. Stereotactic radiosurgery for Herkes, G. K. Postoperative seizure outcome in a series
arteriovenous malformations after embolization: a case– of 114 patients with supratentorial arteriovenous Competing interests statement
control study. J. Neurosurg. 117, 265–275 (2012). malformations. J. Clin. Neurosci. 7, 107–111 (2000). The authors declare no competing interests.
20 | 2015 | VOLUME 1 www.nature.com/nrdp
© 2015 Macmillan Publishers Limited. All rights reserved
You might also like
- Vascular Malformations: A Review: Joshua A. Cox, MD Erica Bartlett, MD Edward I. Lee, MDDocument6 pagesVascular Malformations: A Review: Joshua A. Cox, MD Erica Bartlett, MD Edward I. Lee, MDYusmiatiNo ratings yet
- Management of Unruptured Intracranial Aneurysms: Neurology Clinical PracticeDocument10 pagesManagement of Unruptured Intracranial Aneurysms: Neurology Clinical PracticeEddwwin Varillas ReyesNo ratings yet
- Aneurysmal Subarachnoid Hemorrhage.6Document19 pagesAneurysmal Subarachnoid Hemorrhage.6Aldy Setiawan PutraNo ratings yet
- Cerebral AneurysmsDocument12 pagesCerebral AneurysmsDyah Ayu Puspita AnggarsariNo ratings yet
- Cerebral Venous ThrombosisDocument14 pagesCerebral Venous ThrombosisSrinivas PingaliNo ratings yet
- Unruptured Intracranial Aneurysms: Robert D. Brown, JR., M.D., M.P.HDocument8 pagesUnruptured Intracranial Aneurysms: Robert D. Brown, JR., M.D., M.P.HtonnyprogramadorNo ratings yet
- Ajiboye 2015Document11 pagesAjiboye 2015editingjuryNo ratings yet
- Art 7Document5 pagesArt 7miguelNo ratings yet
- 2017 HSA Clinical PracticeDocument10 pages2017 HSA Clinical PracticeAndrea MartinezNo ratings yet
- AVM CnsDocument31 pagesAVM CnsGamma KnifeNo ratings yet
- CA Coil ClipDocument12 pagesCA Coil ClipArdiansyah P PratamaNo ratings yet
- Rutman Et Al 2022 Incidental Vascular Findings On Brain Magnetic Resonance AngiographyDocument13 pagesRutman Et Al 2022 Incidental Vascular Findings On Brain Magnetic Resonance AngiographySofía ValdésNo ratings yet
- Subarachnoid HemorrhageDocument10 pagesSubarachnoid HemorrhageRoberto López Mata100% (1)
- Risk of Hemorrhage in Patients With Untreated SM Grade IV and V AVMsDocument7 pagesRisk of Hemorrhage in Patients With Untreated SM Grade IV and V AVMsKashifNo ratings yet
- Stroke Prevention and Treatment in Sickle Cell Disease: Robert J. Adams, MS, MDDocument4 pagesStroke Prevention and Treatment in Sickle Cell Disease: Robert J. Adams, MS, MDMeshaki MbarukaNo ratings yet
- Update Managemant Unrupture Aneurysm 2018Document8 pagesUpdate Managemant Unrupture Aneurysm 2018Mikha ManurungNo ratings yet
- Scientific Report Journal 22 NovDocument6 pagesScientific Report Journal 22 Novnaresh kotraNo ratings yet
- Congenital Heart Disease: Transvenous Pacing Leads and Systemic Thromboemboli in Patients With Intracardiac ShuntsDocument7 pagesCongenital Heart Disease: Transvenous Pacing Leads and Systemic Thromboemboli in Patients With Intracardiac Shuntsdenydeniche388No ratings yet
- 10.1136@jnnp 2020 324418Document7 pages10.1136@jnnp 2020 324418RAFAEL BRITONo ratings yet
- Brain Metastases: Review ArticleDocument17 pagesBrain Metastases: Review ArticleSebastianNo ratings yet
- Visualizing Cerebral Small Vessel Degeneration During Aging and Diseases Using2Document15 pagesVisualizing Cerebral Small Vessel Degeneration During Aging and Diseases Using2Sofía ValdésNo ratings yet
- Stroke NarrativeDocument10 pagesStroke Narrativecfalcon.medicinaNo ratings yet
- Int J Stroke 2014 Benavente 1057 64Document8 pagesInt J Stroke 2014 Benavente 1057 64Fauzan IndraNo ratings yet
