You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Reiki Symbols Infographic PDFDocument1 pageReiki Symbols Infographic PDFjasmeet100% (5)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Nursing Process SOAPIEDocument33 pagesNursing Process SOAPIEChoi Gong Ju100% (4)
- Rodulfo Final Thesis BookDocument204 pagesRodulfo Final Thesis BookPierre RodulfoNo ratings yet
- History of Acupuncture 2020723123350Document54 pagesHistory of Acupuncture 2020723123350Kavya MittalNo ratings yet
- Amaroli 15 YicDocument25 pagesAmaroli 15 Yicparvesh sangwanNo ratings yet
- Client Info FormDocument2 pagesClient Info FormkamalsalmanNo ratings yet
- Neurontin (Gabapentin)Document1 pageNeurontin (Gabapentin)E100% (3)
- Advanced Master's Degree in Endodontics, Periodontics and Oral SurgeryDocument62 pagesAdvanced Master's Degree in Endodontics, Periodontics and Oral SurgerySimona BudauNo ratings yet
- 6th July Flyer A4 - The Pillars and Biomechanical Concepts... El ZoghbiDocument1 page6th July Flyer A4 - The Pillars and Biomechanical Concepts... El ZoghbiSimona BudauNo ratings yet
- Advanced Occlusion Wax Up July 21Document11 pagesAdvanced Occlusion Wax Up July 21Simona BudauNo ratings yet
- Analysis of Radiographic Changes Associated With The Periradicular Diagnosis of Symptomatic Apical PeriodontitisDocument49 pagesAnalysis of Radiographic Changes Associated With The Periradicular Diagnosis of Symptomatic Apical PeriodontitisSimona BudauNo ratings yet
- Jida Feb March NMDocument53 pagesJida Feb March NMSimona BudauNo ratings yet
- Denticles of The Pulp ChamberDocument9 pagesDenticles of The Pulp ChamberSimona BudauNo ratings yet
- Lecture - Pulpal Pathology (Part 1 and 2) 4 YearDocument55 pagesLecture - Pulpal Pathology (Part 1 and 2) 4 YearSimona BudauNo ratings yet
- Sicat Endo Brochure 201 03 20 enDocument8 pagesSicat Endo Brochure 201 03 20 enSimona BudauNo ratings yet
- J Clinic Periodontology - 2020 - Issue InformationDocument3 pagesJ Clinic Periodontology - 2020 - Issue InformationSimona BudauNo ratings yet
- Brochure Impacted Wisdom Teeth Management Clinical CertificateDocument7 pagesBrochure Impacted Wisdom Teeth Management Clinical CertificateSimona BudauNo ratings yet
- Clinical Classification of The Status of The Pulp and Dental HealthDocument15 pagesClinical Classification of The Status of The Pulp and Dental HealthrahaazadNo ratings yet
- GEMS Course Brochure - 0Document8 pagesGEMS Course Brochure - 0Simona BudauNo ratings yet
- Current Guidelines For Schools Jan 22Document2 pagesCurrent Guidelines For Schools Jan 22Simona BudauNo ratings yet
- PIIS0161642015012671Document27 pagesPIIS0161642015012671Simona BudauNo ratings yet
- Writing Your Critical ReflectionDocument5 pagesWriting Your Critical ReflectionSimona BudauNo ratings yet
- Bone, Joints and Muscle InjuriesDocument35 pagesBone, Joints and Muscle InjuriesCdrrmc DigosNo ratings yet
- DR - Ziauddin A Kashmiri - Chest Tube Drainage-UpdatedDocument9 pagesDR - Ziauddin A Kashmiri - Chest Tube Drainage-UpdatedAli AftabNo ratings yet
- Aap Ki AntaraDocument22 pagesAap Ki AntaraChitrangada ChakrabortyNo ratings yet
- Upadacitinib AR SELECT NEXT TrialDocument10 pagesUpadacitinib AR SELECT NEXT TrialMr. LNo ratings yet
- 3PM PMTCT Indicator ReviewDocument5 pages3PM PMTCT Indicator ReviewJane GacheriNo ratings yet
- Hallux VarusDocument12 pagesHallux VarusZam PamateNo ratings yet
- Angelica M.docx LFD PharmacologysDocument2 pagesAngelica M.docx LFD PharmacologysAngelica Malacay RevilNo ratings yet
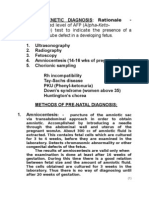
- Prenatal DiagnosisDocument5 pagesPrenatal Diagnosissarguss14No ratings yet
- Lesson Plan CaloriesDocument9 pagesLesson Plan Caloriesapi-353699297No ratings yet
- Mobility Programs For The Hospitalized Older Adult: A Scoping ReviewDocument18 pagesMobility Programs For The Hospitalized Older Adult: A Scoping ReviewArif GustyawanNo ratings yet
- Family Planning MethodDocument7 pagesFamily Planning MethodDebyang B ChangliNo ratings yet
- Introductions: Important Grammar RulesDocument11 pagesIntroductions: Important Grammar RulesyazzNo ratings yet
- Solo Protect Case Study - Healthcare at HomeDocument2 pagesSolo Protect Case Study - Healthcare at HomentapianNo ratings yet
- Jaanus' Optometrist - "Astigmatism Correction Is For Rare, Serious Cases" - Endmyopia®Document1 pageJaanus' Optometrist - "Astigmatism Correction Is For Rare, Serious Cases" - Endmyopia®Wil ScribdNo ratings yet
- Stages of GingivitisDocument42 pagesStages of Gingivitislia wardinaNo ratings yet
- Mysoline (Primidone) PIDocument2 pagesMysoline (Primidone) PIBrian HarrisNo ratings yet
- Constipation/ - Bian Bi: ConceptionDocument3 pagesConstipation/ - Bian Bi: Conceptionnaeem_k7No ratings yet
- Legal and Ethical Issues in PsychotherapyDocument69 pagesLegal and Ethical Issues in PsychotherapyRhea Andrea UyNo ratings yet
- Nail ExtractionDocument5 pagesNail ExtractionArip SeptadiNo ratings yet
- Adjuvant and Neoadjuvant ChemotherapyDocument22 pagesAdjuvant and Neoadjuvant Chemotherapyprabushankar7No ratings yet
- FitoterapiDocument8 pagesFitoterapiNetta JaneNo ratings yet
- Actinomycosis PPT Joel RuminantDocument20 pagesActinomycosis PPT Joel RuminantJoel Primavera100% (1)
- Hospital AdmissionDocument27 pagesHospital AdmissionHurley ReefNo ratings yet