- Cerebral Venous Thrombosis: A Comprehensive Review: Clinical Neurology: Review ArticleDocument11 pagesCerebral Venous Thrombosis: A Comprehensive Review: Clinical Neurology: Review Articledanby danbyNo ratings yet
- Monika Fleckenstein Age Related Macular Degeneration ADocument11 pagesMonika Fleckenstein Age Related Macular Degeneration Afrwf8j7dr4No ratings yet
- Acv PDFDocument14 pagesAcv PDFFelipe AlcainoNo ratings yet
- Seminar: Daniel J Penny, G Wesley Vick IIIDocument10 pagesSeminar: Daniel J Penny, G Wesley Vick IIIMuhammadAldoGiansyahNo ratings yet
- Review ArticleDocument8 pagesReview ArticleOctavianmdNo ratings yet
- Cryptogenic Stroke: Clinical PracticeDocument10 pagesCryptogenic Stroke: Clinical PracticenellieauthorNo ratings yet
- Neurologic Disorders Associated With Mitral Valve ProlapseDocument6 pagesNeurologic Disorders Associated With Mitral Valve Prolapsegeorgiana_884431330No ratings yet
- Intracerebral Haemorrhage: Disease PrimersDocument18 pagesIntracerebral Haemorrhage: Disease PrimersMarlon VillanuevaNo ratings yet
- 0003319715605977Document7 pages0003319715605977Jose Manuel Ornelas-AguirreNo ratings yet
- Cryptogenic Stroke 2016Document10 pagesCryptogenic Stroke 2016tatukyNo ratings yet
- Percutaneous SclerotherapyDocument11 pagesPercutaneous SclerotherapyVictorMattathiasNoliTjakrapawiraNo ratings yet
- Vascular Instability and Neurological Morbidity in Sickle Cell Disease: An Integrative Framework.Document21 pagesVascular Instability and Neurological Morbidity in Sickle Cell Disease: An Integrative Framework.Arturo Martí-CarvajalNo ratings yet
- Arterial Embolisms and Thrombosis in Upper Extremity IschemiaDocument10 pagesArterial Embolisms and Thrombosis in Upper Extremity IschemiaDede MarizalNo ratings yet
- Heritability of Mitral Regurgitation: Original ArticleDocument8 pagesHeritability of Mitral Regurgitation: Original ArticleLopis Cristian RenyaanNo ratings yet
- Chelliah2019 Article CardiovascularCTInCyanoticCong 210913 062234Document14 pagesChelliah2019 Article CardiovascularCTInCyanoticCong 210913 062234Rika PutriNo ratings yet
- Chelliah2019 Article CardiovascularCTInCyanoticCong 210913 062234Document14 pagesChelliah2019 Article CardiovascularCTInCyanoticCong 210913 062234Rika PutriNo ratings yet
- Point: How Do I Manage A Suspected Oral Vascular Malformation?Document3 pagesPoint: How Do I Manage A Suspected Oral Vascular Malformation?Luis Mesicano QuipeNo ratings yet
- J Jacc 2022 09 044Document17 pagesJ Jacc 2022 09 044Ivan BitunjacNo ratings yet
- Primer: Abdominal Aortic AneurysmsDocument22 pagesPrimer: Abdominal Aortic AneurysmsBeatriz Jaramillo ZaramaNo ratings yet
- Aneurysmal Subarachnoid Hemorrhage: Review ArticleDocument10 pagesAneurysmal Subarachnoid Hemorrhage: Review ArticlekucingkucingNo ratings yet
- Neuroint 2018 01011Document11 pagesNeuroint 2018 01011AnnetNo ratings yet
- LMOSMOOSMMOAMINISNKDocument16 pagesLMOSMOOSMMOAMINISNKRafaelNo ratings yet
- Oncologic Emergencies in The Head and NeckDocument20 pagesOncologic Emergencies in The Head and NeckEduardo FrancoNo ratings yet
- Cancer Stem Cells: To The EditorDocument4 pagesCancer Stem Cells: To The Editormira ariantiNo ratings yet
- Natural History of Arteriovenous Malformations - Presentation, Risk of Hemorrhage and MortalityDocument5 pagesNatural History of Arteriovenous Malformations - Presentation, Risk of Hemorrhage and MortalityKashifNo ratings yet
- Pi Is 0003497505012002Document5 pagesPi Is 0003497505012002Tri RachmadijantoNo ratings yet
- Genetics of Hemangiomas, Vascular Malformations, and Primary LymphedemDocument7 pagesGenetics of Hemangiomas, Vascular Malformations, and Primary LymphedemMiradz 'demmy' MuhidinNo ratings yet
- Thick and Diffuse Cisternal Clot Independently Predicts Vasospasm-Related Morbidity and Poor Outcome After Aneurysmal Subarachnoid HemorrhageDocument9 pagesThick and Diffuse Cisternal Clot Independently Predicts Vasospasm-Related Morbidity and Poor Outcome After Aneurysmal Subarachnoid HemorrhageVanessa LandaNo ratings yet
- Cervicofacial Vascular Anomalies. I. Hemangiomas and Other Benign Vascular TumorsDocument9 pagesCervicofacial Vascular Anomalies. I. Hemangiomas and Other Benign Vascular TumorsBikash ShresthaNo ratings yet
- Management of No-Re Ow Phenomenon in The Catheterization LaboratoryDocument9 pagesManagement of No-Re Ow Phenomenon in The Catheterization LaboratoryRajendra ChavanNo ratings yet
- Practneurol 2020 002763Document12 pagesPractneurol 2020 002763Fitri ainun MalahayatiNo ratings yet
- Clinical Manifestations, Prevention and Treatment of Stroke in WomenDocument6 pagesClinical Manifestations, Prevention and Treatment of Stroke in WomenCentral Asian StudiesNo ratings yet
- CCR 8 152Document6 pagesCCR 8 152ekafithraNo ratings yet
- Ictus en Joven Ferro2010Document12 pagesIctus en Joven Ferro2010Mez RealNo ratings yet
- Microcirculation in Cardiovascular DiseasesFrom EverandMicrocirculation in Cardiovascular DiseasesEnrico Agabiti-RoseiNo ratings yet
- Imaging in Peripheral Arterial Disease: Clinical and Research ApplicationsFrom EverandImaging in Peripheral Arterial Disease: Clinical and Research ApplicationsNo ratings yet
- MenopauseDocument3 pagesMenopauseTony NgNo ratings yet
- Prenatal Screening and DiagnosisDocument4 pagesPrenatal Screening and DiagnosisTony NgNo ratings yet
- Lactation MCQDocument5 pagesLactation MCQTony NgNo ratings yet
- Pelvi Abdominal MassesDocument5 pagesPelvi Abdominal MassesTony NgNo ratings yet
- Unplanned PregnancyDocument4 pagesUnplanned PregnancyTony NgNo ratings yet
- Postcoital and Post-Menopausal BleedingDocument4 pagesPostcoital and Post-Menopausal BleedingTony NgNo ratings yet
- Normal Labour and PuerperiumDocument3 pagesNormal Labour and PuerperiumTony NgNo ratings yet
- Intro To Obstetrics and Routine Antenatal CareDocument3 pagesIntro To Obstetrics and Routine Antenatal CareTony NgNo ratings yet
- InfertilityDocument4 pagesInfertilityTony NgNo ratings yet
- Streptococcus Mitis Expressing Pneumococcal Serotype 1 Capsule - 2018 Nature ResearchDocument9 pagesStreptococcus Mitis Expressing Pneumococcal Serotype 1 Capsule - 2018 Nature ResearchTony NgNo ratings yet
- Pain and Bleeding in Early PregnancyDocument7 pagesPain and Bleeding in Early PregnancyTony NgNo ratings yet
- Induction of Labour and Abnormal Labour ProgressDocument3 pagesInduction of Labour and Abnormal Labour ProgressTony NgNo ratings yet
- Career Symposium Aug 2020 Schedule - Program Outline - 18 JulyDocument4 pagesCareer Symposium Aug 2020 Schedule - Program Outline - 18 JulyTony NgNo ratings yet
- Iron HomeostasisDocument30 pagesIron HomeostasisTony NgNo ratings yet
- Within-Host Microevolution of Streptococcus Pneumoniae Is Rapid and Adaptive During Natural Colonisation - 2020 Nature ResearchDocument14 pagesWithin-Host Microevolution of Streptococcus Pneumoniae Is Rapid and Adaptive During Natural Colonisation - 2020 Nature ResearchTony NgNo ratings yet
- Designing Ecologically Optimized Pneumococcal Vaccines Using Population Genomics - 2020 Nature ResearchDocument25 pagesDesigning Ecologically Optimized Pneumococcal Vaccines Using Population Genomics - 2020 Nature ResearchTony NgNo ratings yet
- Allelic Variation of The Capsule Promoter Diversifies Encapsulation and Virulence in Streptococcus Pneumoniae - 2016 Nature ResearchDocument17 pagesAllelic Variation of The Capsule Promoter Diversifies Encapsulation and Virulence in Streptococcus Pneumoniae - 2016 Nature ResearchTony NgNo ratings yet
- Animal Models of Streptococcus Pneumoniae Disease - 2008 AMR American Society For MicrobiologyDocument20 pagesAnimal Models of Streptococcus Pneumoniae Disease - 2008 AMR American Society For MicrobiologyTony NgNo ratings yet
- The Post-Vaccine Microevolution of Invasive Streptococcus Pneumoniae - 2015 Nature ResearchDocument8 pagesThe Post-Vaccine Microevolution of Invasive Streptococcus Pneumoniae - 2015 Nature ResearchTony NgNo ratings yet
- Adenylate Kinase Potentiates The Capsular Polysaccharide by Modulating Cps2D in Streptococcus Pneumoniae D39 - 2018 Nature ResearchDocument14 pagesAdenylate Kinase Potentiates The Capsular Polysaccharide by Modulating Cps2D in Streptococcus Pneumoniae D39 - 2018 Nature ResearchTony NgNo ratings yet
- Protection Against Streptococcus Pneumoniae Lung Infection After Nasopharyngeal Colonization Requires Both Humoral and Cellular Immune ResponsesDocument13 pagesProtection Against Streptococcus Pneumoniae Lung Infection After Nasopharyngeal Colonization Requires Both Humoral and Cellular Immune ResponsesGufron MustofaNo ratings yet
- CPSR, A GNTR Family Regulator, Transcriptionally Regulates Capsular Polysaccharide Biosynthesis and Governs Bacterial Virulence inDocument12 pagesCPSR, A GNTR Family Regulator, Transcriptionally Regulates Capsular Polysaccharide Biosynthesis and Governs Bacterial Virulence inTony NgNo ratings yet
- Bacterial Meningitis. Nature Review 2016Document20 pagesBacterial Meningitis. Nature Review 2016Caleb RojasNo ratings yet
- RGG-SHP Regulators Are Important For Pneumococcal Colonization and Invasion Through Their Effect On Mannose Utilization and Capsule SynthesisDocument15 pagesRGG-SHP Regulators Are Important For Pneumococcal Colonization and Invasion Through Their Effect On Mannose Utilization and Capsule SynthesisTony NgNo ratings yet
- Bacterial Polymers Biosynthesis, Modifications and Applications - 2010 Nature ReviewDocument15 pagesBacterial Polymers Biosynthesis, Modifications and Applications - 2010 Nature ReviewTony NgNo ratings yet
- Reading1.3 2 4 Theory at A Glance 2005 WMLDocument60 pagesReading1.3 2 4 Theory at A Glance 2005 WMLTony NgNo ratings yet
- A Semisynthetic Carbohydrate-Lipid Vaccine That Protects Against S. Pneumoniae in Mice - 2014 Nature ResearchDocument9 pagesA Semisynthetic Carbohydrate-Lipid Vaccine That Protects Against S. Pneumoniae in Mice - 2014 Nature ResearchTony NgNo ratings yet
- Professional IdentitiyDocument12 pagesProfessional IdentitiycelNo ratings yet
- M1 Anatomy Tutorial - Muscles of The Upper Limb (David)Document8 pagesM1 Anatomy Tutorial - Muscles of The Upper Limb (David)Tony NgNo ratings yet
- M1 Anatomy Tutorial - Muscles of The Lower Limb (David)Document6 pagesM1 Anatomy Tutorial - Muscles of The Lower Limb (David)Tony NgNo ratings yet
- Anaphy ReviewerDocument102 pagesAnaphy Reviewermaureensolano63No ratings yet
- HydragenaeDocument4 pagesHydragenaeArmonNo ratings yet
- Assess Lower Extremities HealthDocument253 pagesAssess Lower Extremities Healthseph bron100% (1)
- Life Processes NotesDocument22 pagesLife Processes NotesHarshit bhaveNo ratings yet
- 11.1 Multiple Choice Part I Questions: Chapter 11 The Cardiovascular SystemDocument33 pages11.1 Multiple Choice Part I Questions: Chapter 11 The Cardiovascular SystemmuryumNo ratings yet
- TRANSCALLOSAL TRANSCHOROIDAL APPROACH TO Third VentriclDocument6 pagesTRANSCALLOSAL TRANSCHOROIDAL APPROACH TO Third VentriclNikolay PeevNo ratings yet
- Evolve Resources For Illustrated Anatomy of The Head and Neck 5th Edition Fehrenbach Test BankDocument17 pagesEvolve Resources For Illustrated Anatomy of The Head and Neck 5th Edition Fehrenbach Test Bankjoshuabowmanymctpnejsw100% (29)
- Heart Failure Clinical Presentation - History, Physical Examination, Predominant Right-Sided Heart FailureDocument12 pagesHeart Failure Clinical Presentation - History, Physical Examination, Predominant Right-Sided Heart FailureAshutosh SinghNo ratings yet
- Anatomy of The LiverDocument5 pagesAnatomy of The LiverAioanei Octavian100% (1)
- 2.4 Circulatory SystemDocument8 pages2.4 Circulatory SystemUdesh RajNo ratings yet
- Science Primary 5 Second Term 2015 Worksheetمراجعة نهائية علوم لغات الصف الخامس الابتدائي الترم الثانيDocument16 pagesScience Primary 5 Second Term 2015 Worksheetمراجعة نهائية علوم لغات الصف الخامس الابتدائي الترم الثانيrabei100% (8)
- Margi KC Amavata 2Document54 pagesMargi KC Amavata 2hetvi.m.patel.1999No ratings yet
- Deep Vein ThrombosisDocument33 pagesDeep Vein ThrombosisWisnu Cahyo100% (1)
- Standardised Inotrope and Vasopressor Guidelines - Learning Package FINALDocument30 pagesStandardised Inotrope and Vasopressor Guidelines - Learning Package FINALInês MendonçaNo ratings yet
- Science 9 TG Draft 4.29.2014Document406 pagesScience 9 TG Draft 4.29.2014astherielleNo ratings yet
- Deep Venous ThrombosisDocument28 pagesDeep Venous ThrombosisJavier CubillosNo ratings yet
- The Circulatory System of Fish Is Quite SimpleDocument3 pagesThe Circulatory System of Fish Is Quite SimpleEarl John Fajarito RafaelNo ratings yet
- Angeles University Foundation Nursing Program Details Pregnancy HypertensionDocument31 pagesAngeles University Foundation Nursing Program Details Pregnancy HypertensionMylene Angelie Bognot100% (2)
- Chronic Venous Insufficiency: Causes, Symptoms, Diagnosis and TreatmentDocument40 pagesChronic Venous Insufficiency: Causes, Symptoms, Diagnosis and TreatmentGihan NakhlehNo ratings yet
- BCS InterventionDocument14 pagesBCS InterventiondrrochanNo ratings yet
- Respiratory and Circulatory Systems WorksheetDocument7 pagesRespiratory and Circulatory Systems Worksheetar0411No ratings yet
- Biology-Igcse FULL NotesDocument63 pagesBiology-Igcse FULL NotesSameer Abu Munshar100% (5)
- The Structure and Function of the Human HeartDocument22 pagesThe Structure and Function of the Human HeartNunoAlmeidaNo ratings yet
- Acute Myocardial InfarctionDocument62 pagesAcute Myocardial InfarctionJohn Alvin YoroNo ratings yet
- Handbook of Clinical SkillsDocument56 pagesHandbook of Clinical SkillswiwienNo ratings yet
- Scientific Survey of The Yogic PosesDocument66 pagesScientific Survey of The Yogic PosesSnehal Kale100% (1)
- Chapter_005 Interdependent Body SystemsDocument46 pagesChapter_005 Interdependent Body SystemsTina VargheseNo ratings yet
- Deep Vein Thrombosis FlyerDocument2 pagesDeep Vein Thrombosis FlyerMuhammad Reza Syahli PiliangNo ratings yet
- 03 Soal Bahasa Inggris 2001 - 2009Document83 pages03 Soal Bahasa Inggris 2001 - 2009Afreza MalfiraNo ratings yet
- Cardio MechDocument84 pagesCardio MechTim LeeNo ratings yet